Introduction. Although there has been made great progress in understanding the epidemiology of high-grade cervical intraepithelial lesions (CIN 2/3), the cofactors involved in the dynamics of cervical HPV infection are still a subject of debate. The purpose of this paper was to assess the patients’ demographic characteristics correlated with the risk of lesions’ persistence/recurrence post-cervical excisional therapy for CIN 2/3.
Materials and method. We conducted an analytical, observational, prospective cohort study carried out in the “Prof. Dr. Panait Sîrbu” Clinical Hospital of Obstetrics and Gynecology over a 3-year period. We included 290 patients diagnosed with high-grade cervical dysplasia who benefited from conization in our clinic. The demographic variables obtained from the anamnesis were statistically correlated with the rate of persistent/recurrent cervical lesions post-therapy.
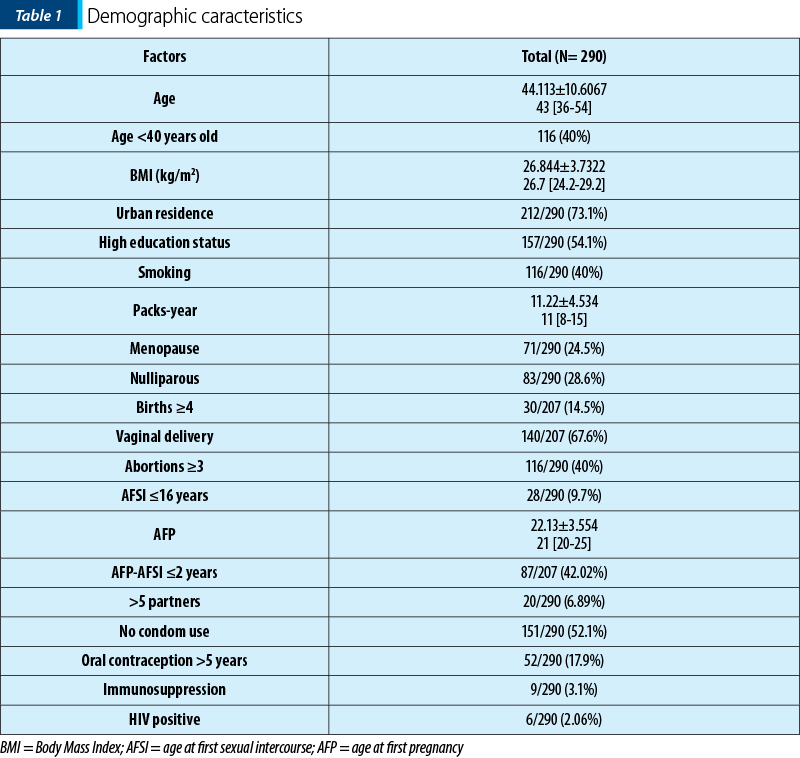
Results. The mean age for our study group was 44.1 years old; more than half of the patients (73.1%) came from urban environments and were highly educated (54.1%). Regarding personal obstetrical history, most of the patients were multiparous (71.3%), with 14.5% having more than four births and 67.6% having delivered vaginally. The mean age at the first sexual intercourse was 22.13 years old, and more than half of the patients claimed never having used the condom. Nine patients (3.1%) had been diagnosed with immunodeficiency syndromes, out of which six patients were HIV-positive. The multivariate logistic regression analysis showed that age (OR=1.08; p<0.01), smoking status (OR=3.96; p<0.01) and age at first pregnancy (OR=0.87; p<0.01) were independent predictive factors for the risk of persistence/recurrence of CIN lesions.
Conclusions. The three factors that were statistically correlated with persistent/recurrent CIN after therapy can be used as a predictive model for clinicians struggling to prevent cervical neoplastic invasive lesions.
Corelaţia dintre factorii demografici şi rata de persistenţă/recurenţă a leziunilor CIN după conizaţie
The correlation between patients demographic characteristics and the rate of persistent/recurrent high-grade CIN after conization
First published: 27 decembrie 2018
Editorial Group: MEDICHUB MEDIA
DOI: 10.26416/Gine.22.4.2018.2141
Abstract
Rezumat
Introducere. Cu toate că înţelegerea epidemiologiei leziunilor cervicale intraepiteliale de grad înalt (CIN 2/3) s-a îmbunătăţit semnificativ, cofactorii implicaţi în istoria naturală a infecţiei cervicale cu HPV rămân un subiect deschis în literatură. Scopul acestei lucrări este de a identifica factorii demografici corelaţi cu riscul de persistenţă/recurenţă lezională post-terapie conservatoare pentru CIN 2/3.
