Digestive cancer during pregnancy is a rare condition, but it has a poor prognosis for the mother. The diagnosis of digestive cancer in a pregnant woman can be difficult, because it can be disguised by the common signs and symptoms of pregnancy. Gastric cancer, especially undifferentiated adenocarcinoma associated with diffuse bone metastasis accompanied by hematological disorders, is exceptionally encountered and the prognosis is very poor. A mean survival period of 4-5 months was attributed to gastric cancer with bone metastasis. The management of pregnancy-associated digestive cancer represents a challenge for clinicians, requiring a multidisciplinary approach.
OBSTETRICS
Neoplaziile tractului digestiv în timpul sarcinii – diagnostic şi management
Pregnancy-associated digestive cancer – diagnosis and management
Ana Veronica Uzunov,
Diana Ioana Voicu,
Diana Cristina Secară,
Octavian Munteanu,
Natalia Ţurcan,
Oana Bodean,
Adrian Dumitru,
Maria Sajin,
Polixenia Georgeta Iorga,
Corina Silvia Pop,
Monica Mihaela Cîrstoiu
First published: 04 decembrie 2020
Editorial Group: MEDICHUB MEDIA
DOI: 10.26416/Gine.30.4.2020.3940
Abstract
Rezumat
Cancerele cu punct de plecare în viscerele tractului digestiv în timpul sarcinii reprezintă patologii rar întâlnite, dar care au un prognostic rezervat pentru gravidă. Diagnosticul poate fi dificil, deoarece poate fi mascat de semnele şi simptomele specifice sarcinii. Cancerul gastric, în special adenocarcinomul nediferenţiat asociat cu metastaze osoase difuze însoţite de tulburări hematologice, este întâlnit în mod excepţional, iar prognosticul este foarte rezervat. Un timp mediu de supravieţuire de 4-5 luni a fost atribuit acestui stadiu. Managementul cancerului digestiv întâlnit în sarcină reprezintă o provocare pentru obstetrician şi necesită o abordare multidisciplinară.
Introduction
Cancer during pregnancy is very rare, occurring approximately in 1 per 1,000 pregnancies annually, corresponding to 0.07% to 0.1% of all malignant tumors(1).
The physiological changes occur in pregnancy during the fetal development and have the role to prepare the mother for labor and delivery(1). It is important to differentiate between normal and pathological changes, because some physiologic changes mimic the symptoms of a variety of conditions, and vice versa(1).
Pregnancy involves changes in maternal physiology, including alterations in hematologic parameters like expansion in maternal blood and plasma volume(1,2). Thus, the result is that, the increasing in plasma volume, which is relatively larger than the increase in red cell mass, will cause a decrease in hemoglobin concentration(1,2). Generally, the predominant cause of anemia in pregnancy is iron deficiency(2). During pregnancy, anemia is defined as hemoglobin (Hb) <10 g/dL and hematocrit (Hct) <30%(1,2).
If Hb is <11.5 g/dL at the onset of pregnancy, the women can be treated prophylactically because subsequent hemodilution usually reduces Hb to <10 g/dL(1-3). However, oxygen-carrying capacity remains normal during pregnancy(3). Hematocrit normally increases immediately after birth(3).
Several types of anemia can develop during pregnancy. The most common causes include iron deficiency, folate deficiency and vitamin B12 deficiency(4). Anemia is a condition in which the patient has a lack of enough healthy red blood cells to carry adequate oxygen to the body’s tissues(4,5). The early symptoms of anemia are usually non-specific(5). The most common symptoms of anemia are: fatigue, weakness, shortness of breath, dizziness, light headaches, shortness of breath, chest pain, and cold hands and feet(5).
Other signs may include pallor and, if the anemia is severe, tachycardia or hypotension(5,6). There are many forms of anemia, each with its own cause. Anemia can be temporary or long term, and it can range from mild to severe(6).
Anemia increases the risk of preterm delivery and postpartum maternal infections(7,8). Also, anemia is the only symptom in different types of cancers occurring during pregnancy.
