In Romania, postterm pregnancies are defined as pregnancies which last beyond 41 weeks and 0 days of gestation. The determination of the “true” postterm pregnancies remains challenging, due to incorrect gestational dating. Therefore, it is widely accepted that the ultrasonographic measurement of crown-rump length (CRL) (having an error of 4.7 days) is the most accurate method of dating gestational age, being superior to exclusively second-trimester fetal biometry. The maternal complications rise exponentially through the five weeks of “term” pregnancies. The pathophysiological basis for the increased fetal risk in postterm pregnancies is unclear, although it has been long suggested the role played by the placental senescence; the most frequently associated fetal risk of the postterm pregnancy is the meconial aspiration syndrome. Thus, the question remains: when should the intervention for delivery outrun the expectative management? The delivery becomes necessary when the fetal and/or maternal risks associated with the continuation of pregnancy are greater than those faced after delivery.
Sarcina depăşită cronologic – riscuri şi management
Postterm pregnancy – risks and management
First published: 20 septembrie 2019
Editorial Group: MEDICHUB MEDIA
DOI: 10.26416/Gine.25.3.2019.2495
Abstract
Rezumat
În România, sarcina depăşită cronologic este definită ca o sarcină cu durată mai mare de 41 de săptămâni şi 0 zile. Determinarea unei sarcini „adevărate” suprapurtate rămâne în schimb o provocare, din cauza datării incorecte a vârstei gestaţionale. Astfel, este acceptat pe scară largă că măsurarea ultrasonografică în primul trimestru a lungimii cranio-caudale (CRL) embrionare (cu o eroare de 4,7 zile) este metoda cea mai precisă de a determina vârsta gestaţională, fiind superioară biometriei fetale exclusive din trimestrul al doilea. Complicaţiile materne cresc exponenţial pe perioada celor cinci săptămâni de gestaţie „la termen”. Baza fiziopatologică pentru creşterea riscului fetal în sarcina suprapurtată este neclară, deşi se consideră de mult timp teoria senescenţei placentare; complicaţia fetală asociată cu sarcina suprapurtată este sindromul de aspiraţie meconială. Astfel, întrebarea rămâne: la ce vârstă gestaţională intervenţia pentru naştere devansează managementul expectativ? Naşterea este indicată oricând riscul fetal şi/sau matern asociat cu continuarea sarcinii este mai mare decât cel preconizat după naştere.
Introduction
The gestational age which falls between 37 weeks, 0 days and 41 weeks, 0 days is considered to be a term pregnancy(1). According to the National Health Organization, postterm pregnancy is defined as having a gestational age over 42 weeks (over 294 days), beginning on the first day of the last menstrual cycle, and occurs in 1.5-10% of the total number of pregnancies(2). Prolonged pregnancy is stated as having a gestational age between 41 weeks, 0 days and 41 weeks, 6 days.
Determining a “true” postterm pregnancy remains a challenge due to the incorrect dating of the gestational age. Changes brought into the paraclinical methodology have led, however, to a decline in the number of postterm births. Determining gestational age by calculating time elapsed since the first day of last menstrual cycle usually leads to overestimation due to lengthy and often unpredictable follicular phase. Ultrasound dating reduces the risk of incorrectly labeling a pregnancy as postterm. It is therefore widely accepted that first-trimester ultrasound measuring of embryo CRL (crown-rump length) is the most precise method for determining gestational age, having an error margin of 4.7 days, superior even to second-trimester fetal biometry(3-5).
Risk factors for postterm pregnancy
The etiology of postterm pregnancy is usually poorly understood. Some of the known risk factors are listed in Table 1.

Perinatal mortality and morbidity
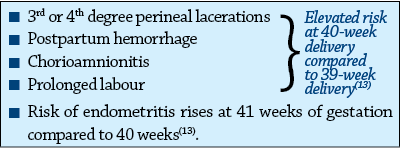
The risk of maternal complications during the five weeks of “term pregnancy” increases each week as follows:
The predominant cause of increased perinatal morbidity and mortality in postterm pregnancy is believed to be progressive uteroplacental insufficiency(14). Postterm newborns (over 41 weeks of gestation) show a higher rate of neonatal mortality compared to “term” newborns. The risk rises from 0.7% at 37 weeks, 0 days to 5.8% at 43 weeks, 0/7 days(1,15).
