Chorionic bump represents a rare abnormality of the gestational sac and, until now, there has been conflicting evidence related to its association with adverse perinatal outcomes. It appears as a bulge from the choriodecidual surface into the gestational sac which often decreases in size with time and rarely persists beyond the first trimester. Our case report presents and discusses a chorionic bump diagnosed early in pregnancy. After adequate counseling, the patient opted for termination of pregnancy; the embryonic karyotype was normal (46, XY). Taking into accoung the relative rarity of this entity, we review the available literature in order to raise awareness on this interesting sonographic finding.
OBSTETRICS
Chorionic bump în sarcina incipientă: un aspect ecografic inedit. Prezentare de caz şi review al literaturii
Chorionic bump at early stage of gestation: an interesting ultrasound finding. Case report and literature review
First published: 24 martie 2022
Editorial Group: MEDICHUB MEDIA
DOI: 10.26416/Gine.35.1.2022.6123
Abstract
Rezumat
Chorionic bump reprezintă o anomalie rară a sacului gestaţional, posibil asociată cu o serie de complicaţii perinatale. Aspectul sonografic este acela al unei formaţiuni protruzive în interiorul sacului gestaţional de la nivelul suprafeţei coriodeciduale ale cărei dimensiuni de obicei se reduc pe parcursul sarcinii, rareori persistând în trimestrul al treilea. În acest articol vom prezenta un caz diagnosticat precoce în sarcină cu chorionic bump. Pacienta a fost consiliată adecvat privind posibilele complicaţii obstetricale asociate acestui diagnostic, iar aceasta a decis întreruperea la cerere a cursului sarcinii. Testarea genetică a produsului de concepţie a evidenţiat un cariotip masculin normal (46, XY). Având în vederea raritatea acestui aspect ecografic, vom prezenta un review al datelor publicate până în prezent în literatura de specialitate referitoare la chorionic bump.
Introduction
A chorionic bump (CB), which was first reported by Harris et al. in 2006, has often been described as an irregular, convex bulge from the choriodecidual surface into the first-trimester gestational sac(1). It is tipically located within the thickest part of the developing placenta, chorion frondosum(2).
The incidence of CB is between 1.5 and 7 per 1000 pregnancies(3) and the viable pregnancy outcome rate is reported between less than 50% to 65% and even higher (83%) if the pregnancy is otherwise normal(4). The presence of CB on early first-trimester ultrasound increases threefold the risk of miscarriage and adverse pregnancy outcomes, making it an ultrasound marker that requires a close surveillance throughout the pregnancy to prevent the long-term complications and provide adequate counseling to the patient(5).
The most common sonographic findings of CB are a protrusion from the chorionic wall into the gestational sac, having a central hypoechoic region and a peripheral hyperechoic rim, with no vascularity; a less comon aspect is a hyperechoic protrusion with no vascularity(6).
The purpose of this paper is to present a case diagnosed with chorionic bump at early stage of gestation and to review the data available in literature regarding this entity and the perinatal outcomes of pregnancies associated with it.
Case presentation
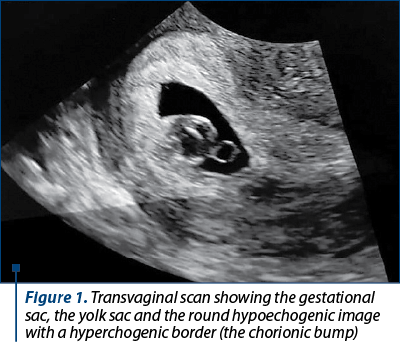
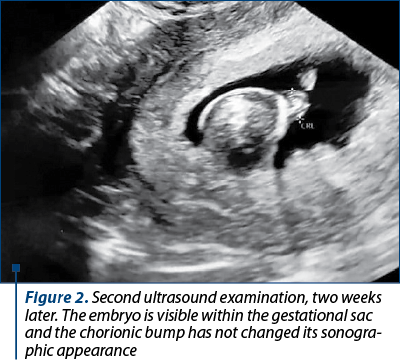
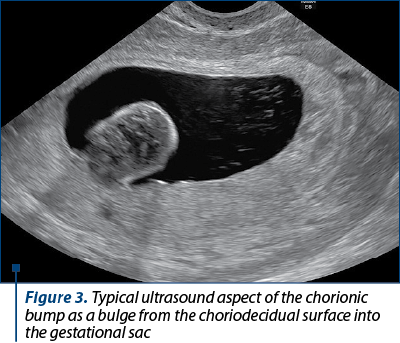
A 27-year-old Caucasian, gravida 1 (births 0, abortus 0), with 5 weeks and 2 days of amenorrhea and a positive urinary pregnancy test, presented in our department of fetal medicine for an early scan. The pregnancy was spontaneous and planned. The patient’s medical history was uneventful. The transvaginal ultrasound examination revealed an unique intrauterine gestational sac, the yolk sac and a round hypoechogenic image with a hyperchogenic border withing the gestational sac measuring 1.4/1.3 cm (Figure 1). Upon color and power Doppler examination, no vascular flow was detected. The seric concentration of free beta-HCG was 107,516.99 mUI/mL. The patient was rescanned after two weeks and a live embryo became visible with a CRL of 9.9 mm (corresponding to 7 weeks and 1 day). The sonographic appearance and size of the echogenic mass remained unchanged (Figures 2 and 3). We established that the diagnosis was a chorionic bump and the patient was counseled on the available data existing in literature regarding this obstetric complication. The patient opted for surgical termination of pregnancy (dilatation and curettage) and the embryonic karyotype came back normal (46, XY). The patient was discharged and is currently attempting to conceive again.
