Caesarean section is one of the most common abdominal surgeries that do not benefit from a standard technique. The short-term and long-term consequences of the intervention depend on the technique used at each stage of the procedure, the choice of method being essentially influenced by the knowledge of anatomical landmarks and scientific evidence. The objective of our review is to provide updated evidence-based guidance for surgical decisions during caesarean delivery. We focused on the requirements of the uterine closure at the time of caesarean section, with emphasis on the woman’s reproductive desires. The conventional double-layer and single-layer suturing are discussed in this paper, with regard to full thickness healing of the cut margins. The quality of the cut margins of the uterus due to the process of labor on a prior scared uterus may lead to the poor healing of the uterine wall and results in thinned out scars.
Tehnici de sutură în operaţia cezariană
Suture techniques in caesarean section
First published: 30 septembrie 2020
Editorial Group: MEDICHUB MEDIA
DOI: 10.26416/Gine.29.3.2020.3767
Abstract
Rezumat
Operaţia cezariană este una dintre cele mai frecvente intervenţii chirurgicale abdominale ce nu beneficiază de o tehnică standard. Consecinţele pe termen scurt şi pe termen lung ale intervenţiei depind de tehnica folosită în fiecare etapă a procedurii, alegerea metodei fiind influenţată, în esenţă, de cunoaşterea reperelor anatomice şi de dovezile ştiinţifice. Obiectivul review-ului nostru este de a oferi un ghid actualizat bazat pe dovezi ştiinţifice, în vederea ghidării deciziilor chirurgicale în timpul operaţiei cezariene. Ne-am concentrat pe cerinţele suturii uterine în momentul intervenţiei de cezariană, punând accentul pe viitorul obstetrical al pacientei. Sutura convenţională cu două straturi şi cea monostrat sunt discutate în această lucrare, din punctul de vedere al menţinerii grosimii marginilor tăiate. Calitatea marginilor de incizie a uterului, din cauza travaliului la un uter cu o cicatrice precedentă, poate duce la o vindecare deficitară a peretelui uterin şi are ca rezultat obţinerea unei subţieri a cicatricei uterine.
Introduction
One of the most commonly performed surgeries is caesarean section, which can be performed both as elective or urgent procedure. However, once scarred, the uterus could carry long-term consequences, such as an increased risk of placenta accreta spectrum and uterine rupture in subsequent pregnancies. This leads to an increased rate of repeat caesarean delivery to minimize those risks(1,2). A key step in caesarean section is the closure of the uterine incision using an optimal surgical technique that allows the uterine scar created to withstand the stress of subsequent labor. There are two common techniques of suture of uterine closure: (a) single layer and (b) double layer. It is known that closing the transverse uterine incision using a single running locking suture penetrating the full thickness of the myometrium and endometrium is associated with an up to four-fold risk of uterine rupture compared to double-layer closure. Most randomized studies do not evaluate the impact on future pregnancies since, intraoperatively, the focus is on short-term operative complications(2-4). Recently, in the CAESAR collaborative(5) and the CORONIS collaborative(6), more than 18,000 women were randomized to single- or double-layer uterine closure in order to answer the long-standing question whether the technique of double-layer closure of the uterus at the time of caesarean lowers the risk of subsequent uterine rupture(5).
Other techniques of closing the uterine incisions have been proposed. One of the most interesting is the one performed by Babu and Magon on a patient who was a known case of fibroid uterus and had a post lower segment caesarean section pregnancy (LSCS)(1). The patient was unwilling to undergo vaginal birth after caesarean (VBAC), so a pre-labor caesarean was performed by the authors. Intraoperatively, they observed that the previous uterine scar was very thin. This led to excise the thinned out margins and sutured the uterine closure by a new technique, developed by them – shortly, their technique imply that the uterus is closed with delayed absorbable suture polyglactin 9/10 (0) or PGA (0), by continuous modified mattress suture technique in a single layer, excluding the decidual layer. Their aim was to ensure the correct anatomical approximation of the decidua-to-decidua, myometrium-to-myometrium and serosa-to-serosa layers. Subsequently, the patient underwent hysterectomy at a later stage because of the symptomatic fibroids. Once removed, the site of the uterine scar repaired by the new technique showed no thinning at the site of uterine repair. When compared with another post-caesarean uterus sutured with conventional double-layer technique, the authors observed thinning at the uterine rent repair site in the latter. However, the authors did not measure the thickness of scar site and did not use it as the final predictor of uterine scar strength.