A study(16) which observed postterm and preterm children until preschool age has shown greater risk of emotional and behavioral issues compared to “term” born children. Particularly, the risk of attention deficit and hyperactivity disorder was nearly two-and-a-half times greater in postterm children(11). The cause appears to be lack of oxygen (uteroplacental insufficiency) during intrauterine period, due to deficient placental endocrine function; disturbance of the “placental clock” (responsible for the duration of pregnancy) leads to decreased secretion of the corticotropin-releasing hormone (CRH) – shown to be lower in postterm pregnant women. CRH is the main regulating factor of hypothalamic-pituitary-adrenal axis. Therefore, poor development of this axis can lead to neuroendocrine disorders which can cause behavioral issues and increased emotional vulnerability of affected children.
A study made by Danish National Birth Register between 1980 and 2001 has linked postterm pregnancy with a slightly higher risk of epilepsy in children aged 0-1 years old(8).
The pathophysiological ground for increased fetal risk in postterm pregnancy is unclear, although placental senescence has long been considered(15). The most significant complication is intrauterine fetal demise, which has decreased considerably, in 2001 having been estimated at 1.6-3.5%(1). Meconial aspiration syndrome causes a notable degree of morbidity and mortality, being most clearly associated with postterm pregnancy, with a risk of 0.24% at 38 weeks, 0 days, to 1.42% at 42 weeks, 6 days(1). A statistical analysis has shown an increased rate of meconial aspiration syndrome, C-section, and abnormal fetal heart rate in the expectant management group, compared to the above 41-week pregnancy group where labor was induced(17).
Other fetal complications include low Apgar score, neonatal convulsions (1.5 times greater(1)), fetal macrosomia (five times greater risk(1)), polycythemia, and neonatal sepsis (1.3 times greater risk).
Fetal evaluation
Studies are yet inconsistent regarding the type and frequency of antenatal assessment.
Despite the fact that there is no superior method for antenatal assessment of postterm pregnancy, most experts recommend external cardiotocography or biophysical profile and evaluation of amniotic fluid index twice weekly.
It is not recommended to measure the amniotic fluid index in the four quadrants (which defines oligohydramnios as lower that 5 cm); a single 2x2 cm amniotic fluid pocket is considered normal(1,8).
Expectant management versus delivery
If a low-risk pregnancy has reached 41 weeks, it can be approached either via expectant management, or labor inducing. The question remains: at what gestational age should intervention supersede expectant management?
When labor is not induced at 41 weeks, 7% of pregnancies reach 42 weeks, and 1.4% reach 43 weeks(5).
Delivery is recommended when fetal and/or maternal risk associated with continued pregnancy is greater than predicted postnatal risk.
High-risk pregnancies (diabetes mellitus, arterial hypertension, or maternal age above 35 years old) are most suitable for delivery around 38-39 weeks. The management of low-risk pregnancies is more controversial.
The decision to induce labor requires the consideration of several factors, including prenatal fetal assessment, (un)favorable cervical condition, gestational age, maternal risk factors and patient preference. At 41 weeks, 74% of patients prefer labor inducing(18).
A study conducted in England has noted shorter labors and more frequent and intense contractions in the group where labor was induced at 41 weeks compared to the expectant management group, regardless whether labor was later induced or spontaneous(18).
Analyzing the means to prevent postterm pregnancy, a Cochrane analysis has shown that inferior pole amniochorionic membrane sweep, with stimulation of Ferguson reflex in pregnant women who are close to their due date, reduced this risk. The number of inferior pole membrane sweep maneuvers necessary to prevent chemically induced labor was eight(8).
Expectant management does involve elevated anxiety in patients, however they do not perceive it to be a significant medical issue(5). The American College of Obstetricians and Gynecologists deems inducing labor as recommended at 41 (0/7) weeks, and mandatory at 42 (0/7) weeks(15).
Delivery
-
Additional situations where inducing labor is recommended(8):
-
Oligohydramnios assessed via ultrasound.
Non-reactive cardiotocography with positive oxytocin test or biophysical profile greater than 6.
A predictive clinical factor for favorable induction of labor is a Bishop score (it assesses fetal station and cervical dilation, ripening, consistency and position) of more than 6. A study found that cervical shortening and low BMI are better predictive factors than the Bishop score(8).
