The global coronavirus pandemic has a major impact on the healthcare services and professionals. It brings challenges to the gynecologists’ work in optimizing the care of their patients. In an effort to restrain the transmission of the virus and prioritize the treatment of patients with COVID-19, the elective surgeries were limited during the pandemic. Nevertheless, the urgent procedures must be performed. In this paper, we reviewed the articles regarding the advantages and risks of minimally invasive surgery and the methods to perform a safe surgery during the COVID-19 pandemic. At this time, there is limited evidence that laparoscopy represents a high risk of infection, because there is limited data on the presence of the virus in the surgical smoke. However, it is thought that the best option for all the surgeons would be to use certain strategies to minimize any theoretical risk of viral transmission during laparoscopic surgery. Recommendations and guidelines have been made by authorities, by the Ministry of Health from Romania and by professional societies on how to operate under extreme circumstances within a system where the priority is, first and foremost, the patients who need immediate care under safe circumstances. The laparoscopy advantages regarding the reduced hospitalization time, the smoke and fluids that can be restrained and evacuated in a safer way and the less traumatic surgical maneuvers are very helpful during this pandemic. Recommendations were made regarding the protection during emergency surgery in COVID-19 patients that specifically include the use of N95 masks for anesthesia and surgical teams. The patient should also wear a fluid-resistant surgical face mask. A checklist that can be considered both a new standard for hospitals and a tool that helps healthcare personnel and patients to feel safe during their hospital stay was developed in order to decrease the risk of viral spread.
Chirurgia minim invazivă în timpul pandemiei de COVID-19. Rolul chirurgiei laparoscopice în endometrioză şi oncologie
Minimally invasive surgery during the COVID-19 pandemic. The approach to laparoscopic surgery in endometriosis and oncology
First published: 23 octombrie 2020
Editorial Group: MEDICHUB MEDIA
DOI: 10.26416/ObsGin.68.3.2020.4008
Abstract
Rezumat
Pandemia creată de noul tip de coronavirus are un impact major asupra serviciilor de sănătate publică şi asupra profesioniştilor din acest domeniu. Pandemia aduce noi provocări ginecologilor care lucrează pentru a optimiza îngrijirea acordată pacienţilor lor. În încercarea de a minimiza riscul transmiterii virusului şi pentru a prioritiza tratarea pacienţilor infectaţi cu SARS-CoV-2, intervenţiile elective au fost limitate în timpul pandemiei. Totuşi, intervenţiile care apar de urgenţă trebuie efectuate în continuare. În cadrul acestei lucrări, vom prezenta avantajele şi riscurile chirurgiei minim invazive efectuate în timpul pandemiei de COVID-19, dar şi cum se poate efectua o intervenţie minim invazivă în condiţii de siguranţă. Literatura de specialitate existentă până la ora actuală dispune de date limitate în ceea ce priveşte existenţa virusului în fumul emis în cadrul intervenţiilor minim invazive. Însă se admite că luarea unor măsuri intraoperatorii pentru a limita o teoretică transmitere virală este cea mai bună strategie. Au fost emise recomandări şi ghiduri de către autorităţi, Ministerul Sănătăţii şi de societăţile de obstetrică-ginecologie, care au cuprins metode de efectuare a intervenţiilor la pacienţii care aveau nevoie de îngrijiri de sănătate imediate. Avantajele general valabile ale chirurgiei laparoscopice se menţin şi în contextul pandemiei de COVID-19, iar timpul redus de spitalizare, faptul că fumul şi fluidele sunt reţinute într-un singur loc şi că manevrele chirurgicale sunt mai puţin traumatice sunt de mare ajutor în această perioadă. În ceea ce priveşte protecţia personalului medical, se recomandă, în cadrul intervenţiilor de urgenţă, purtarea de măşti N95 pentru anestezie şi de către echipa chirurgicală. Pacienţii ar trebui să poarte, de asemenea, o mască rezistentă la fluide. A fost creată o listă de reglementări ce poate fi considerată ca un nou standard pentru spitale, dar şi un mijloc prin care personalul medical şi pacienţii să se simtă mai în siguranţă în perioada petrecută în spital.
Introduction
The current coronavirus pandemic raised a lot of questions and challenges among the gynecologists from all over the world. The healthcare services redirected their priorities to take care for patients infected by the new type of coronavirus(1). The increased number of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infected patients led to the reorganization of the resources and operating rooms and of intensive care beds in order to be used for these cases. This caused elective surgical procedures to be limited, but the urgent procedures cannot be limited(2).