Materials and method
We performed an observational retrospective analysis of all women diagnosed with digestive cancer during pregnancy admitted in the Department of Obstetrics and Gynecology of the Bucharest University Emergency Hospital, a tertiary center in Romania, between the 1st of January 2018 and the 31st of October 2020. The information regarding pregnancy, delivery outcomes and neonatal data was retrieved from the hospitalization sheets and the data base system of the Bucharest University Emergency Hospital.
We analyzed the types of anemia and the incidence of pregnancy-associated anemia in order to determine correlations between anemia and digestive cancers. The most frequent pathologies associated with anemia in pregnancy were also studied.
Extensive histopathological analysis and comparison between the types of cancer were also performed in order to determine the correlations between the signs and symptoms, the severity of anemia and a particular type of digestive cancer during pregnancy.
The study was approved by the Ethics Committee of the Bucharest University Emergency Hospital. The statistical analysis was performed using Microsoft Excel and SPSS 9.5 softwares.
Results
A total of 7,858 pregnant patients, with a gestational age over 20 weeks of amenorrhea, were admitted in the Department of Obstetrics and Gynecology of the Bucharest University Emergency Hospital between the 1st of January 2018 and the 31st of October 2020. The incidence of pregnancy-associated anemia was 15.1%. This percentage corresponds to the analysis of 563 cases of pregnancy-associated anemia admitted in our unit during those three years.
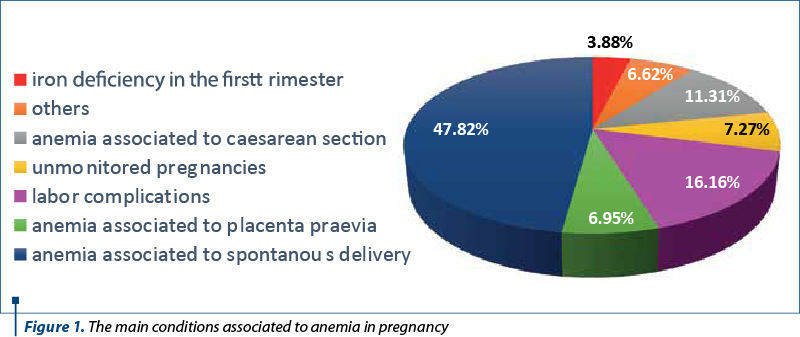
As shown in Figure 1, the predominant conditions that lead to pregnancy-related anemia are spontaneous (45.61%) and caesarean birth (15.41%), labor complications (15%), followed by conditions such as placenta praevia (7%) and other causes of antenatal metrorrhagia in pregnancy (10.79%). Also, a significant percentage corresponds to unmonitored pregnancies (7%). Many other pathologies related to anemia in pregnancy appeared with a lower incidence. Digestive disorders combined with pregnancy and anemia had an incidence of approximately 1% (Figure 1).
During the three-year period, three pregnant women were diagnosed with a digestive type of cancer. Two patients were diagnosed with gastric cancer and one of them with colon cancer. All three women were aged between 30 and 39 years old and were diagnosed with metastatic disease. Regarding the parity, the patients were primiparous or secundiparous. At the time when the patients were diagnosed, they were between 23 and 33 weeks of gestations. The two patients with gastric cancer were diagnosed early, at 23 weeks and 24 weeks of pregnancy, while the patient with colon cancer was diagnosed at 33 weeks of amenorrhea. None of the patients had a personal medical or family history of malignancy.
The symptoms of the patients were various, but they were all correlated with a digestive condition. The patient with colon cancer, at the time of the admission in our hospital, had abdominal pain, constipation and a history of multiple hospitalizations for sub-occlusive episodes. Both patients with gastric cancer presented nausea and fatigue in the moment of the hospitalization. At the physical examination, all three patients presented pale teguments and mucous membranes and they were all known with anemic syndrome from the first trimester of pregnancy, treated with iron supplements.