In the present study, we try to identify the optimal way to close the uterus at the time of caesarean, and to evaluate the healing of the scar.
Results
Incision types
There are two common types of suprapubic abdominal wall transverse incisions, characterized postoperatively by reduced pain, increased tensile strength and superior cosmetic results: (a) the Pfannenstiel incision, introduced since 1900, which is slightly curved and practiced at 2-3 cm from the pubic symphysis extending to the caudal in the middle portion of the pubic hairline insertion; and (b) the Joel-Cohen incision, described in 1972, which is straight and performed 3 cm below the line which joins the anterosuperior iliac spines. The Pfannenstiel incision is slightly taller and longer compared to the Joel-Cohen incision. Rarely used, the Bardenheuer-Bastien incision is made from one iliac spine to the other, while the Rapin-Kustner incision cuts the skin crosswise and takes off the plane upper skin as much as possible to the umbilicus. The Maylard incision, introduced in 1907, is a cross section of the right abdominal muscles.
Median longitudinal incisions between the pubic and umbilical symphysis deal along the white line, with reduced bleeding and nerve damage, generally allow a faster penetration into the abdomen and an easy possibility of cranial extension left paraumbilical (to protect the round ligament of the liver)(8,9), if the access space needs to be wider, to the detriment of the cosmetic appearance. The superior speed of the longitudinal incision approach is a controversial issue(10). The caudal landmark of the incision is a point located 2-3 cm above the pubic symphysis; the size of the abdominal incision must be suitable for easy, atraumatic extraction of the fetus, 15 cm in the cranial direction being the minimum opening of the abdomen for a full-term fetus(11). The incision of the uterine wall in a caesarean section should consider the placental location, fetal size and position, and the level of progression of labor, which in the more advanced stages it relaxes the lower segment retracted above the presentation, in which case a lower incision may interest the cervix or even the vagina. The presence of leiomyomas is also a factor which customizes the decision of the operator. The hysterotomy, transverse or vertical, must allow the atraumatic extraction of the fetus. The uterine incision has traditionally been longitudinal; although in 1882 Kehrer introduced the transverse incision, demonstrating its advantages, it was not universally accepted until its reintroduction by Kerr in 1926(12). The transverse segmental incision (Monro Kerr/Kerr) is commonly used due to reduced bleeding and the low risk of uterine rupture during subsequent pregnancy. The disadvantage of this type of incision is the increased risk of uterine artery damage and its emergencies near the intersection with the ureter when the incision is significantly extended laterally; the extension of the incision in “J” or inverted “T” when widening is necessary. This often leads to poor quality uterine scars(13). Low vertical incisions (Kronig/De Lee/Cornell) performed at the non-contractile lower segment appear to be as resistant to scarring as those carried out at this level(14), provided that it is not prolonged uncontrollable to the uterine fundus or to the bladder, cervix or vagina. The classical vertical incision affects the upper uterine segment, and for this reason it is associated with increased maternal morbidity and a risk of dehiscence or rupture of the uterus in subsequent pregnancies of about 4-9%, compared to the risk of 0.2-1.5% which carries the low cross-segment incision(15). The generally accepted indications of vertical incision are the lack of development of the lower segment in terms of anticipating the need for maneuvers, low dorso-anterior transverse presentations or pelvic presentations with extreme prematurity, pathology of the lower uterine segment of the type voluminous leiomyomas, placenta praevia or anterior invasive or postmortem birth(13).
When comparing the skin incision type in the context of general approaches to caesarean delivery (Pfannenstiel, Joel-Cohen, Misgav-Ladach, modified Misgav-Ladach), four studies comparing Misgav-Ladache-based procedures with Pfannenstiel techniques noted improved operating times and possible cost savings in the former, with minimal difference in maternal morbidity(7,16-19). Studies using the Joel-Cohen surgical methods noted significantly improved short-term outcomes (less blood loss, less fever, lower duration of postoperative pain). Concerning the need to expand the uterine incision, blunt expansion remains preferred to sharp expansion of the uterine incision since it carries decreased maternal morbidity as measured by estimated blood loss and decrease in hemoglobin (with blunt cephalad-caudad expansion of the uterine incision)(20). When analyzing uterine exteriorization for hysterotomy repair, provider preferences (surgeon’s capability) should be accounted for, since febrile complications and surgical time were similar between uterine exteriorization and intraabdominal repair(7,21).