Discussion
Chorionic bump is a rare condition usually diagnosed in the first trimester of pregnancy as a bulge from the choriodecidual surface into the gestational sac. It often decreases in size with time and rarely persists beyond the first trimester(7), although a recent case has been described being diagnosed in the third trimester(3).
The clinical significance and etiology of the CB remain unclear. The existing data hypothesize that the CB might be a hematoma, which has been consistently supported by sonographic findings and histopathological analysis(6). Baalman et al. were of the opinion that the mechanism behind chorionic bumps was the extensive necrosis of the decidualized endometrium(8).
While some authors suggest that a chorionic bump detected during the 11-week to 13-week scan is a transient, incidental finding with probably no relevant clinical significance(9), a recent systematic review and meta-analysis which included 173 pregnant women with CB and 1263 pregnant women without CB (control group) showed that the presence of CB at the first-trimester ultrasound significantly increased the risk of miscarriage and adverse pregnancy outcomes and reduced the rate of live newborns(5). After presenting all this information to our patient, she decided to terminate the pregnancy, in consequence we were unable to make any comments regarding the pregnancy outcome.
Another recent paper published by Lu et al. revealed that an increased incidence of chorionic bump was observed in patients with intrauterine operations and/or adverse maternal history. The early detection of CB, bigger relative size and multiple lesions are factors likely to be associated with poorer pregnancy outcomes(10).
Wax et al. demonstrated in their study that a sonographically isolated CB is associated with a significantly increased likelihood of aneuploidy in high-risk fetuses(11). Two pregnancies having CB were subsequently diagnosed with complete mole and trisomy 18, respectively, and the authors hypothesized that placental pathology (including edema and hydropic villi) may contribute to or cause the ultrasound findings of some CB(12).
The coexistence of neural tube defects (acrania) and CB was reported and this association was potentially attributed to folate deficiency(13). In our case, the patient opted for karyotype of the embryo and, thus, aneuploidy was excluded. There is no specific management or guidelines for pregnancies diagnosed with CB and it remains unclear whether there is an intervention that might reduce the risk of miscarriage in affected patients(6). Due to the associated risk of poor obstetric outcome, these cases should be followed-up with serial ultrasound examinations throughout the pregnancy(14).
Conclusions
We presented in our paper a case of chorionic bump diagnosed sonographically early in pregnancy and also the newest data published on this relatively rare condition. The clinical inference is that CB on first-trimester sonography does not guarantee a secure prediction and it is important to consider it as an ultrasound marker that requires close surveillance throughout pregnancy in order to prevent complications and be able to provide adequate couseling to the patients.
Conflict of interests: The authors declare no conflict of interests.
Bibliografie
- Harris RD, Couto C, Karpovsky C, Blanchette Porter MM, Ouhilal S. The chorionic bump: A first-trimester pregnancy sonographic finding with a guarded prognosis. J Ultrasound Med. 2006;25(6):757-63.
- Sana Y, Appiah A, Davison A, Nicolaides KH, Johns J, Ross JA. Clinical significance of first-trimester chorionic bumps: a matched case-control study. Ultrasound Obstet Gynecol. 2013;42(5):585-9.