For inducing labor, the election method consists of administering prostaglandins, except in case of scarred uterus – the risk of uterine rupture being higher with prostaglandins (2.45%) than with oxytocin (0.7%)(1,24).
Therefore, labor should not be induced in case of scarred uterus, spontaneous labour at 38-39 weeks having a better prognosis than prostaglandin-induced labor.
Prostaglandins may be administered intravaginally or orally; some studies claim the superiority of oral administration for inducing labor(20).
The recommended dose for inducing labour is 25-50 µg(21,22). Prostaglandin tablets available in Romania are between 100 and 200 µg, requiring the obstetrician to fragment them.
The recommended treatments are one tablet at 6-hour cycles (maximum of two doses – a second dose only if labor has not commenced), or one cycle of prolonged-release prostaglandin (one dose every 24 hours)(23).
In Romania, the only prostaglandin product designed for inducing labor is a controlled-release vaginal device, which releases misoprostol at approximately 7 micrograms per hour for 24 hours (Misodel® 200 micrograms, vaginal release system, FERRING GMBH – Germany).
Another means for triggering labor is oxytocin administration, used in case of favorable cervical conditions (Bishop score of 5).
A study has shown the effectiveness of administering prostaglandins vaginally, 12 hours before administering oxytocin: prostaglandins bear a tight interaction with oxytocin, mobilizing the arachidonic acid in membrane phospholipids and initiating cyclooxygenase gene 2 transcription, which ensures the continuous synthesis of prostaglandins(21).
The C-section recommendation for fetal distress has been examined for each week, at 39 weeks being 13.7%, at 40 weeks – 19.6%, rising to 23.5% at 41 weeks, and to 27.5% at 42 weeks(13).
A study found an increased risk of C-section between weeks 40 and 41 – 9% and 14% respectively, rising as high as 21.7% in pregnancies over 42 weeks(13). This risk has been noted to be greater in nulliparous cases compared to multiparous ones. The risk of instrument-assisted delivery is double at 42 weeks (17.4%) compared to 9.4%(13).
Conclusions
The management of postterm pregnancies remains a challenge for obstetricians, deciding which patients are indicated to have labor induced, which will respond to induction, and which ones require C-section.
Fetal, neonatal and maternal complications associated with postterm pregnancies have always been underestimated. This is the reason why ultrasound screening during the first trimester will reduce the number of false diagnoses of postterm pregnancies.
Regarding the management, numerous Cochrane analyses have shown that inducing labor at 41 weeks yields a lesser risk of perinatal mortality and morbidity, when compared to expectant management. At this gestational age, it is pertinent to consider the chemical termination of pregnancy.
Conflict of interests: The authors declare no conflict of interests.
Bibliografie
- Vayssiere C, Haumonte JB, Chantry A, Coatleven F, Debord MP, Gomez C, Sentilhes L. Prolonged and post-term pregnancies: guidelines for clinical practice from the French College of Gynecologists and Obstetricians (CNGOF). Eur J Obstet Gynecol Reprod Biol. 2013; 69(1):10-6.
- Kortekaas JC, Kazemier BM, Ravelli AC, De Boer K, Van Dillen J, Mol B, De Miranda E. Recurrence rate and outcome of postterm pregnancy, a national cohort study. Eur J Obstet Gynecol Reprod Biol. 2015; 193:70-4.
- Bennett KA, Crane JMG, O’Shea P, Lacelle J, Hutchens D, Copel JA. First trimester ultrasound screening is effective in reducing postterm labor induction rates: A randomized controlled trial. Am J Obstet Gynecol. 2004; 190(4):1077-81.
- Bruckner TA, Cheng YW, Caughey AB. Increased neonatal mortality among normal-weight births beyond 41 weeks of gestation in California. Am J Obstet Gynecol. 2008; 199(4):421.e1-421.e7.
- Mandruzzato G, Alfirevic Z, Chervenak F, Gruenebaum A, Heimstad R, Heinonen S, Thilaganathan B. Guidelines for the management of postterm pregnancy.
- J Perinat Med. 2010; 38(2):111–9.
- Sanchez-Ramos L, Olivier F, Delke I, Kaunitz AM. Labor induction versus expectant management for postterm pregnancies: a systematic review with meta-analysis. Obstet Gynecol. 2003; 101(6):1312-8.