Sonography evaluated anatomical references
The optimal time for sonographic evaluation of the uterine scar in caesarean section is early follicular phase, in which the small size of endometrium facilitates the individualization of the myometrial scar. The transvaginal 2D approach is obviously superior to the transabdominal one, and gel instillation is more accurate than saline hysterography due to prolonged substance content at cavity level; data from literature support the twice as frequently detection of defects of the scar after caesarean section in case of examination with gel infusion compared to conventional transvaginal examination(22-24).
The sonographic examination of the uterus begins with the longitudinal plane; the internal cervical orifice is identified as the junction point between the endometrial cavity and the canal cervical. Uterine flexion is determined by identifying the angle between the longitudinal axis of the uterus and the longitudinal axis of the cervix. Uterine anteflexion is diagnosed by anterior deviation of the long axis of the uterine body from the long axis of the cervix; retroflexion is defined by establishing the axis deviation to the rear. Ultrasound individualization of the endometrium, hypoechoic middle muscle layer of uterus and vesicouterine fold, composed of hyperechoic peritoneal reflection above the muscle and mucosa of the bladder, allows the location of the uterine incision at the lower segment, optimally located 2-3 cm below the upper edge of the peritoneum of the vesicouterine fold. The transvaginal ultrasound detection of uterine scarring is easy performed by following the main principles: (1) setting the patient on a gynecology or obstetrics mode in the first trimester; (2) identifying the depth of the cervical canal and the segment in a panoramic view, subsequently magnifying the identified scar up to 75% of the screen; (3) setting the sector to maximum amplitude, targeting the area of intersection of the cervical axis with the uterine body axis; (4) clear identification of the cervical canal and the thin, hyperechoic internal cervical orifice located at the level of the uterine arteries and defined by the “V” appearance of the cranial extremity of the endocervical canal(25). The low-segment transverse scar after caesarean section is described as a hypoechoic identification of the anterior wall of the segment, located between the vesicouterine fold and the internal cervical orifice, in the middle of the segment and lower, sometimes even at the level of the internal cervical orifice after cesarean section in emergency in labor.
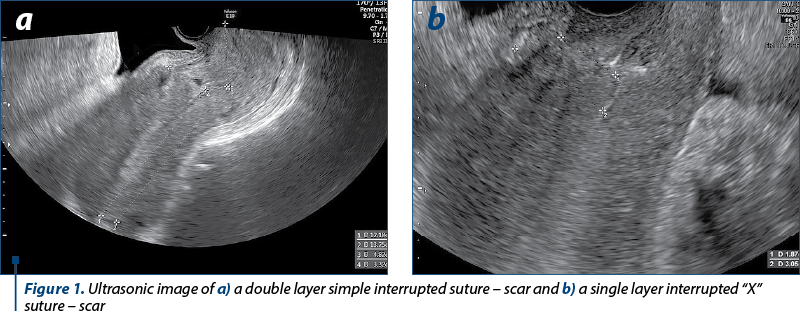
The evaluation of the uterine scar concerns the following parameters: (a) the number of scars on the anterior uterine wall (single or multiple; if multiple scars, they are evaluated separately, numbered in relation to proximity to the uterine fundus or internal cervical orifice); (b) the location of each uterine scar, defined by the height ratio H = a/b, where “a” is the distance from the top of the endometrial cavity to the scar, and “b” is the distance from the top of the endometrial cavity to the internal cervical orifice, a measurement that covers virtually the entire length of the endometrial cavity. The unit value of the ratio means a location of the scar at the level of the internal cervical orifice, while a subunit value of the ratio indicates the location of the scar above the level of the internal cervical orifice; (c) the healing defect defined by the deficiency ratio D = c/d, where “c” is the myometrial thickness at the uterine scar and “d” is the normal adjacent thickness of the myometrium measured as longitudinal section (Figure 1). In 2012, Naji et al. standardized the imaging techniques and ultrasound measurements of the uterine scar after caesarean section and proposed a three-dimensional measurement of the defect in both sagittal and transverse planes(25). The loss of over 50% of the myometrial thickness at the level of the scar classifies the defect in the severe category. A Danish study looked at 324 women and 471 scars, and reported a 4.4% percentage of body locations and an incidence of defects scarring of 19.4%, half of which were severe; the risk of vicious scars doubles in the case of uterine retroversion and with each new caesarean section, confirming that repeated tissue trauma and mechanical traction are factors which causes the disruption of the normal healing process by the progressive deficiency of vascular perfusion(26).
