Introduction. Minimally invasive gynecologic procedures, such as hysteroscopic myomectomy, laparoscopic myomectomy and hysteroscopic uterine septum resection, present numerous advantages, including the preservation of the reproductive potential. Hence, they have been widely used in recent years. However, the number of patients with complications has also increased, including pregnant women with uterine rupture, and associated significant hemorrhage and elevated risk of hemodynamic collapse. Case series. We present four cases of women with pregnancies following minimally invasive gynecologic procedures with uterine rupture and acute surgical abdomen and the management that was applied in the Department of Obstetrics and Gynecology of the Bucharest University Emergency Hospital. Conclusions. Minimally invasive gynecologic procedures do not lack complications, therefore the potential risks in future pregnancies must be explained to patients before surgery. Great care must be taken in choosing patients feasible for this kind of procedures, given the possible complications, in order to reduce maternal and fetal morbidity and mortality.
Complicaţii rare pe termen lung ale intervenţiilor minim invazive în cursul sarcinii
Long-term rare complications of minimally invasive gynecologic procedures during pregnancy
First published: 31 mai 2022
Editorial Group: MEDICHUB MEDIA
DOI: 10.26416/Gine.36.2.2022.6545
Abstract
Rezumat
Introducere. Procedurile ginecologice minim invazive, precum miomectomia histeroscopică sau laparoscopică şi rezecţia histeroscopică a septurilor uterine, prezintă numeroase avantaje, incluzând prezervarea potenţialului reproductiv. Astfel, acestea au fost folosite frecvent în ultimii ani. Totuşi, numărul pacientelor cu complicaţii a crescut de asemenea, incluzând gravide care prezintă ruptură uterină, în asociere cu hemoragie semnificativă şi cu un risc crescut de colaps hemodinamic. Prezentare de cazuri. Prezentăm patru cazuri ale unor paciente cu istoric de proceduri ginecologice minim invazive, cu ruptură uterină şi abdomen acut chirurgical, dar şi managementul acestor cazuri în cadrul Departamentului de obstetrică şi ginecologie al Spitalului Universitar de Urgenţă Bucureşti. Concluzii. Procedurile ginecologice minim invazive nu sunt lipsite de complicaţii, astfel că riscurile potenţiale la sarcinile viitoare trebuie explicate acestor paciente înainte de intervenţie. Având în vedere posibilele complicaţii, pacientele fezabile pentru acest tip de intervenţii trebuie alese cu grijă, cu scopul de a reduce riscurile materne şi fetale de morbiditate şi mortalitate.
Introduction
Minimally invasive gynecologic procedures have been widely used in recent years due to their advantage of preserving the reproductive potential. Although they came along with numerous benefits, these procedures also carry some short- and long-term complications. Hence, these procedures cannot be ignored since they might represent the cause of maternal and fetal morbidity and mortality(1-3).
Hysteroscopy, laparoscopic myomectomy and hysteroscopic uterine septum resection present numerous advantages, such as short hospital stay, faster recovery time and less postoperative pain(4-8). Also, if comparing laparotomy myomectomy with laparoscopic myomectomy, the latter presents lower intraoperative blood loss and less morbidity(9). However, these minimally invasive gynecologic procedures do not lack complications, such as uterine rupture, therefore the potential risks in future pregnancies must be explained to these patients before surgery(2,4,5,10-12).
The rupture of the uterine wall in pregnant women is a rare but severe event which may be the cause of significant hemorrhage, resulting in hemodynamic collapse(4,5,13-15). Uterine rupture may appear on an unscarred uterus, but the risk increases if the patient has a medical history consistent with uterine surgery(4,16). Risk factors for uterine rupture include previous caesarean section, laparotomic or laparoscopic myomectomy, trauma, placenta percreta, choriocarcinoma, uterine abnormalities or uterine overdistension(5,17). In women without surgical history, the incidence is very low, being around 0.012% or 0.03-0.08%, depending on the study, while in women with abdominal myomectomy the incidence is 0-4%, and in women with laparoscopic myomectomy the incidence is 0-1%(18-21).