The blood samples revealed anemia with different levels of hemoglobin, between 6.5 g/dL and 9.2 g/dL. In both patients with gastric cancer, severe thrombocytopenia (between 7000/mmc and 41000/mmc) and hypofibrinogenemia (between 122 mg/dl and 200 mg/dl) were detected, while hepatic and renal tests were normal. The patient with colon cancer had the liver markers seriously modified, with high levels of direct bilirubin, fibrinogen and transaminases.
All three patients were tested for tumor markers: alpha-fetoprotein, carcinoembryonic antigen, CA 125 and CA 19-9. The alpha-fetoprotein and CA 19-9 were elevated in all cases, and CA 19-9 had levels between 440 U/ml and more than 2000 U/ml. The patient with 23 weeks of pregnancy and gastric cancer and the patient with colon cancer had a positive result for CA 125.
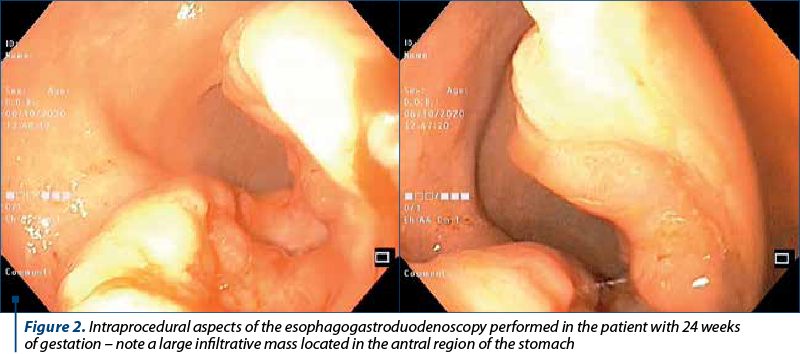
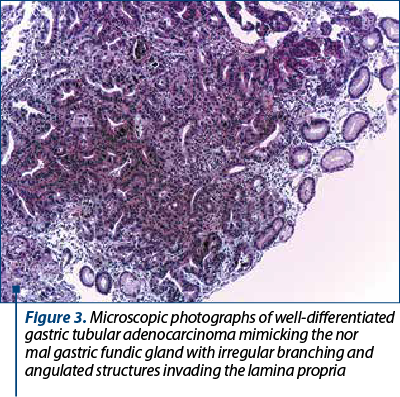
In both patients with gastric cancer, a bone marrow trephine biopsy was performed. It suggested metastases with a high suspicion of a primary gastric tumor, therefore an esophagogastroduodenoscopy was realized, which detected an infiltrative mass in the stomach body (Figure 2). Biopsies were taken and the histopathological examination confirmed the diagnosis of gastric cancer (Figure 3 and Figure 4).
All three patients underwent an abdominal ultrasound examination. The patient with colon cancer had severe hepatomegaly, the patient with 23 weeks of pregnancy had suggestive images for hepatic metastases, adenopathy and splenomegaly, and the other patient with gastric cancer had only a mild hepatomegaly.
Regarding the obstetrical exam, the patients with viable pregnancy had no clinical features or signs of preterm labor. All three pregnancies were periodically evaluated by ultrasound. Both pregnancies developed with no issues related to the fetus, such as intrauterine growth restriction or small for gestational age.
The patient with colon cancer and the one with gastric cancer and 24 weeks of pregnancy benefited from an MRI scan, which revealed, in the patient with colon cancer, lesions with malignant features in the hepatic parenchyma or metastases from an extrahepatic source, while the other patient had pelvic bone metastases. The other patient with gastric cancer benefited from an emergency CT scan, confirming the multiple metastases and the adenopathy.