Depending on the cut-off used in defining the tranche defect (visible versus ≤1 mm), the prevalence of the niche reported in literature is extremely variable, ranging from 6.9% to 96.6%(27). The magnitude of the defect is significantly influenced by the type of myorrhaphy, the continuous interlocking suture being associated with a residual myometrial thickness significantly lower compared to the simple double-layer suture, but the prevalence defects, the dehiscence rate and the uterine rupture rate in the next pregnancy are similar for both types of suture(28). In terms of anatomical landmarks, low transverse incision near or affecting the internal cervical orifice has an increased predisposition to niche formation compared to the high seedbed incision(29).
Sutures
The commonly used suturing techniques of the uterine closure include: (a) double layer, where continuous interlocking is followed by an imbricating second layer; and (b) single layer, where both continuous interlocking and non-interlocking sutures are used. The differences between the two sutures have been compared in four studies(5,7,30,31), where participants were randomized to two of three of the following techniques: single- versus double-layer uterine closure, peritoneal closure versus non-closure, and liberal versus restrictive subsheath drainage(32). No major differences were observed between the groups when dealing with the short-term outcomes (morbidity from infection as primary outcome, surgery duration, pain, the need for blood, hospital readmission, breastfeeding and transfusion). Thus, the role of double-layer closure for reducing a subsequent uterine rupture, when compared with single-layer closure, remains controversial. There is no evidence that double-layer closure reduces the risk of uterine rupture as derived from these studies, in which women were not randomly allocated to single- or double-layer closure, so the definitive recommendations regarding subsequent uterine rupture risk are not possible in women who desire future pregnancies(7).
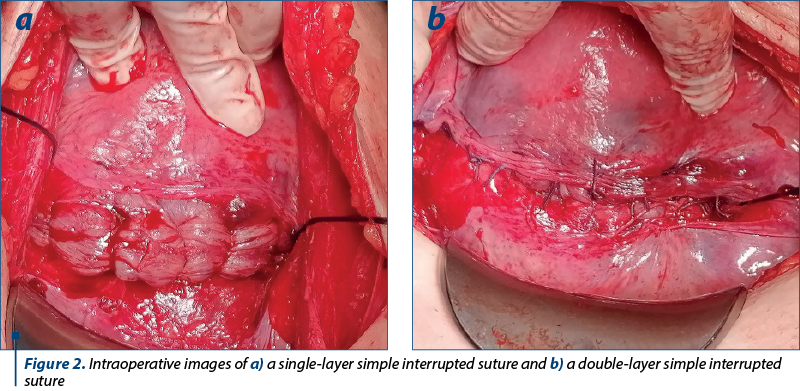
Other types of sutures that are used in caesarean section include interrupted sutures with simple thread, single or double layer, or “X”-thread (Figure 2). Some authors compared the continuous versus interrupted sutures(33). Their findings show that the advantages of continuous approach are the decreased blood loss and a shorter operating time. Using the swaged sutures they introduced less foreign material in the wound, which is an important advantage since the postpartum uterus involves quite rapidly. However, in term of sonographic-diagnosed hematomas and postoperative analgesic therapy, there were no differences between the two groups. The suitability of the suture for subsequent pregnancy was not discussed since previously uterine surgery was an exclusion criteria.
Discussion
Usually, single-layer closure is associated with high risks, although having its advantages, such as significant reductions in blood loss, operative time and postoperative pain, to name a few, but it carries more than twice the risk of uterine rupture compared with the double-layer closure. Several studies have produced higher rates of subsequent uterine rupture in women who had a single-layer uterine closure in previous caesarean(1-3). Thus, it is strongly recommended that the single-layer closure be avoided in women who desire a subsequent vaginal birth. However, the same studies have reported equivalent scar thickness irrespective of the method of closure and those locked and unlocked single-layer closures were associated with a higher uterine rupture risk than the double-layer closure, in women attempting a trial of labor. Babu and Magon(1) proposed a mechanism that can explain the inferior performance of the single-layer suture: they consider that the locked suture, although a strong hemostatic procedure, can cause a strangulation of the scar tissue. In turn, it could lead to a weaker healing of the tissue by inclusion of the decidua (endometrium) in the scar tissue. This argument is sustained by Poidevin(3) in several animal experiments, who demonstrated that suturing the complete thickness of the uterus allowed inclusions of endometrial tissue in the scar. Those inclusions produce scar defects in the subsequent weeks or months later. We can agree that a standardization of the suturing technique is imperative in order to ensure a correct approximation of all the layers and also restrict interoperator variability. This standardization will reduce all the risks associated with different suturing techniques and will minimize any thinning of lower segment caesarean section. Finally, in a quasirandomized study, Hayakawa et al.(4) found that a double-layer closure (which is defined as the continuous suture of the endometrium followed by a second continuous suture of the myometrium) was associated with fewer scar defects compared to the usual single-layer closure, a finding which cannot be ignored when we consider the woman’s reproductive desire. We also conclude that the correct uterine closure approach should be tailored to the patients’ needs(1-4).