Wound healing is an essential step in preventing uterine rupture after laparoscopic myomectomy. The risk increases with unsuccessful hemostasis and the persistence of myometrial defects and it is influenced by the methods and tools used during the procedure. Regarding hysteroscopy, the risk depends upon the purpose of the procedure. Hence, the highest risk is associated with myomectomy, while the lower risk is associated with polypectomy and diagnostic hysteroscopy(4). The risk depends on the number and the size of the myomas and if they protrude in the endometrial cavity or not, although there are studies claiming the fact that uterine ruptures appear regardless of myoma characteristics(1,5,18,22).
The exact mechanism of the uterine rupture occurrence is not known, but they might be associated with suboptimal healing or local infection, inadequate tools or methods, induced pneumoperitoneum from laparoscopy, improper suture of the uterine wall, poor hemostasis and hematoma formation, inappropriate use of monopolar of bipolar electrosurgery, with subsequent devascularization and myometrial necrosis in some segments of the uterus, resulting in vicious scars(4,5,10,23). Electrosurgery used for uterine incisions and hemostasis is still a matter of debate, given that there are no conclusive studies yet to describe its impact on uterine rupture formation(10,24). Individual factors on which healing process depends, such as excess collagen deposition, must also be taken into consideration(5,18).
During hysteroscopy, uterine perforation occurs in a percentage of 1.5%. Conservative management is taken into consideration in uterine fundal perforation made with a uterine sound or narrow dilator and in the absence of bleeding. In cases of perforations with sharp instruments or in evident bleeding, laparoscopy or even laparotomy may be indicated. Hence, the associated risk of uterine rupture during pregnancy, depending on the medical history of the patient(25).
Case series
We present four cases and the management that was applied in the Department of Obstetrics and Gynecology of the Bucharest University Emergency Hospital. These cases include women with pregnancies following minimally invasive gynecologic procedures like laparoscopy and hysteroscopy. These minimally invasive procedures were the cause of maternal morbidity, such as illustrated here, as all patients presented with acute surgical abdomen, therefore requiring emergency surgical procedures.
Case 1
A 37-year-old woman (gravida 4, para 2) presented to the Bucharest University Emergency Hospital with amenorrhea lasting for two weeks in association with irregular menstrual cycle in the last four months, despite the treatment she was following with combined oral contraceptive pills in the last eight years. Her medical history consists of two vaginal deliveries and two induced abortions, the latter taking place eight years ago. The patient reported an episode of severe headache, acute postcoital pelvic pain, which was followed by an episode of lipothymia.
Clinically, the patient was alert, awake and afebrile but presented signs of hemodynamic and respiratory instability, in association with diffuse abdominal tenderness, rebound tenderness and guarding. Vaginal examination revealed no genital bleeding. Hence, the suspicion was of ruptured ectopic pregnancy.
Transvaginal ultrasonography showed an ectopic abdominal gestational sac containing a 11-week viable embryo, in association with important intraperitoneal hemorrhage.
The patient’s complete blood count showed a hemoglobin level of 9.4 g/dL and a hematocrit level of 25.5%.
Due to the presence of intraperitoneal bleeding and ectopic abdominal pregnancy, exploratory laparotomy was performed. Approximately 2000 mL of hemorrhagic peritoneal fluid were drained. Laparotomy revealed bilateral fallopian tubes and ovaries of normal aspect, a small uterus, and a gestational sac with a diameter of approximately 7 cm (Figure 1).