Materiale şi metodă. Am efectuat un studiu analitic, observaţional, prospectiv, în cadrul Spitalului Clinic de Obstetrică-Ginecologie „Prof. Dr. Panait Sîrbu”, pe o perioadă de trei ani, care a inclus 290 de paciente diagnosticate histologic cu CIN 2/3, la care s-a practicat terapie excizională cervicală conservatoare (conizaţie). Parametrii demografici obţinuţi din datele anamnestice au fost corelaţi statistic cu rata de persistenţă/recurenţă a leziunilor cervicale după terapie.
Rezultate. Vârsta medie a pacientelor din lot a fost de 44,11 ani, peste jumătate dintre paciente (73,1%) provenind din mediul urban şi având studii superioare (54,1%). În ceea ce priveşte istoricul obstetrical, majoritatea pacientelor au fost multipare (71,3%), iar dintre acestea, 14,5% au prezentat peste patru naşteri şi 67,6% au născut pe cale vaginală. Vârsta medie de debut a vieţii sexuale pentru lotul de studiu a fost de 22,13 ani şi peste jumătate dintre paciente au afirmat neutilizarea contracepţiei de barieră. Nouă paciente (3,1%) au fost diagnosticate cu sindroame de imunosupresie, şase dintre acestea fiind pozitive pentru HIV. Dintre variabilele pentru care am identificat asociere statistică cu riscul de persistenţă/recurenţă lezională, cele care au fost independent predictive (conform analizei de regresie logistică multivariată) sunt: vârsta (OR=1,08; p<0,01), statusul de fumătoare (OR=3,96; p<0,01) şi vârsta la momentul primei naşteri (OR=0,87; p<0,01).
Concluzii. Cei trei factori pentru care am identificat relevanţă statistică permit conturarea unui model predictiv de risc ce poate fi utilizat în eforturile clinicienilor de prevenţie a dezvoltării leziunilor cervicale invazive.
Introduction
Over the last three decades, the level of knowledge and understanding regarding the epidemiology and pathogenic dynamics of cervical neoplasia has increased significantly(1). Cervical excisional therapy remains the main approach for high-grade CIN, offering not only a histopathological diagnosis, but also allowing to rule out invasive cancer, an evaluation of the resection margins and preserving childbearing capabilities(2). Nonetheless, clinical studies have shown that patients who benefit from such a therapeutic solution for CIN2/3 lesions still pose a higher risk of being diagnosed with cervical cancer in comparison to healthy women. A meta-analysis review proved that the incidence of invasive cervical neoplasia is 56/100,000 for at least 20 years post-therapy, this rate being 10 times higher as opposed to the one seen in the general population(3); in addition, another study reported cumulative rates of CIN2/3 detection at six years after treatment of 14%(4).
The rate of persistent/recurrent CIN after treatment varies in literature studies from 1% to 21%(5), the most important mechanisms explaining this phenomenon being: incomplete excision of the lesion, persistent high-risk HPV infection, reinfection with a different HPV strain(6). Still, the risk factors involved in the development of persistent/recurrent disease are controversial and remain a matter of debate.
Objectives
In the present study we sought to evaluate the demographic characteristics which could potentially be linked to the rate of CIN persistence/recurrence after primary conization. The identification of such factors could be valuable in optimizing the follow-up protocol by creating a risk assessment model and also avoiding overtreatment.
Matherials and method
We performed an analytical, observational, longitudinal, prospective cohort study in the “Prof. Dr. Panait Sîrbu” Clinical Hospital of Obstetrics and Gynecology, involving 290 patients diagnosed with high-grade cervical dysplasia who benefited from conservative excisional therapy (conization) in our clinic. The inclusion criteria used were: initial diagnosis (either cytological or histological) of high-grade squamous lesion, conization performed in our hospital setting, histopathological examination and colposcopic examination performed in our hospital, known HPV status before surgery and at least one follow-up visit, a minimum of two follow-up visits (at 12 and 24 months after therapy), informed consents for colposcopy, anesthesia and surgical procedures (cervical biopsy, endocervical sampling, cervical excision, hysterectomy).
