Pelvic organ prolapse has become a common problem among women and, because of its increasing incidence, several surgical techniques have been developed. The current gold standard surgical repair for pelvic organ prolapse is the abdominal sacrocolpopexy, because of its high success rate and excellent anatomic outcome. Laparoscopic sacrocolpopexy has become an alternative for the abdominal approach. The aim of this systematic review is to compare the advantages and disadvantages between the laparoscopic sacrocolpopexy and the abdominal sacrocolpopexy.
GYNECOLGY
Sacrocolpopexia – avantaje şi dezavantaje între abordul abdominal şi cel laparoscopic. Sinteză sistematică şi metaanaliză
Sacrocolpopexy – advantages and disadvantages of abdominal and laparoscopic approaches. A systematic review and meta-analysis
Șef de lucrări dr. Mihai Dumitraşcu,
Răzvan Fodoroiu,
Cătălin George Nenciu,
Florica Şandru,
Aida Petca,
Răzvan Petca,
Monica Mihaela Cîrstoiu
First published: 12 decembrie 2019
Editorial Group: MEDICHUB MEDIA
DOI: 10.26416/Gine.26.4.2019.2711
Abstract
Rezumat
Prolapsul genital a devenit o afecţiune frecventă în rândul populaţiei de sex feminin. În urma creşterii incidenţei, au fost dezvoltate diferite tehnici chirurgicale pentru refacerea tulburărilor de statică pelviană. Standardul de aur în managementul acestei patologii a devenit sacrocolpopexia folosind abordul clasic abdominal, datorită rezultatului anatomic excelent şi eficienţei metodei. Abordul laparoscopic în sacrocolpopexie a devenit o alternativă la abordul clasic. Scopul acestei sinteze este de a compara şi prezenta avantajele şi dezavantajele celor două modalităţi de abord al sacrocolpopexiei.
Introduction
Pelvic organ prolapse (POP) is known to affect 30% of women aged 50-89 years old, and it is predicted that the morbidity of POP will increase by more than 40% over the next 40 years(1). The procedure for POP repair must be safe, effective, with a low recurrence rate, and must improve sexual and urinary functions(2).
The current gold standard in the treatment of POP is the abdominal sacrocolpopexy (ASC). In comparison with the sacrospinous ligament fixation, ASC is associated with longer recovery time and operative time, but has a higher success rate, with less dyspareunia(3,4). Over the past decades, the laparoscopic-assisted sacrocolpopexy (LSC) has become available, with similar overall results as the abdominal approach. Although LSC is less invasive, it requires greater surgical skills in order to determine the proper plans for safe and effective dissection of the rectovaginal and vesicovaginal spaces(5).
The aim of this study was to compare the advantages and disadvantages of different sacrocolpopexy techniques, and to perform a systematic review of the outcomes.
Materials and method
A systematic review and meta-analysis was performed. Abstracts and studies were selected using Medline search after applying exclusion and inclusion criteria. A single investigator reviewed the studies and the abstracts. The study selection process is demonstrated in Figure 1. After meeting the inclusion criteria, studies were later excluded from the review based on the exclusion criteria.
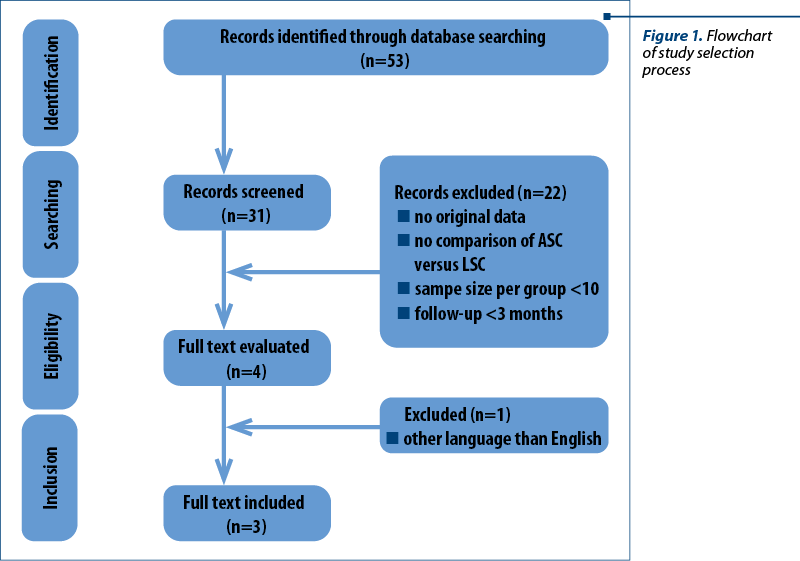
The inclusion criteria were: published original research, comparison of the outcomes of ASC and LSC, sample size in each group greater than 10, and the follow-up duration more than three months. Studies were excluded if the language was not English, and if the results of the studies did not include comparable results.