Recommendations and guidelines were made by authorities and professional societies on how to operate under extreme circumstances within a system where priority is given to patients who need immediate care(3). The Royal College of Surgeons recommends “to consider laparoscopy only in selected individual case”, and the Society of American Gastrointestinal and Endoscopic Surgeons recommends the use of filters to release the CO2(4,5).
A list from the American College of Surgeons has been made in order to classify the gynecological interventions according to severity(6).
Emergency surgeries:
-
Ectopic pregnancy
-
Spontaneous abortion
-
Adnexal torsion
-
Ruptured tubal-ovarian abscess
-
Tubal-ovarian abscess not responding to conservative therapy
-
Acute and severe vaginal bleeding
-
Emergency cerclage of the cervix based on pelvic exam/ultrasound findings.
-
Surgeries that if significantly delayed could cause significant harm:
-
Cancer or suspected cancer
-
Gestational trophoblastic neoplasia
-
Cerclage of the cervix to prevent premature delivery based on history
-
Pregnancy termination (for medical indication or at patient’s request).
Because some surgeries had to be done, a concern with the use of minimally invasive techniques has been raised, due to the potential risk of viral transmission of SARS-CoV-2 in the context of pneumoperitoneum creation(7).
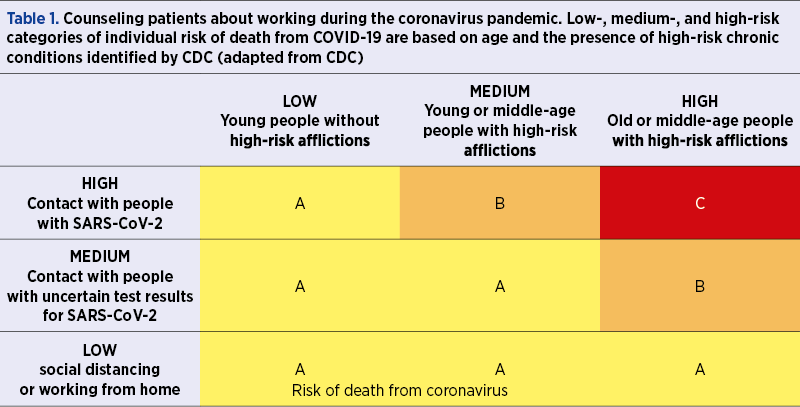
Studies have shown that people with chronic conditions (diabetes, hypertension, obesity) and older people in general are more susceptible to die from COVID-19. An epidemiological study carried out in China shows that the fatality rate is less than 0.5% among people under 50 years of age, 1.3% among those aged 50 to 59 years old, and 3.6% among those aged 60 to 69 years old(8).
There are not enough data for estimating the occupational risk for COVID-19, although the Center for Disease Control and Prevention (CDC) states that healthcare workers represent at least 11% of the reported SARS-CoV-2 infections(9). One hospital in Spain has reported that 11.6% of its 6800 employees tested positive for SARS-CoV-2(10).
Having all this information, the question we address is whether people at high risk for death from COVID-19 should stop working in order to diminish the risk of infection and death.
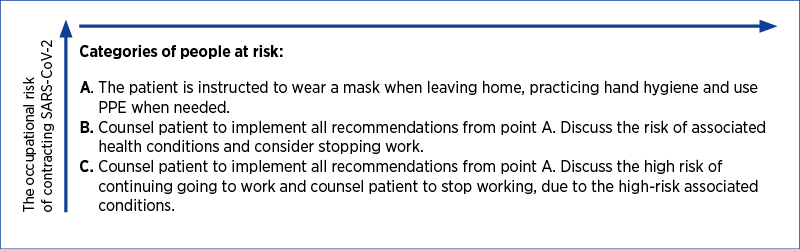
We will further present a diagram that correlates the occupational risk of contracting SARS-CoV-2 and the risk of death if they are infected. It is important to identify the low-, medium-, and high-risk categories of workers and to implement a counseling program for patients about working during this pandemic(11).
Risk of SARS-CoV-2 transmission during surgery
Laparoscopy is an aerosol-generating procedure and this fact raised some concerns on the safety of the surgical team during the intervention. SARS-CoV-2 is an RNA respiratory virus which is primarily identified in the human upper and lower respiratory tract and has a size range of 0.06 to 0.14 microns. Beside respiratory tract, the virus has been found in the entire gastrointestinal tract(12). The virus may also be aerosolized and transmitted in smaller droplets in gas suspension. Despite the fact that the RNA can be detected in the blood, there is no evidence of transmission that way(13).