- Mirghani MH, Wadhwa N, Jahangir F, Abdel Hak OW, Uppal S. Case report: chorionic bump detected in the third trimester. J Clin Ultrasound. 2022;50(1):82-5.
- Younesi L, Shahnazari R. Chorionic bump in first-trimester sonography. J Med Ultrasound. 2017;25(4):221-6.
- Vena F, Bartolone M, D’Ambrosio V, et al. Pregnancy and perinatal outcomes in pregnancy with diagnosis of chorionic bump on first-trimester sonography: a systematic review and meta-analysis. J Matern Fetal Neonatal Med. 2021 Nov 22;1-8.
- Yousaf A, Tayyab A, Anil MSU, et al. Chorionic bump: radiologic features and pregnancy outcomes. Cureus. 2020;12(11):e11480.
- Carvalho RS, Osorio M, Brito C, Valente F. Chorionic bump in a pregnant patient with a history of infertility. BMJ Case Rep. 2018:bcr2018225091.
- Baalmann CG, Galgano SJ, Pietryga JA, Novak L, Robbin ML. A case of a chorionic bump: new sonographic-histopathologic findings with review of the literature.
- J Ultrasound Med. 2017;36:1968-70.
- Sepulveda W. Chorionic bump at 11 to 13 weeks’ gestation: prevalence and clinical significance. Prenat Diagn. 2019;39(6):471-6.
- Lu Yu, Wu Y, Huang F, Ren M. A single-center retrospective study of the clinical significance of chorionic bump at early stage of gestation. Am J Reprod Immunol. 2021;85(3):e13346.
- Wax JR, Cartin A, Litton C, Pinette MG, Lucas FL. First-trimester chorionic bump –
- association with fetal aneuploidy in a high-risk population. J Clin Ultrasound. 2017;45(1):3-7.
- Wax JR, Blaszyk H, Jones M, Cartin A, Pinette MG. The chorionic bump: etiologic insights from two pathologic pregnancies. J Clin Ultrasound. 2016;44(7):452-4.
- Wegrzyn P, Brawura-Biskupski-Samaha R, Borowski D, Gorski A, Wielgos M. The
- chorionic bump associated with acrania – case report. Ginekol Pol. 2013;84(12):1055-8.
- Tan ST, Ipek A, Sivaslioglu A, et al. The chorionic bump: radiologic and pathologic correlation. J Clin Ultrasound. 2011;39:35-7.
Articole din ediţiile anterioare
OBSTETRICS | Ediţia 2 36 / 2022
Dificultăţi de examinare ecografică la gravidele supraponderale. Studiu retrospectiv şi analiza literaturii
Răzvan Socolov, Mona Akad, Roxana Covali, Ioana Shadye-Scripcariu, Demetra Socolov, Dragoş Crauciuc, Eduard Crauciuc, Fawzy Akad, Diana Popovici, Roxana Gireadă
Introducere. În ultimele decenii, sistemul medical se confruntă tot mai des cu paciente obeze sau supraponderale. Obezitatea este asociată cu un ri...
31 mai 2022
OBSTETRICS | Ediţia 2 28 / 2020
Provocarea trombofiliei: profilul pacientelor cu trombofilii compuse rare
Diana Ioana Voicu, Octavian Munteanu, Luciana Arsene, Florina Păuleț, Oana Bodean, Eugen Radu, Monica Mihaela Cîrstoiu
Trombofilia este o patologie multigenică. Mutaţia factorului V Leiden şi mutaţia genei protrombinei G20210A sunt cele mai frecvente trombofilii ere...
18 mai 2020
OBSTETRICĂ | Ediţia 5 (3) / 2014
Management atipic în sarcina gemelară (FIV-ET) după avortul spontan al primului făt
Andreea Velișcu, Bogdan Marinescu, Bogdan Luchian, Mihai Mitran, Lucia Costoiu
Prezentăm cazul unei paciente în vârstă de 42 de ani cu sarcină gemelară obţinută prin fertilizare in vitro care la 15 săptămâni este internată pen...
15 octombrie 2014
GYNECOLOGY | Ediţia 1 27 / 2020
Ecografia în endometrioza infiltrativă profundă
Anca Daniela Stănescu, Romina-Marina Sima, Denisa-Oana Bălălău, Alina Talpalaru, Liana Pleș
Introducere. Endometrioza cu diferite grade de severitate afectează aproximativ 5% dintre femei. Aceasta poate implica ovarele, peritoneul pelvian,...
13 martie 2020