- Laursen M, Bille MC, Olesen AW, Hjelmborg J, Skytthe A, Christensen K. Genetic influence on prolonged gestation: A population-based Danish twin study. Am J Obstet Gynecol. 2004; 190(2):489-94.
- Wang M, Fontaine P. Common questions about late-term and postterm pregnancy. Am Fam Physician. 2014; 90(3):160-5.
- American College of Obstetricians and Gynecologists. Practice bulletin no. 146: Management of late-term and postterm pregnancies. Obstet Gynecol. 2014; 124(2 Pt 1):390.
- Zvâncă ME, Petca A, Boţ M. Progesterone, vitamins, metformin during pregnancy – “myth” or evidence-based medicine?. Ginecologia.ro. 2016; 4(14): 14-7.
- Taipale P, Hiilesmaa V. Predicting delivery date by ultrasound and last menstrual period in early gestation. Obstet Gynecol. 2001; 97(2):189-94.
- Milulescu A, Vlădăreanu S, Vlădăreanu R. Etiology and pathogenic mechanism of neonatal hypoxic-ischemic encephalopaty. Ginecologia.ro. 2016; 4(13):30-1.
- Caughey AB, Stotland NE, Washington AE, Escobar GJ. Maternal and obstetric complications of pregnancy are associated with increasing gestational age at term. Am J Obstet Gynecol. 2007; 196:155.e1-155.e6.
- Savitz DA, Terry Jr JW, Dole N, Thorp Jr JM, Siega-Riz AM, Herring AH. Comparison of pregnancy dating by last menstrual period, ultrasound scanning, and their combination. Am J Obstet Gynecol. 2002; 187(6):1660-6.
- Maoz O, Wainstock T, Sheiner E, Walfisch A. Immediate perinatal outcomes of postterm deliveries. J Matern Fetal Neonatal Med. 2018; 32(11):1847-52.
- El Marroun H, Zeegers M, Steegers EAP,van der Ende J, Schenk JJ, Hofman A, Tiemeier H. Post-term birth and the risk of behavioural and emotional problems in early childhood. Int J Epidemiol. 2012; 41(3):773–81.
- Senat MV. Management of postterm pregnancies: the role for AFI, biophysical score and Doppler. J Gynecol Obstet Bio R. 2011; 40(8):785–95.
- Heimstad R, Romundstad PA, Hyett J, Mattsson KE, Kjell A. Women’s experiences and attitudes towards expectant management and induction of labor for post-term pregnancy. Acta Obstet Gyn Scan. 2007; 86(8):950-56.
- Elden H, Hagberg H, Wessberg A, Sengpiel V, Herbst A, Bullarbo M, Stephansson O. Study protocol of SWEPIS a Swedish multicentre register based randomised controlled trial to compare induction of labour at 41 completed gestational weeks versus expectant management and induction at 42 completed gestational weeks. BMC Pregnancy Childbirth. 2016; 16(1):49.
- Alfirevic Z, Aflaifel N, Weeks A. Oral misoprostol for induction of labour. Cochrane Database Syst Rev. 2014; 13(6):Cd001338.
- Pimentel VM, Arabkhazaeli M, Moon JY, Wang A, Kapedani A, Bernstein PS, Tropper PJ. Induction of labor using one dose vs. multiple doses of misoprostol: a randomized controlled trial. Am J Obstet Gynecol. 2018; 218(6):614-e1.
- Weeks AD, Navaratnam K, Alfirevic Z. Simplifying oral misoprostol protocols for the induction of labour. BJOG. 2017; 124(11):1642-5.
- Boulvain M, Kelly AJ, Irion O. Intracervical prostaglandins for induction of labour. Cochrane Database Syst Rev. 2008; 23(1):CD006971.
- Boţ M, Borislavschi A, Ichim M, Vlădăreanu R, Vlădăreanu S. Indications and contraindications of vaginal birth post C-section. Ginecologia.ro. 2017; 5(18):8-10.
Articole din ediţiile anterioare
Actualităţi în conduita terapeutică a ruperii premature şi precoce a membranelor
Ruperea prematură şi precoce a membranelor fetale (PPROM) se referă la ruperea membranelor înainte de 37 de săptămâni de gestaţie, în absenţa trava...