Laparoscopy surgery has an essential component – pneumoperitoneum – that raises the risk of aerosol exposure to the surgical team. Aerosol exposure is more likely to occur during the release of CO2 at the beginning and at the end of procedure, with the insertion and removal of ports and instruments(5). There are studies that show that there is a risk of transmission of infections with hepatitis B virus (HBV), human immunodeficiency virus (HIV) and human papillomavirus (HPV) from surgical smoke(1).
However, since the only demonstrated form of transmission of SARS-CoV-2 is through respiratory droplets, the risk of transmission from the abdomen is unclear, as there are no data on the presence of SARS-CoV-2 in the surgical smoke(2).
The advantages of minimally invasive surgery
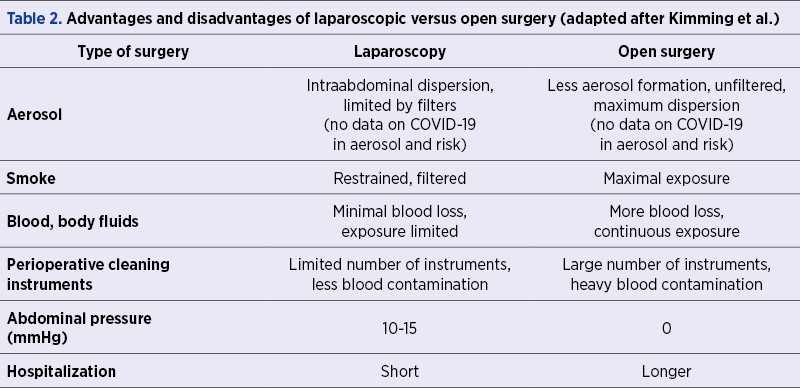
In the limited climate of COVID-19, we must review the benefits of the laparoscopic surgery. In the pandemic situation, the laparoscopic approach can reduce the length of hospitalization due to faster recovery, therefore increasing the availability of beds. In case of a positive SARS-CoV-2 patient, the laparoscopic surgery has less traumatic maneuvers compared to open surgery. An advantage over open surgery is that the smoke and fluids are collected in a restrained space, and as long as the smoke and fluids are evacuated in a safe way, the spread to the surgical team is minimal(1,7). In Table 2 there are presented the advantages and disadvantages of laparoscopic versus open surgery.
Thus, laparoscopy might offer a protection against direct viral exposure through blood and smoke by using filters and evacuating the smoke in a proper way.
Smoke evacuation
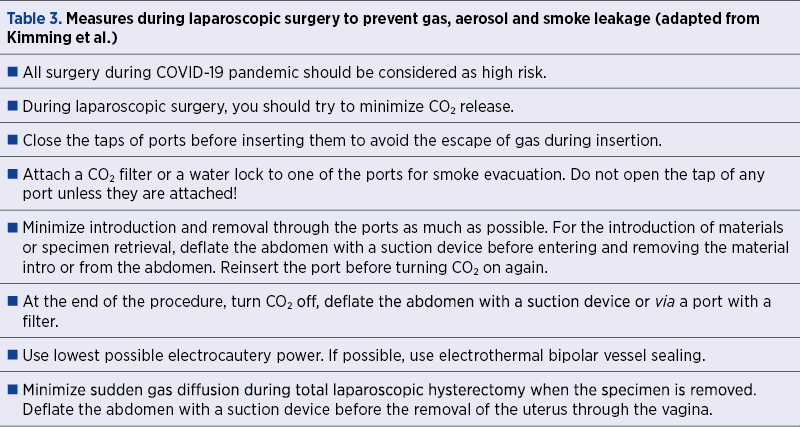
There are some techniques that can be used in order to lower the risk of airborne particle dispersion at the time of laparoscopic surgery, and especially during smoke and pneumoperitoneum evacuation. The traditional laparoscopic ways of insufflation, exsufflation and releasing the smoke to clear the field can have a risk of infection. Therefore, some new recommendations are necessary – in Table 3, there are presented the measures to reduce gas dispersion and smoke leaking(3,7).