Results
Characteristics of the selected studies
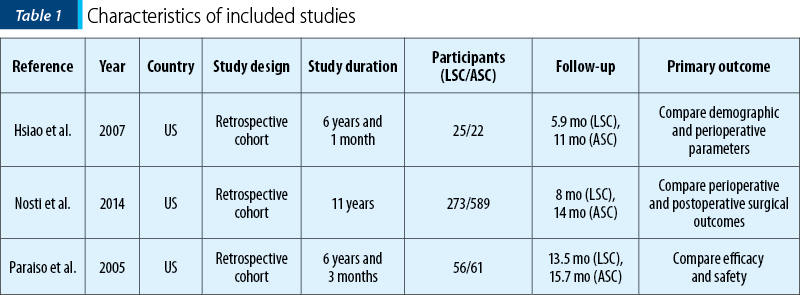
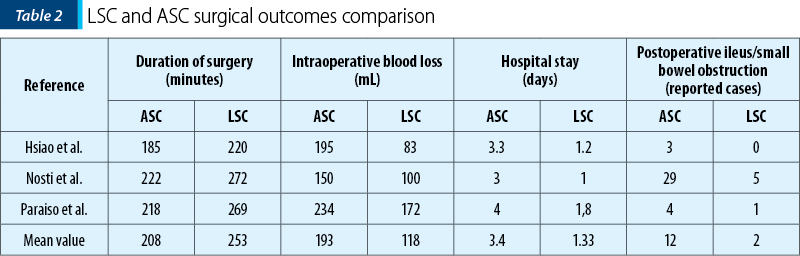
A total of 53 papers were initially identified. Three studies, including 996 patients, were retrieved(6-8). Overall, a number of 672 patients underwent ASC and 354 underwent LSC. The mean follow-up duration was 13.5 months after ASC and 9.1 months after LSC. Studies included women undergoing concomitant vaginal repair and anti-incontinence surgery. Paraiso et al. study also included five women who underwent bowel resection due to rectal prolapse associated with constipation symptoms(8). Table 1 summarizes the studies characteristics. Table 2 summarizes the surgical outcomes comparison between LSC and ASC.
Synthesis of results
Duration of surgery. The duration of surgery was 17.8% shorter in the ASC group in comparison with the LSC group. This analysis was performed on all three studies that involved 672 patients who underwent ASC and 354 patients with LSC. The mean operation time for ASC was 208 minutes, in comparison with 253 mean operation time for LSC. The difference in the duration of surgery was 45 hours(6-8).
Blood loss. Intraoperative mean blood loss in the ASC group was 193 mL, being 63% higher than in the LSC group, which had a significantly lower mean intraoperative blood loss of 118 mL(6-8).
Hospital stay. ASC was associated with greater hospital stay (mean hospital stay of 3.4 days) compared with LSC (mean hospital stay of 1.33). This result estimated that LSC had a 61% shorter hospital stay(6-8).
Postoperative ileus/small bowel obstruction (SBO). It is well known that laparoscopical approach offers a lower rate of complications. ASC is thus associated with increased risk of postoperative ileus and small bowel obstruction. Nosti et al. reported 29 cases (out of 273 patients) of ileus and SBO in the ASC group. The other two groups only reported seven cases in total. Out of a total of 672 patients who underwent ASC, 5.35% had ileus and SBO complications. As a comparison, the LSC group reported only six cases, which represented 1.69% of the patients enrolled in these studies(6-8).