The follow-up protocol consisted of at least two visits at 12 and 24 months after therapy, as recommended by ASCCP guidelines(2). We performed for each visit: clinical examination, liquid based cervical cytology and HPV testing (co-testing). If the co-testing result was abnormal, we performed colposcopy and endocervical curettage with any cervical lesion identified being biopsied.
If both co-testing results were normal, we performed retesting at three years and for these patients the persistent/recurrent disease was considered absent.
The criterion used for defining persistent/recurrent lesions was identifying histological CIN on cervical specimens obtained from biopsies, endocervical curettage, reexcision and total hysterectomy performed during the follow-up program. When documented, the therapeutic approach for persistent/recurrent disease was chosen taking into consideration the grade of dysplasia, age and the patient’s desire for fertility sparing.
After performing the patients anamnesis, we collected and analyzed the following parameters: age (years), Body Mass Index, residence (urban/rural setting), education status, smoking status, menopause status, parity, mode of delivery (vaginal/caesarean section), age at first pregnancy (AFP), abortion rate, age at first sexual intercourse (AFSI), short period between AFSI-AFP≤2 years, having more than five partners, unprotected sexual intercourse, use of combined contraceptive pills for a period longer than five years, previously diagnosed immunodeficiency syndromes (including HIV status).
The data obtained were statistically analyzed using standard methods of descriptive statistics (means, median, SD). The characteristics of the patients were compared between the study group in which persistent/recurrent lesions were identified and the group without these lesions using Fischer exact, Mann-Whitney and Student t tests. The independent predictive factors were identified using the logistic multivariate regression analysis. The level of statistical significance was set at p<0.05.
Results
The mean age for our study group was 44.11 years old, with a median value of 43 years old, the age group being 28-71 years old. More than half of the patients (60%) were over 40 years old. The level of education analysis showed that 54.1% of the patients were highly educated.
Regarding the residence status, most of the patients lived in an urban setting (212 patients; 73.1%).
For each patient we calculated the Body Mass Index (BMI); the mean value was 26.84±3.73 kg/m2 and the median value was 26.7 kg/m2.
The percentage of smokers in our study group was 40% (116/290) and the pack-year mean value was 11.22, with a median value of 11.
Regarding the personal birth history, 83/290 patients (28.6%) were nulliparous, and of the total of 207 parous women, 30 patients (14.5%) had over four births and 140 patients (67.6%) delivered vaginally. Furthermore, 116 patients (40%) had affirmatively more than three elective abortions.
Regarding the sexual behaviour, 28 patients (9.7%) declared a less than 16 years old age at the first sexual intercourse and 20 patients (6.9%) declared having more than five sexual partners. Also, the latency between the age at first pregnancy and the age at first sexual intercourse less than two years was declared by 87 patients. The mean age at first pregnancy was 22.13 years old, with a median value of 21 years old.
As for contraception, a quarter of the patients (74/290; 25.51%) declared never having used any methods, 139/290 (47.93%) declared using male condom, 62/290 (21.37%) used oral contraceptives and 15/290 (5.17%) declared using IUD.
Nine patients (3.1%) had been previously diagnosed with immunodeficiency syndromes: six patients were HIV-positive, one patient had a history of Hodgkin IIA lymphoma (in remission during our study period), one patient who had undergone mastectomy for breast cancer with adjuvant chemotherapy and radiation therapy, and one patient with psoriasis who was on biological therapy (with human recombinant monoclonal antibodies).
All demographic characteristics of our study group are presented in Table 1.
After a mean follow-up period of 24.97±1.11 months, the rate of persistent/recurrent lesions in the study group was 30.68% (89/290 patients). Using Mann-Whitney and Fischer exact test, we compared the group with persistent/recurrent CIN with the one in which these lesions were absent and obtained statistical significance for: the mean age, BMI, urban residence, high education status, smoking, menopause, nulliparous state, more than four births and vaginal delivery, more than three abortions, AFSI≤16 years, the mean age at first pregnancy, AFP-AFSI≤2 years latency, absence of condom use and HIV-positive status. No difference was observed for the use of contraceptive pills for a period longer than two years and for having more than five sexual partners. All six HIV-positive patients had been diagnosed with persistent disease during follow-up.
These correlations can be seen in Table 2.