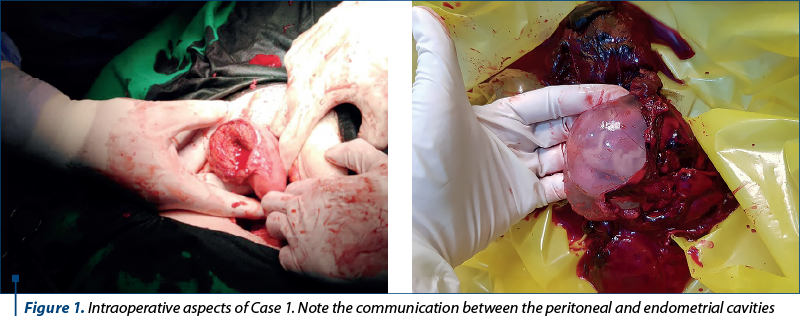
The source of active bleeding turned out to be some anomalous epiploic vessels in association with vessels originating from abnormal tissue covering the uterine fundus, which provided the vascularization of the trophoblast. After removing the trophoblastic tissue from the uterus, a communication between peritoneal and endometrial cavities was observed (Figure 1). This was suggestive for iatrogenic uterine perforation, which was later followed by ectopic implantation of the embryo in this site. Partial omentectomy, curettage of the uterine cavity and hemorrhage control were performed. Intraoperative blood transfusion and one unit of fresh frozen plasma were needed. The patient did not present any postoperative complications and was discharged after four days.
Case 2
A 35-year-old woman (nulligravida, nullipara) was referred to the Bucharest University Emergency Hospital with severe hypochromic microcytic anemia and diffuse abdominal pain during a 20-week pregnancy obtained after embryo transfer. Her medical history consisted of one minimally invasive procedure – a hysteroscopic resection of an endometrial polyp.
Clinically, the patient was conscious, febrile (38.5ºC), presenting skin pallor, hypotension (100/50 mmHg) and tachycardia (95 bpm). On examination, there was distension of the abdomen caused by an irregular pelvic mass whose superior border was located at the level of the umbilicus. During palpation, abdominal pain and slight guarding were present, suggesting discrete peritoneal irritation. On gynecological examination, the cervix had a normal appearance, presenting minimal discharge. During bimanual examination, the uterus was tender to palpation, had a normal size and the limit between it and the pelvic mass described above was present.
Ultrasonographic examination revealed an intraabdominal gestational sac with embryonic demise (20 weeks). The placenta was implanted on the fundus and posterior uterine wall, showing poor vascularization. The complete blood count revealed leukocytosis (30,190/µL) and low hemoglobin (7.1 g/dL) and hematocrit levels (19.3%).
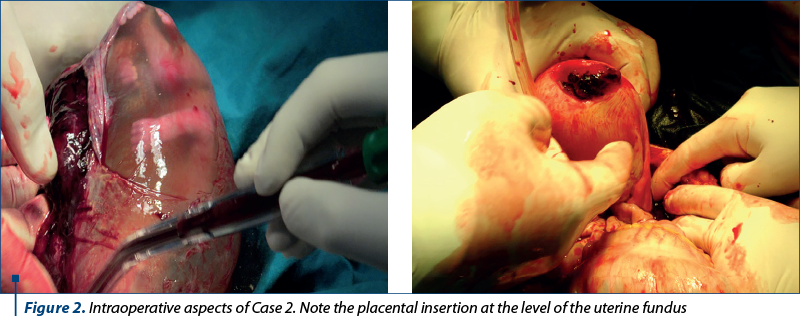
Emergency surgery was performed, revealing an intraperitoneal hemorrhage, which was caused by an ectopic abdominal gestational sac with the placenta invading the uterine wall up to the myometrium (Figure 2). Surgical hemostasis was performed, the ectopic sac was removed, and the uterine wall was sutured. Postoperatively, two red blood cells units and antibiotic prophylaxis were needed. The patient presented favorable postoperative evolution and, thus, she was discharged after seven days.
Case 3
A 29-year-old woman (primigravida, primipara) presented to the Bucharest University Emergency Hospital with abdominal pain and altered consciousness. She was 29-week pregnant and under medical supervision. Her medical history includes hysteroscopic resection of an incomplete uterine septum and hysteroscopic myomectomy.