Funding: Authors own resources.
Conflict of interests: The authors declare no conflict of interests.
Bibliografie
- Babu KM, Magon N. Uterine closure in Cesarean delivery: a new technique. N Am J Med Sci. 2012;4(8):358–61.
- Bujold E. The optimal uterine closure technique during cesarean. N Am J Med Sci. 2012;4(8):362–3.
- Poidevin LO (ed). Springfield, IL, Thomas CC. Caesarean section scars. 1965.
- Hayakawa H, Itakura A, Mitsui T, Okada M, Suzuki M, Tamakoshi K, et al. Methods for myometrium closure and other factors impacting effects on cesarean section scars of the uterine segment detected by the ultrasonography. Acta Obstet Gynecol Scand. 2006;85:429–34.
- CAESAR study collaborative group. Caesarean section surgical techniques: a randomised factorial trial (CAESAR). BJOG. 2010;117:1366-76.
- CORONIS collaborative. International study of caesarean section surgical techniques: a randomised factorial trial. Available at: www.npeu.ox.ac.uk/coronis.
- Dahlke JD, Mendez-Figueroa H, Rouse DJ, Berghella V, Baxter JK, Chauhan SP. Evidence-based surgery for cesarean delivery: an updated systematic review. Am J Obstet Gynecol. 2013;209(4):294-306.
- Bohîlţea R. Repere anatomice în operaţia cezariană. In: Operaţia cezariană. Ionescu C, Dimitriu M, eds. Carol Davila Publishing, 2018.
- Wylie BJ, Gilbert S, Landon MB, Spong CY, et al.; Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD) Maternal-Fetal Medicine Units Network (MFMU). Comparison of transverse and vertical skin incision for emergency cesarean delivery. Obstet Gynecol. 2010;115(6):1134.
- Holmgren G, Sjöholm L, Stark M. The Misgav Ladach method for cesarean section: method description. Acta Obstet Gynecol Scand. 1999;78(7):615-21.
- Dahlke JD, Mendez-Figueroa H, Rouse DJ, Berghella V, Baxter JK, Chauhan SP. Evidence-based surgery for cesarean delivery: an updated systematic review. Am J Obstet Gynecol. 2013;209(4):294-306.
- Todman D. A history of caesarean section: from ancient world to the modern era. Aust N Z J Obstet Gynaecol. 2007;47(5):357-61.
- Berghella V. Cesarean delivery: Technique. UpToDate. 2017. Available at: https://www.uptodate.com/contents/cesarean-delivery-surgical-technique
- Shipp TD, Zelop CM, Repke JT, Cohen A, Caughey AB, Lieberman E. Intrapartum uterine rupture and dehiscence in patients with prior lower uterine segment vertical and transverse incisions. Obstet Gynecol. 1999;94(5 Pt 1):735-40.
- Patterson LS, O’Connell CM, Baskett TF. Maternal and perinatal morbidity associated with classic and inverted T cesarean incisions. Obstet Gynecol. 2002;100(4):633-7.
- Naki MM, Api O, Celik H, Kars B, Yasar E, Unal O. Comparative study of Misgav-Ladach and Pfannenstiel-Kerr cesarean techniques: a randomized controlled trial. J Matern Fetal Neonatal Med. 2011;24:239-44.
- Gedikbasi A, Akyol A, Ulker V, et al. Cesarean techniques in cases with one previous cesarean delivery: comparison of modified Misgav-Ladach and Pfannenstiel-Kerr. Arch Gynecol Obstet. 2011;283:711-6.
- Belci D, Kos M, Zoricic D, et al. Comparative study of the “ Misgav-Ladach” and traditional Pfannenstiel surgical techniques for cesarean section. Minerva Ginecol. 2007;59:231-40.
- Xavier P, Ayres-De-Campos D, Reynolds A, Guimaraes M, Costa-Santos C, Patricio B. The modified Misgav-Ladach versus the Pfannenstiel-Kerr technique for cesarean section: a randomized trial. Acta Obstet Gynecol Scand. 2005;84:878-82.