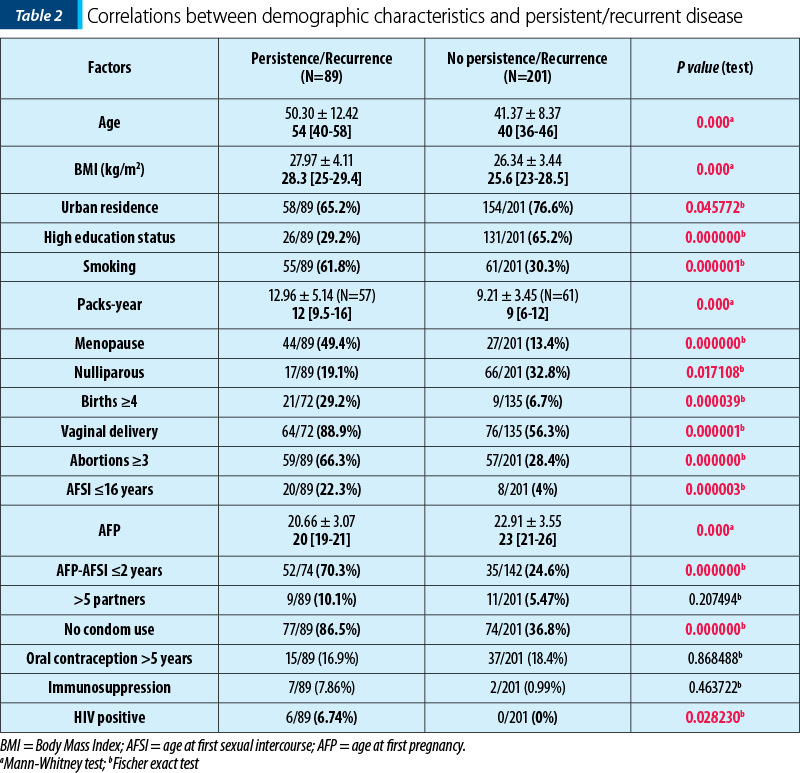
Using the multivariate logistic regression analysis, we found out that age and smoking status were independent predictive factors for residual/recurrent cervical dysplasia (OR=1.08; OR=3.96; p<0.01). The age at first pregnancy was a protective factor, meaning that the higher its value, the lower the risk of persistent/recurrent CIN (OR=0.87; p<0.01).
Discussion
We observed that the mean age of the patients diagnosed with residual/recurrent CIN was significantly higher, and similar results were seen in another case-control study(7). The impact of age on the development of these lesions can be explained by: modulation of the immune system(8), positive selection of persistent HPV oncogenic strains(9) or the higher position of the squamocolumnar junction in menopause patients which limits complete excision of CIN 2/3 lesions.
Living in an urban environment and high education status proved to be associated with a lower risk of developing recurrent/persistent lesions. The lack of medical information that patients tend to have in our country (especially in rural areas), which correlates with cervical cancer screening deficiency, explains the still alarming high rates of invasive cervical cancer(10).
In the present study, smoking increased the odds of having a persistent/recurrent lesion by 3.71; this result is conflicting taking into account that numerous epidemiological studies showed that smoking was a risk factor for CIN 3 and cervical cancer(11). High levels of smoking metabolites such as nicotine, phenols and other hydrocarbons were identified in the cervical mucus of smoking women(11). The mechanisms involved include the direct carcinogenic effect on the cervical epithelial cells(12), but also on Langerhans cells which might contribute to persistence of HPV infection(13).
Having used contraceptive pills for more than 5 years was not found to be a risk factor in our study (OR=0.89; p=0.75), as opposed to not having used barrier contraception (OR=11.01; p<0.01). A possible explanation for this result is that the relationship between oral contraceptive use and the risk for cervical neoplasia is linear, dose-dependent and reversible at 5-10 years after being stopped, and we did not assess in our study the exact time which elapsed from their first usage.
We observed that all six HIV-positive patients had persistent lesions after primary therapy, in accordance with a study which showed that the residual rate for CIN2/3 was 63.6% compared to 31.8% in HIV-negative patients (OR=4.7; CI=1.9-11.5; p<0.001)(14). We did not analyze in this study the influence of the CD4 status, viral load or antiviral therapy. Specifically, the patient with Hodgkin lymphoma underwent two cervical excision procedures and then abdominal total hysterectomy with further negative vaginal cytology reports. At present time, she is still in remission and continues the follow-up protocol in our clinic(15).