On clinical examination, the patient presented hemorrhagic shock with intense pallor, was tachycardic with 120 bpm and hypotensive with systolic blood pressure of 60 mmHg and undetectable diastolic blood pressure. Abdominal distension due to pregnancy was visible, with the uterine fundus halfway between the umbilicus and the xiphoid process. The palpation revealed abdominal tenderness and positive Blumberg’s sign, suggesting peritoneal irritation. On obstetric examination, the fetus was in cephalic presentation, but the fetal heartbeats were absent. Ultrasonography confirmed the pregnancy loss (absent fetal heartbeat using Doppler mode) and showed a significant amount of free intraperitoneal fluid, suggesting massive hemoperitoneum.
The patient’s complete blood count illustrated severe posthemorrhagic anemia with hemoglobin levels of 5.1 g/dL and hematocrit levels of 22.3%, in association with leukocytosis (24,140/µL) and thrombocytopenia (107,000/µL).
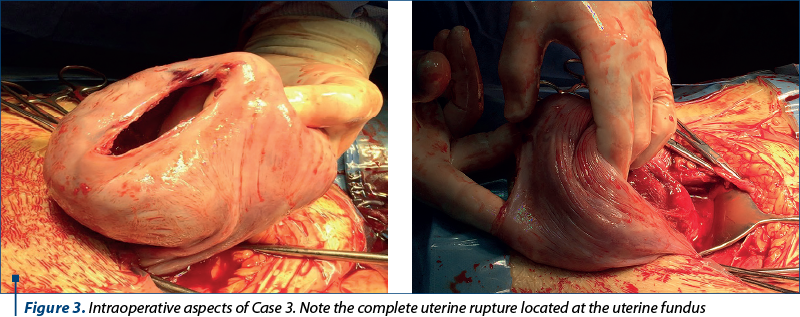
During emergency surgery, approximately 3000 mL of blood and blood clots were drained. Transverse uterine incision was needed for the extraction of a dead female fetus of 1300 g. We detected a stage IV uterine rupture measuring approximately 10 cm involving the uterine fundus (Figure 3). Both the incision and the rupture were sutured. Level 1 infusion was needed to regain hemodynamic stability, along with antibiotics and anti-inflammatory drugs to prevent infection and pain. The postoperative evolution was favorable, and the patient was discharged after eight days.
Case 4
A 35-year-old woman (primigravida, nullipara) presented to the Bucharest University Emergency Hospital with painful uterine contractions. She was in week 27 of pregnancy. The medical history includes a laparoscopic myomectomy and uterine rupture during a 16-week former pregnancy. The histopathological analysis of the product of conception from the former pregnancy revealed extreme prematurity in association with multiple visceral edema and dystrophy.
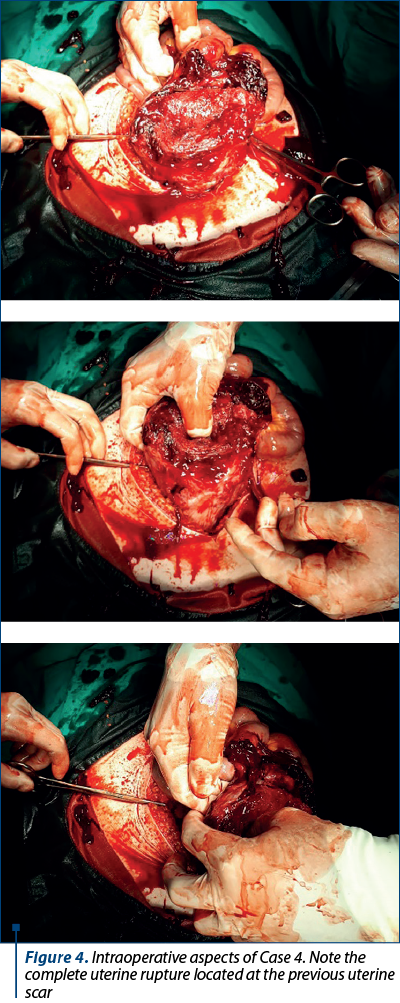
On clinical examination, the patient’s blood pressure was 105/70 mmHg, in association with skin pallor. Inspection revealed abdominal distension due to pregnancy, while palpation showed diffuse pain and the uterine fundus being located halfway between the umbilicus and the xiphoid process. On pelvic examination, it was observed a tumoral mass arising from the external cervical ostium, without any blood or amniotic fluid loss. Ultrasonography revealed the myometrium with an area of extreme thinness (approximately 2 mm) on the anterior uterine wall, near the placental insertion. Fluid was present in pouch of Douglas. Although the initial clinical examination in association with an ultrasound did not suggest signs of fetal distress, six days later the patient became anxious, reported painful uterine contractions and fetal cardiac rate dropped below 80 bpm. Emergency caesarean section was performed due to fetal distress and the suspicion of uterine rupture with hemoperitoneum. A moderate amount of blood was drained from the peritoneal cavity and a breach in the uterine wall was observed at the level of the uterine scar (Figure 4). The fetus was extracted through the solution of continuity. Adhesiolysis and enterorrhaphy were performed. The postoperative outcome was favorable.