- Sekhavat L, Dehghani Firouzabadi R, Mojiri P. Effect of expansion technique of uterine incision on maternal blood loss in cesarean section. Arch Gynecol Obstet. 2010;282(5):475-9.
- Walsh CA, Walsh SR. Extraabdominal vs. intraabdominal uterine repair at cesarean delivery: a metaanalysis. Am J Obstet Gynecol. 2009;200(6):625.e1-8.
- Regnard C, Nosbusch M, Fellemans C, Benali N, van Rysselberghe M, Barlow P, Rozenberg S. Cesarean section scar evaluation by saline contrast sonohysterography. Ultrasound Obstet Gynecol. 2004;23(3):289–92.
- Valenzano M, Lijoi D, Mistrangelo E, Costantini S, Ragni N. Vaginal ultrasonographic and hysterosonographic evaluation of the low transverse incision after caesarean section: correlation with gynaecological symptoms. Gynecol Obstet Invest. 2006;61(4):216–22.
- Bij de Vaate AJM, Brolmann HAM, Van der Voet LF, et al. Ultrasound evaluation of the Cesarean scar: relation between a niche and postmenstrual spotting. Ultrasound Obstet Gynecol. 2011;37(1):93–9.
- Naji O, Abdallah Y, Bij De Vaate AJ, Smith A, Pexsters A, Stalder C, McIndoe A, Ghaem-Maghami S, Lees C, Brolmann HA, Huirne JA, Timmerman D, Bourne T. Standardized approach for imaging and measuring Cesarean section scars using ultrasonography. Ultrasound Obstet Gynecol. 2012;39(3):252–9.
- Ofili-Yebovi D, Ben-Nagi J, Sawyer E. et al. Deficient lower-segment Cesarean section scars: prevalence and risk factors. Ultrasound Obstet Gynecol. 2008;31(1):72–7.
- Glavind J, Madsen L D, Uldbjerg N, Dueholm M. Ultrasound evaluation of Cesarean scar after single- and double-layer uterotomy closure: a cohort study. Ultrasound Obstet Gynecol. 2013;42(2):207–12.
- Sardo AS, Saccone G, McCurdy R, Bujold E, Bifulco G, Berghella V. Risk of Cesarean scar defect following single- vs. double-layer uterine closure: systematic review and meta-analysis of randomized controlled trials. Ultrasound Obstet Gynecol. 2017;50(5):557-58.
- Osser OV, Jokubkiene L, Valentin L. High prevalence of defects in Cesarean section scars at transvaginal ultrasound examination. Ultrasound Obstet Gynecol. 2009;34(1):90-7.
- Roberge S, Chaillet N, Boutin A, et al. Single- versus double-layer closure of the hysterotomy incision during cesarean delivery and risk of uterine rupture. Int J Gynaecol Obstet. 2011;115(1):5-10.
- Dodd JM, Anderson ER, Gates S. Surgical techniques for uterine incision and uterine closure at the time of caesarean section. Cochrane Database Syst Rev. 2014;(7):CD004732.
- Viney R, Isaacs C, Chelmow D. Intra-abdominal irrigation at cesarean delivery: a randomized controlled trial. Obstet Gynecol. 2012;119(6):1106-11.
- Hohlagschwandtner M, Chalubinski K, Nather A, Husslein P, Joura EA. Continuous vs. interrupted sutures for single-layer closure of uterine incision at cesarean section. Arch Gynecol Obstet. 2003;268(1):26–8.
Articole din ediţiile anterioare
Indicaţiile şi contraindicaţiile naşterii vaginale după operaţie cezariană
În ultimii ani, modalitatea de naștere este reprezentată de operația cezariană într-un procent foarte ridicat. Operația cezariană reprezintă aproap...
Rolul sarcinii şi al naşterii în apariţia tulburărilor de statică pelvică
Introducere. Multiple studii subliniază consecinţele naşterii vaginale asupra planşeului pelvic, însă sarcina în sine reprezintă un factor de risc ...
Postpartum hemorrhage – a major obstetrical emergency. Causes and treatment
Hemoragia post-partum (HPP) este o problemă semnificativă de sănătate maternă, reprezentând o cauză majoră de mortalitate obstetricală la nivel g...
Corticoterapia, beneficii şi riscuri − o revizuire a literaturii
De aproape trei decenii, administrarea corticosteroizilor înainte de naşterea prematură este una din cele mai importante terapii antenatale dispo...