In times when economy is not doing well and the availability of consumables and protection equipment is limited, Yoav Mintz et al. proposed a simple, very low-cost filtration system made of components that are found in an operating theater. They used standard electrostatic filters from ventilation machines that are connected to the trocar via a standard tubing and an endotracheal tube connector. This filter can be used for evacuating and filtering the generated smoke, as well as the potential viral load, and ensures the safety of the surgical team(14).
Protection of medical personnel
Surgical teams are at high risk for SARS-CoV-2 exposure, as the virus survives for days on multiple operating room surfaces, plastic and stainless steel. The personal protective equipment (PPE) is the most important topic of discussion for front-line healthcare staff. There are two main issues: shortages of equipment and inappropriate use of equipment(15).
The Stanford guideline states that any patient could be infected with SARS-CoV-2 unless proven otherwise by a negative RT-PCR test.
-
When operating on SARS-CoV-2 positive patients, the guideline recommends that the surgeons, anesthesiologists and operating room staff wear standard surgical personal protective equipment (PPE), that includes a face shield, mask, waterproof gown, double gloves, and shoe covers.
-
When an RT-PCR test is negative for SARS-CoV-2, the surgical team members can wear standard surgical clothing and a simple surgical mask.
Anesthesiologists should wear N95 face masks and droplet-protective PPE because they are positioned at the head of the operating table throughout the procedure. The cleaning staff should take precautions regarding droplets when cleaning any operating room(16).
There are multiple options available to choose from when using a protective mask, depending on the SARS-CoV-2 PCR test result: standard surgical mask, or N95 respiratory mask. There are no strict rules or data to suggest that N95 are better for protecting against SARS-CoV-2(17). A standard surgical mask blocks gross inhalation of droplets, while a well-fitted N95 respiratory mask is capable of filtering aerosols up to dimensions of 0.3 microns.
A recent guideline from the Chinese Journal of Surgery presented recommendations for emergency surgery in COVID-19 patients that specifically include the use of N95 masks for anesthesia and surgical teams. Eyewear can be added based on a risk assessment. The patient should also wear a fluid-resistant surgical face mask(18).
World Health Organization recommends that airborne precautions consist of: fit-tested and fit-checked high filtration mask, goggles or visor, long sleeved fluid-repellent gown and gloves. The personal protective equipment should be simple to remove after use, without contaminating the user, because the risk of contamination is the highest after removal(17).

Resuming laparoscopic surgery during and post-COVID-19 pandemic
New concerns regarding patient’s safety are emerging as hospitals are preparing for the resumption of elective surgery.
The American College of Surgeons (ACS) puts emphasis on building patient’s trust regarding the healthcare facility’s readiness for safely performing surgery during and post-COVID-19 pandemic. Thus, ACS has developed a comprehensive checklist with all the additional strategies implemented in the healthcare facility in order to diminish the epidemiological risk of viral spread(19). This checklist can be defined both as a new standard for all the healthcare facilities and also as a tool to help surgeons provide all the information needed to the patients in order to feel safe during their admission in the hospital.
It is suggested that surgeons should first verify which of the checklist items are present in their healthcare facility, and ACS also emphasizes the fact that the checklist can be adjusted according to the particularities of a certain hospital (some items might be developed, other missing items might not be considered necessary). Also, it is suggested that surgeons should inform the patients regarding certain checklist items (e.g., resources, protocols, policies). This can be done by any means (e-mail, personal letter or other).
The checklist suggested by the American College of Surgeons is organized in two parts: part one – core facility checklist items; and part two – surgery-specific items.
Part one consists of important aspects that provide the general safety of the patients during their stay in the hospital.
Patient-related COVID-19 policies for the facility bring the following key points:
1. Screening and testing for patients entering the facility – screening policy for all the people entering a facility, and protocols for patients who screen positive.
2. Mitigation with masks – patient/visitor mask policy in place and supply on hand for patients without one.
3. COVID-19 informed patient program – its purpose is to educate the patients about the conduct they should adopt while staying in the hospital in order to avoid any complications in the post-pandemic environment(20).
Healthcare workers and PPE policies for the facility consist of protocols for healthcare workers to keep patients safe, protocols for the safe protection of medical front-line teams from the emergency department, and policies in place for healthcare workers which include the level of PPE required.
Facility infection control and pandemic COVID-19 policies emphasize the need of the following strategies: universal precautions protocols, patient isolation and physical distancing, hand washing protocol, facility cleaning, equipment sterilization, and air circulation/filtration processes.