Bladder and bowel injury. There was no significant difference in rate of bowel and bladder injury between the two groups(6-8).
Reoperation for prolapse surgery. There was no significant difference in the rate of reoperation for prolapse surgery between ASC and LSC groups. ASC had one case of repeated surgery in the group from Nosti et al. Regarding LSC, Paraiso et al. reported one case of repeated surgery for apical recurrence, and Nosti et al. also reported one repeated surgery for apical recurrence in the LSC group(6-8).
Discussion
This systematic review found that the laparoscopic approach in sacrocolpopexy has the advantage of less blood loss, shorter hospital stay, less postoperative ileus/SBO, but a longer operation time compared with the abdominal approach. The findings reveal that there is no difference between the two methods regarding the need for further surgery and the risk of bowel or bladder injury(6-8).
Our results were similar with other meta-analyses regarding blood loss, hospital stay and surgery duration(5,9).
According to a recent systematic review(10) which compared ASC with LSC, the duration of surgery between the two approaches was 87 minutes. In our systematic review, we found a smaller difference in the duration of surgery of 45 minutes. This difference may be explained by the fact that surgeons with experience can perform the LSC much faster than surgeons who are still in the learning curve.
There is good evidence to support the laparoscopic approach due to the advantage of a shorter hospital stay and less blood loss, which can have a positive impact of the patients’ expectations of hospital care and service. Because the anatomical and combined outcomes were not very different between LSC and ASC, it is important to notice the fact that ASC had a shorter duration of surgery, which leads to a shorter anesthesia time for the patient.
Conclusions
The present systematic review indicates that ASC and LSC have similar clinical outcomes in prolapse surgery. The abdominal approach has a shorter surgery time, but is associated with greater blood loss, longer hospital stay, and has greater risk of postoperative ileus and small bowel obstruction. LSC represents a safe alternative to ASC, with similar anatomical results and with all the aforementioned advantages.
Conflicts of interests: The authors declare no conflict of interests.
Bibliografie
- Luber KM, Boero S, Choe JY. The demographics of pelvic floor disorders: current observations and future projections. Am J Obstet Gynecol. 2001; 184(7):1496–501.
- Culligan PJ, Murphy M, Blackwell L, Hammons G, Graham C, Heit MH. Long-term success of abdominal sacral colpopexy using synthetic mesh. Am J Obstet Gynecol. 2002; 187(6):1473–80, discussion; 1481–2.
- Benson J, Lucente V, McClellan E. Vaginal versus abdominal reconstructive surgery for the treatment of pelvic support defects: a prospective randomized study with long-term outcome evaluation. Am J Obstet Gynecol. 1996; 175:1418–22.
- Lo T, Wang A. Abdominal colposacropexy and sacrospinousligament suspension for severe uterovaginal prolapse: a comparison. J Gynaecol Surg. 1998; 14:59–64.
- Pan K, Zhang Y, Wang Y, Wang Y, Xu H. A systematic review and meta-analysis of conventional laparoscopic sacrocolpopexy versus robot-assisted laparoscopic sacrocolpopexy. Int J Gynecol Obstet. 2015; 132(3):284–91.
- Hsiao K, Latchamsetty K, Govier F, et al. Comparison of laparoscopic and abdominal sacrocolpopexy for the treatment of vaginal vault prolapse. J Endourol. 2007; 21:926–30.
- Nosti P, Andy U, Kane S, et al. Outcomes of abdominal and minimally invasive sacrocolpopexy: a retrospective cohort study. Female Pelvic Med Reconstr Surg. 2014; 20:33–7.
- Paraiso M, Walters M, Rackley R, et al. Laparoscopic and abdominal sacral colpopexies: a comparative cohort study. Am J Obstet Gynecol. 2005; 192:1752–8.
- Campbell P, Cloney L, Jha S. Abdominal versus laparoscopic sacrocolpopexy. Obstet Gynecol Survey. 2016; 71(7):435–42.
- De Sa M, Claydon L, Whitlow B, et al. Laparoscopic versus open sacrocolpopexy for the treatment of prolapse of the apical segment of the vagina: a systematic review and meta-analysis. Int Urogynaecol J. 2016; 27:3–17.