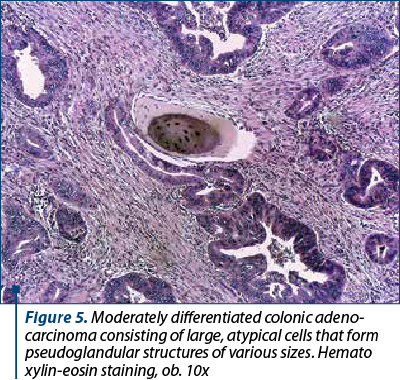
The evolution of the pregnant woman with 23 weeks of gestation and gastric cancer was extremely aggressive and after four days of hospitalization she suffered a cardiac arrest. For the patient with colon cancer, a caesarean section at 33 weeks of pregnancy was performed and a single live male fetus, weighting 1750 grams, with an Apgar score of 8, was extracted. During the surgery, the right ovary appeared with malignant modifications and the histopathological exam revealed a colonic-type adenocarcinoma – Krukenberg tumor, the certain diagnosis (Figure 5). After almost one month, she received chemotherapy. The patient with 24 weeks of pregnancy and gastric cancer was stabilized and after 10 days she was released and started chemotherapy.

Discussion
Anemia as a sign of neoplasia associated to pregnancy
In our unit, a third-degree maternity, the incidence of pregnancy-associated anemia was 15.1%, a percentage that corresponds to the analysis of 563 cases of pregnancy-associated anemia. Obviously, the incidence of anemia in the pregnant population is much higher, considering that only severe cases of anemia or cases associated with other pathologies are admitted. According to the World Health Organization, anemia becomes a severe public issue if the incidence in a population study exceeds 5%(9).
As revealed by Figure 1, the proportion of other digestive disorders associated with anemia in pregnancy barely reaches 1%.
Although a rare and challenging condition, cancer during pregnancy should rapidly be identified and treated(10). Fetal safety might be weighted for clinical decisions(10). Anemia caused by blood loss is the most frequent in cancer during pregnancy(10). At the outset, anemia can be mild and considered physiological in pregnancy, but the symptoms worsen as anemia worsens(10-12).
Gastric cancer, especially undifferentiated adenocarcinoma associated with diffuse bone metastasis accompanied by hematological disorders, is exceptionally encountered and the prognosis is very poor(13). A mean survival time of 4-5 months was attributed to gastric cancer with bone metastasis(14). As in many other complicated cases, the multidisciplinary approach is an essential key.
The screening and diagnosis of anemia in the first trimester are of extreme importance for an easier differential diagnosis, for a better prognosis and an appropriate subsequent management. In the case of advanced, life-threatening disease as the main cause of anemia, the medical interruption of pregnancy can be accepted and therefore an adequate complete treatment can be initiated.
Pregnancy-associated digestive cancer
We presented three cases of digestive malignancy during pregnancy on a period of three years(15,16). Gastric and colon cancers during pregnancy are rare conditions. In a study that included 227 cases of cancer during pregnancy, digestive malignancies represented almost 4.5% of all cases(17).
Digestive neoplasms can present signs and symptoms that can be easily confused with normal manifestations during pregnancy. As we presented, anemia was a common sign in all three cases(15,16). Pregnant women with hemoglobin level under 11g/dL in the first and third trimesters and under 10.5 g/dL in the second trimester are considered to have anemia(18-19). It is important to note that anemia was present from the first trimester of pregnancy in both patients with gastric cancer, but since it is a sign that can mimic the symptoms of pregnancy, the diagnosis was established later(19).
Regarding tumor markers, their sensitivity and specificity may be lower in pregnant women(18). CA 125 and alpha-fetoprotein are physiologically elevated in pregnancy(19,21,22). However, in all our cases, tumor markers were very high and helped us making a presumptive diagnosis(15,16).
Imaging during pregnancy, with the purpose to diagnose and stage the malignancy, should consider the risks for the fetus and the benefits for the mother(19). MRI is safe during pregnancy and is the best choice for cancer’s diagnosis and staging(19,23). Therefore, in two of our cases, the patients benefited from MRI and it was the one technique which staged the neoplasia. Even though CT scan should be avoided due to cumulative radiation(20,24), it was performed in one of our cases as an emergency exam because of her poor prognosis and the viability of the fetus.