Discussion
Ultrasonography is one of the most important diagnostic tools in pregnancies associated with uterine rupture(26). Although it is the elected imaging technique, ultrasonography’s results might be affected by intestinal gas and low resolution. Computed tomography (CT) is not indicated in pregnant women due to its radiation risks to the fetus(4). Magnetic resonance imaging (MRI) is a useful technique, but it is not of first choice. However, both CT and MRI are useful, depending on the context(4,27). After the clinical diagnosis of hemoperitoneum is given, laparotomy represents the surgical procedure of choice(26).
Ndwambi et al. describe a case of a 9-week abdominal ectopic pregnancy following uterine perforation which occurred after the voluntary interruption of pregnancy. The patient presented abdominal pain and reduced vaginal bleeding. Ultrasonography was used for establishing the correct diagnosis. Exploratory laparotomy was needed for the removal of the fetus and the placenta(26). In our first case, the patient had a history of two induced abortions. Because of the presence of the ectopic sac and the trophoblastic tissue in the abdominal cavity, attached to the exterior portion of the uterine breach, we cannot exclude the possibility of a persistent uterine wall defect after the last voluntary interruption of pregnancy. Hence, all women, especially those who underwent this kind of procedure, should present for a gynecologic exam before conception.
Zhao et al. present a case series of uterine rupture during pregnancy after hysteroscopic and laparoscopic procedures. One patient previously needed laparoscopy due to an isthmic pregnancy requiring salpingectomy, while the other patient needed hysteroscopy to remove the endometrial polyps. In all cases, laparotomy was performed and confirmed the presence of intraperitoneal hemorrhagic fluid along with uterine ruptures, the widest from these cases measuring 10 cm(4). In our second case, the patient had a medical history of hysteroscopic resection of an endometrial polyp. As in the cases cited in the literature, she also needed laparotomy due to hemoperitoneum. Although the uterine rupture was not that large as those presented by Zhao et al., the uterine bleeding was significant in our case because of the trophoblastic invasion of the myometrium, the most vascularized uterine wall layer.
Tomczyk et al. present a case of a 6-cm uterine rupture in a 28-week pregnant woman, after a subserosal myoma removal using laparoscopic myomectomy(18). During the study of 768 patients with laparoscopic myomectomy, Landi et al. reported intraoperative complications in 12 patients, meaning 3.3%(10). Uterine perforation with a manipulator was described, afterwards the uterine wall being repaired with a single suture. Myometrial perforation with a uterine sound was also described(10). Hence, the possibility of persistent uterine wall rupture in women who become pregnant. In our third case, the patient had a history of both hysteroscopic myomectomy and hysteroscopic resection of an incomplete uterine septum. She presented with hemorrhagic shock caused by the presence of an approximately 10-cm uterine rupture. Although we do not know which of the procedure caused the uterine breach, the medical history of two minimally invasive gynecologic procedures probably increased the risk of uterine wall weakening and rupture during pregnancy.