Conclusions
To conclude, the most important demographic characteristics correlated in our study with the risk of persistent/recurrent disease after cervical excision are: advanced age, smoking status and age at first pregnancy. Furthermore, immunosuppressed patients (especially HIV-positive patients) are a special category which warrants attention.
Conflict of interests: The authors declare no conflict of interests.
Bibliografie
- Wright TC, Cox TJ. Chapter 4: Cervical Cancer: Epidemiology and Etiology. In: Mayeaux EJ Jr, Cox TJ, ed. Modern Colposcopy: Textbook&Atlas. Lippincott Williams&Wilkins, 2012; 59-71.
- Massad LS, Einstein MH, Huh WK, et al. 2012 updated consensus guidelines for the management of abnormal cervical cancer screening tests and cancer precursors. J Low Genit Tract Dis. 2013; 17(5):S1-S27.
- Soutter WP, Sasieni P, Panoskaltsis T. Long-term risk of invasive cervical cancer after treatment of squamous cervical intraepithelial neoplasia. Int J Cancer. 2006; 118:2048-55.
- Melnikow J, McGahan C, Sawaya GF, Ehlen T, Coldman A. Cervical intraepithelial neoplasia outcomes after treatment: long-term follow-up from the British Columbia Cohort Study. J Natl Cancer Inst. 2009; 101(10):721-8.
- Cox TJ. Chapter 20: Management of lower genital tract neoplasia. In: Mayeaux EJ Jr, Cox TJ, ed. Modern Colposcopy: Textbook&Atlas. Lippincott Williams&Wilkins, 2012; p. 605-55.
- Ryu A, Nam K, Kwak J, Kim J, Jeon S. Early human papillomavirus testing predicts residual/recurrent disease after LEPP. J Gynecol Oncol. 2012; 23:217-25.
- de Mello Silva MV, Coutinho IC, de Andrade Heráclio S, Fittipaldi HM Jr, Katz L. Factors associated with the persistence/ recurrence of CIN2/3 in women submitted to loop electrosurgical excision procedure in a teaching hospital in northeastern Brazil: a case-control study. J Low Genit Tract Dis. 2014; 18(4):286-90.
- Vintermyr OK, Iversen O, Thoresen S, et al. Recurrent high-grade cervical lesion after primary conization is associated with persistent human papillomavirus infection in Norway. Gynecol Oncol. 2014; 133:159-66.
- Verguts J, Bronselaer B, Donders G, et al. High-risk HPV presence in cervical specimens after a large loop excision of the cervical transformation zone: significance of newly detected hr-HPV genotypes. J Med Virol. 2007; 79:314-9.
- http://www.hpvcentre.net/statistics/reports/ROU.pdf.
- Wright TC, Cox TJ. Chapter 4: Cervical Cancer: Epidemiology and Etiology. In: Mayeaux EJ Jr, Cox TJ, ed. Modern Colposcopy: Textbook&Atlas. Lippincott Williams&Wilkins, 2012; p. 65-71.
- Smith JS, Green J, Berrington de Gonzalez, et al. Cervical cancer and use of hormonal contraceptives: a systematic review. Lancet. 2003; 361:1159-67.
- Moody CA, Laimins LA. Human papillomavirus oncoproteins: pathways to transformation. Nat Rev Cancer. 2010; 10:550-60.
- Babkina N, Heller DS, Goldsmith LT, Houck KL. Cervical conization for cervical intraepithelial neoplasia (CIN) 2 and 3 in HIV- positive women: a case-control study. J Low Genit Tract Dis. 2015; 19(2):110-4.
- Maier C, Puia S, Moisa M, Mitran M, Potecă A, Comănescu M, Neagu C, Vlădăreanu C. Rapidly progressive high-grade cervical intraepithelial neoplasia in a Hodgkin lymphoma patient. A case report. Gineco.eu. 2015; 11:111-3.
Articole din ediţiile anterioare
Leziunile CIN de grad înalt în sarcină şi post-partum: o asociere rară. Noutăţi în abordare
Scopul acestei lucrări este de a reevalua oportunitatea terapiei leziunilor CIN 2/3 diagnosticate în cursul sarcinii, pentru a evita progresia a...
Factori predictivi ai bolii reziduale la pacientele cu conizaţie pentru adenocarcinom cervical in situ
Obiective. Scopul lucrării este de a realiza o imagine integrată privind datele recente din literatura de specialitate asupra factorilor de predicţ...