The definitive diagnosis of tumor type and grading were provided by histopathological examination(19). In both our patients with gastric cancer, an upper gastrointestinal endoscopy was performed with multiple biopsies(16). In the patient diagnosed with colon cancer, the definitive diagnosis was established during caesarean section(15). In a study on 41 pregnant patients with colon-rectal neoplasia, 10 patients were diagnosed during acute surgery, but the others were diagnosed using endoscopy with biopsy, MRI or CT scan(25).
The oncologic management should be personalized depending, on one hand, on the type of cancer, tumor biology and staging, and on the other hand, on the viability and safety of the fetus(19). Chemotherapy has teratogenic risks, but it depends on gestational age, agent and dose, and the first trimester is the highest risk period. Because of the benefits to the mother, in many cases the assumption is warranted of risks related to chemotherapy exposure, especially during the second and third trimesters(19). The patient with gastric cancer and viable pregnancy received chemotherapy, while the patient with colon cancer received chemotherapy after surgery.
Conclusions
Digestive cancer during pregnancy may present different signs and symptoms that can be masked by those of pregnancy. It is important to determine the type of anemia from the first trimester of pregnancy and to make possible to have a certain diagnosis as soon as possible, because digestive cancer in women of reproductive age has a poor prognosis. The diagnosis represents a challenge and the treatment requires a multidisciplinary team.
Acknowledgement: We would like to thank our colleagues from the Bucharest University Emergency Hospital who participated in the multidisciplinary management of the pregnant patients diagnosed with digestive cancers: Ana Maria Vlădăreanu, Minodora Onisăi, Irina Voican, Andreea Marinescu, Andreea Bucur, Erika Oprea, Daniel Voiculescu and Petruţa Violeta Filip.
Conflict of interests: The authors declare no conflict of interests.
Bibliografie
-
Locktich G. Clinical biochemistry of pregnancy. Crit Rev Clin Lab Sci. 1997;34(1):67-139.
-
Rodger M, et al. Haematological problems in obstetrics. Best Prac Res Clin Obstet Gynaecol. 2015;29(5):671–84.
-
Ramsay M. The Obstetric Hematology Manual. Cambridge: Cambridge University Press. Normal hematological changes during pregnancy and the puerperium. In Pavord S, Hunt B (ed). 2010:3–12.
-
Wilson M, et al. Blood pressure, the renin-aldosterone system and sex steroids throughout normal pregnancy. Am J Med. 1980;68(1):97–104.
-
Davison JM. Renal haemodynamics and volume homeostasis in pregnancy. Scand J Clin Lab Invest Suppl. 1984;169:15–27.
-
Tkachenko O, et al. Hormones and hemodynamics in pregnancy. Int J Endocrinol Metab. 2014;12(2):e14098.
-
Sifakis S, Pharmakides G. Anemia in pregnancy. Ann NY Acad Sci. 2000;900(1):125-36.
-
Xiong X, et al. Anemia during pregnancy and birth outcome: a meta-analysis. Am J Perinatol. 2000;17(3):137-46.
-
Worldwide prevalence of anaemia 1993-2005: WHO global database on anaemia, 2008. https://www.who.int/nutrition/publications/micronutrients/anaemia_iron_deficiency/9789241596657/en/
-
Breymann C. Iron deficiency anemia in pregnancy. Semin Hmatol. 2015;52(4):339-47.
-
Donegan WL. Cancer and pregnancy. CA Cancer J Clin. 1983;33(4):194–214.
-
Jhaveri MB, et al. Melanoma in pregnancy. Clin Obstet Gynecol. 2011;54(4):537–45.
-
Etoh T, et al. Diffuse bone metastasis with hematologic disorders from gastric cancer: clinicopathological features and prognosis. Oncol Rep. 1999;6(3):601-5.
-
Hussain S, Chui S. Gastric carcinoma presenting with extensive bone metastases and marrow infiltration causing extradural spinal haemorrhage. Brit J Radiol. 2006;79(939):261–3.
-
Munteanu O, et al. Colon cancer in pregnancy: a diagnostic and therapeutic challenge. Rom J Morph Embryol. 2019;60(1):307-17.