Vimercati et al. describe two cases of uterine ruptures during pregnancy following laparoscopic myomectomy, the first case being at 34 weeks of gestation, while the second being at 18 weeks of gestation. Ultrasonography, exploratory laparotomy and hemoperitoneum drainage were performed in both cases. In the first case, the baby was delivered alive along with the placenta, but in the second case, abortion was needed(5). In our fourth case, the patient had a history of laparoscopic myomectomy but also a history of uterine rupture during a former pregnancy. Intraoperatively, we concluded that the source of bleeding was the preexisting uterine scar which presented a rupture. Thus, uterine scars represent a low resistance area and might be the place of uterine rupture, especially in this case, as this was the second time the patient presented with a uterine breach during pregnancy.
Hence, it can be noted that ultrasonography was the main imaging technique used for patients’ examination, and exploratory laparotomy was the surgical modality of choice, given the presence of increased maternal and fetal morbidity and mortality. Gynecologists must be very careful about the patient’s medical history, including minimally invasive gynecologic procedures, and identify women with high risk during pregnancy, such as patients with known uterine scars or uterine rupture during former pregnancies, as we presented above.
Conclusions
Minimally invasive gynecologic procedures, such as hysteroscopy and laparoscopy, represent an important risk factor for obstetrical complications. Given the possible complications, great care must be taken in choosing patients feasible for this kind of procedures.
The uterine scar resulting from minimally invasive gynecologic procedures is a potential place for uterine perforation or ectopic pregnancy implantation. Hence, it is shown the importance of an interdisciplinary team and its role to reduce maternal and fetal morbidity and mortality.
Conflict of interests: The authors declare no conflict of interests.
Bibliografie
-
Koo YJ, Lee JK, Lee YK, Kwak DW, Lee IH, Lim KT, et al. Pregnancy outcomes and risk factors for uterine rupture after laparoscopic myomectomy: a single-center experience and literature review. J Minim Invasive Gynecol. 2015;22(6):1022-8.
-
Kim HS, Oh SY, Choi SJ, Park HS, Cho GJ, Chung JH, et al. Uterine rupture in pregnancies following myomectomy: A multicenter case series. Obstet Gynecol Sci.2016;59(6):454-62.
-
Turner MJ. Uterine rupture. Best Practic Res Clin Obstet Gynaecol. 2002;16(1):69-79.
-
Zhao B, Wang Y, Zhang Y. Uterine rupture in patients with a history of laparoscopy or hysteroscopy procedures: Three case reports. Medicine (Baltimore). 2019;98(20):e15491.
-
Vimercati A, Del Vecchio V, Chincoli A, Malvasi A, Cicinelli E. Uterine rupture after laparoscopic myomectomy in two cases: real complication or malpractice? Case Rep Obstet Gynecol. 2017;2017:1404815.
-
Kasapoglu T, Kasapoglu D, Deren O. Successful management of the recurrent uterine rupture after the uterine septum resection. Case Rep Womens Health. 2015;8:13-6.
-
Flyckt RL, Falcone T. Uterine rupture after laparoscopic myomectomy. J Minim Invasive Gynecol. 2015;22(6):921-2.
-
Zeteroğlu Ş, Aslan M, Akar B, Bender RA, Başbuğ A, Çalışkan E. Uterine rupture in pregnancy subsequent to hysteroscopic surgery: A case series. Turkish J Obstet Gynecol. 2017;14(4): 252-5.
-
Paul GP, Naik SA, Madhu KN, Thomas T. Complications of laparoscopic myomectomy: a single surgeon’s series of 1001 cases. Aust N Z J Obstet Gynaecol. 2010;50(4):385-90.
-
Landi S, Zaccoletti R, Ferrari L, Minelli L. Laparoscopic myomectomy: technique, complications, and ultrasound scan evaluations. J Am Assoc Gynecol Laparosc. 2001;8(2):231-40.
-
Dubuisson JB, Chapron C, Levy L. Difficulties and complications of laparoscopic myomectomy. J Gynecol Surg. 1996;12(3):159-65.
-
Bean EMR, Cutner A, Holland T, Vashisht A, Jurkovic D, Saridogan E. Laparoscopic myomectomy: a single-center retrospective review of 514 patients. J Minim Invasive Gynecol. 2017;24(3):485-93.
-
Cîrstoiu MM, Secară DC, Secară ID, Tufan CF, Bohîlţea RE, Munteanu O. The relation between uterine scar determined by hysteroscopic procedures and acute abdomen during pregnancy. Case series. Ginecologia. ro. 2015;3(8):6-11.
-
Khallouk Z, Bouhache S, Moussaoui KEL, Louzali FZ, Badsi S, Zeraidi N, Baidada A. Factors predictive of uterine rupture after operative hysteroscopy. J Gynecol Obstet Biol Reprod (Paris). 2004;33(1 Pt 1):51-5.
-
Altgassen C, Kuss S, Berger U, Löning M, Diedrich K, Schneider A. Complications in laparoscopic myomectomy. Surgi Endosc. 2006;20(4):614-8.
-
Teodor OM, Munteanu O, Cîrstoiu MM. A rare case of secondary abdominal pregnancy – case report and literature review. Ginecologia.ro. 2022;35:12-5.
-
Ogbole GI, Ogunseyinde OA, Akinwuntan AL. Intrapartum rupture of the uterus diagnosed by ultrasound. Afr Health Sci. 2008;8(1):57-9.
-
Tomczyk KM, Wilczak M, Rzymski P. Uterine rupture at 28 weeks of gestation after laparoscopic myomectomy – a case report. Menopause Rev. 2018;17(2):101-4.
-
Abbas AM, Abdallah M, Michael A. Recurrent rupture uterus after hysteroscopic resection of uterine septum: A case report. Middle East Fertil Soc J. 2017;22(4):340-2.
-
Pakniat H, Soofizadeh N, Khezri MB. Spontaneous uterine rupture after abdominal myomectomy at the gestational age of 20 weeks in pregnancy: A case report. Int J Reprod Biomed. 2016;14(7):483.
-
Garnet JD. Uterine rupture during pregnancy: an analysis of 133 patients. Obstet Gynecol. 1964;23(6):898-905.
-
Buckley VA, Nesbitt-Hawes EM, Atkinson P, Won HR, Deans R, Burton A, et al. Laparoscopic myomectomy: clinical outcomes and comparative evidence. J Minim Invasive Gynecol. 2015;22(1):11-25.
-
Nkemayim DC, Hammadeh ME, Hippach M, Mink D, et al. Uterine rupture in pregnancy subsequent to previous laparoscopic electromyolysis. Arch Gynecol Obstet. 2000;264(3):154-6.
-
Sentilhes L, Sergent F, Berthier A, Catala L, Descamps P, et al. Uterine rupture following operative hysteroscopy. Gynecol Obstet Fertil. 2006;34(11):1064-70.
-
Stany MP, Farley JH. Complications of gynecologic surgery. Surg Clin North Am. 2008;88(2):343-59.
-
Ndwambi M, Martínez FL. Ectopic abdominal pregnancy due to uterine perforation after an attempt to terminate pregnancy: a case presentation. Medwave. 2017;17(6):e7000.
-
Wye D, Magotti R, Al-Mashat D, Benzie R, Condous G. Sonographic diagnosis of spontaneous uterine rupture at the site of cornual wedge resection scar – a case report. Australas J Ultrasound Med. 2014;17(1):45-8.
Articole din ediţiile anterioare
Indicaţiile şi contraindicaţiile naşterii vaginale după operaţie cezariană
În ultimii ani, modalitatea de naștere este reprezentată de operația cezariană într-un procent foarte ridicat. Operația cezariană reprezintă aproap...
Relaţia dintre cicatricea uterină determinată de intervenţii histeroscopice şi abdomenul acut chirurgical în sarcină - prezentare de cazuri -
Abdomenul acut chirurgical în cursul sarcinii reprezintă o entitate patologică, plurietiologică, cu evoluţie rapidă şi risc vital atât pentru partu...