-
Onisăi M, Vlădăreanu AM, Iordan I, Bumbea H, Nica A, Aliuş C, Grădinaru S, Bohîlţea R, Cîrstoiu M. Pregnancy-associated gastric cancer: Real-life diagnosis and management. Pharmacophore. 2020;11(3):89-92.
-
Sekine M, et al. Malignancy during pregnancy in Japan: an exceptional opportunity for early diagnosis. BMC Pregnancy Childbirth. 2018;18(1):50.
-
Prasetya P, et al. Anemia in the first trimester is associated with anemia during pregnancy in Sidotopo Wetan Community Health Center, Surabaya. Majalah Obstetri Ginekologi. 2020;28(1):16-9.
-
Silverstein J, et al. Multidisciplinary management of cancer during pregnancy. JCO Oncology Practice. 2020;16(9):545-57.
-
Han S, et al. Physiologic variations of serum tumor markers in gynecological malignancies during pregnancy: a systematic review. BMC Med. 2012;10(1):86.
-
Sarandakou A, et al. Tumor markers in biological fluids associated with pregnancy. Crit Rev Clin Lab Sci. 2007;44(2):151-78.
-
Moore R, et al. Serum levels of the ovarian cancer biomarker HE4 are decreased in pregnancy and increase with age, Am J Obst Gynecol. 2012;206(4):349-e1.
-
Michielsen K, et al. Whole-body MRI with diffusion-weighted sequence for staging of patients with suspected ovarian cancer: a clinical feasibility study in comparison to CT and FDG-PET/CT. Europ Radiol. 2014;24(4):889-901.
-
Wang PI, et al. Imaging of pregnant and lactating patients: part 2, evidence-based review and recommendations. Am J Roent. 2012;198(4):785-92.
-
Kocián P, de Haan J, Cardowick EH, Uzan C, Lok CAR, Fruscio R, et al. Writing Committee of the International Network on Cancer, Infertility and Pregnancy (INCIP) on this particular manuscript, Management and outcome of colorectal cancer during pregnancy: report of 41 cases. Acta Chir Belg. 2019;119(3):166-75.
Articole din ediţiile anterioare
OBSTETRICS | Ediţia 2 28 / 2020
Tumoră spinală cervicală asociată sarcinii
Oana Bodean, Mirela Moarcăş, Diana Ioana Voicu, Octavian Munteanu, Luciana Grozavu-Arsene, Florina Păuleț, Monica Mihaela Cîrstoiu
Tumorile spinale sunt rar întâlnite în sarcină, dar atunci când sunt extinse, pot cauza probleme grave prin efectele neurologice rapid progresiv...
18 mai 2020
OBSTETRICS | Ediţia 3 25 / 2019
Diagnosticarea şi managementul emboliei pulmonare în rândul pacientelor gravide
Aida Petca, Ana Maria Plopan, Răzvan Petca, Nicoleta Măru, I. Pacu, Mona Elena Zvâncă
Embolia pulmonară este una dintre situaţiile de urgenţă care necesită multă pregătire şi un simţ clinic foarte bine dezvoltat pentru a evita scenar...
20 septembrie 2019
GINECOLOGIE | Ediţia 6 (4) / 2014
Principii de tratament cu metotrexat al sarcinii extrauterine necomplicate
Diana Ioana Voicu, Octavian Munteanu, Costin Berceanu, Monica Mihaela Cîrstoiu
Sarcina extrauterină reprezintă o urgenţă ginecologică severă care, în lipsa unui diagnostic stabilit corect şi rapid, precum şi a unei intervenţii...
15 noiembrie 2014
OBSTETRICĂ | Ediţia 10 (4) / 2015
Infecţia cu Virusul Herpes Simplex în sarcină
Payam Behzadi, Elham Behzadi, Reza Ranjbar, Esmaiel Saberfar, Saeed Morovvati
Infecţia cu virusurile Herpes Simplex (VHS) reprezintă un grup complex de infecţii, care pot avea drept gazdă organismul uman. Există două tipuri d...
15 noiembrie 2015