COVID-19 rate tracking is also important: the rates of SARS-CoV-2 infections in local hospital should be closely monitored; the number of new cases and COVID-related deaths; patients’ outcomes with morbidity and mortality tracking for COVID-19 related events(6).
Publicly available hospital information and data become mandatory in order for the patients to gain more knowledge regarding all the new measurements taken in the healthcare facility for their safety. For example, sharing information on a hospital website would serve to inform patients of local hospital COVID-19 related policies, and also individual discussions between each patient and their surgeon would ensure that they are informed about all the new protective strategies that are being taken. The American College of Surgeons acknowledges that this discussion is one of the most effective ways to restore patient trust by facilities and surgeons resuming surgery(19).
Publicly available hospital information should present in a comprehensive way the following items: the existence of a multidisciplinary team to review COVID-19 metrics and update COVID-19 daily progress as this impacts the readiness status, visitor policy, patient mask policy within the facility, cleaning policies, entrance screening processes, cleaning policies of key facility areas, including patient rooms, physical distancing, waiting room policy, the use of telehealth options (when existing), staff testing policy, scripted staff introduction and badging policy for patients to know who are the individuals behind masks, gowns, gloves etc., and what role the person plays on the team, policy for patient-centered verbal query on daily basis to access patient experience regarding COVID-19 safety concerns, food preparation and service policy, family update policy, elevator policy, and separate staff policy for treating non-COVID-19 patients(19).
It is suggested that a video tour of the hospital experience should be made, from entering the hospital to the entire process of surgical care in order to demonstrate visually for the patient what to expect, how people will look like, how they will be communicated with, and how to raise concerns and when to ask for clarifications(19).
The second part of the checklist consists of surgery-specific items: preoperative processes for SARS-CoV-2 testing or screening (or both) for surgical patients, protocol/policy for consent with COVID-19 related information and discussion of triage criteria and condition-specific priorities to have surgery if the treatment is at risk due to prolonged delay(21), protocols for patient readiness for surgery with specific screening questions identified for readiness evaluation (e.g., consider isolation for 1-2 weeks prior to operation, protocol/policy for patient PPE [e.g., mask] during inpatient stay(19), cleaning processes within key areas for the surgical patient – operating room, intensive care units, emergency rooms, hospital rooms, imaging centers, anesthesia services, waiting rooms), cleaning processes for equipment related to surgery, including anesthesia(21,22).
Publicly available surgery-related information and data should be available for the following items:
-
Preoperative testing/screening processes for surgical patients.
-
Surgery/operating room staff testing/screening.
-
Policy/recommendation for patient isolation prior to operation.
-
Patient mask policy during the day of operation, and postoperatively.
-
Cleaning policies.
-
Surgery consent policy with informed risks related to COVID-19.
-
Advance directive before surgery discussions.
-
Options for telehealth options.
-
Post-acute care discussions related to surgery.
-
Enhanced recovery protocols in place to optimize postoperative care and outcomes(19).
Conclusions
There are many questions and unknowns regarding the SARS-CoV-2 transmission during gynecological laparoscopic surgery. Because of this, the appropriate precautions must be taken to ensure the protection of medical personnel. The risk of airborne SARS-CoV-2 transmission from the abdominal cavity in a laparoscopic surgery is not known, at this time. However, it is thought that the best option for all the surgeons would be to use certain strategies to minimize any theoretical risk of viral transmission during laparoscopic surgery.
Laparoscopy remains the preferred surgical approach for gynecological patients during COVID-19 pandemic for most surgical indications.
Bibliografie
-
1. Ertan S, Grigoris G. COVID-19 pandemic and gynaecological endoscopic surgery. Facts Views Vis Obgyn. 2020 Mar;12(1):1.
-
2. Morris SN, Fader AN, Milad MP, Dionisi HJ. Understanding the “scope” of the problem: why laparoscopy is considered safe during the COVID-19 pandemic. J Minim Invasive Gynecol. 2020 May-June;27(4):789-791.
-
3. Kimmig R, Verheijen RHM, Rudnicki M. Robot assisted surgery during the COVID-19 pandemic, especially for gynecological cancer: a statement of the Society of European Robotic Gynaecological Surgery (SERGS). J Gynecol Oncol. 2020 May;31(3):e59.
-
4. Equipment PP. Joint RCOG/BSGE Statement on gynaecological laparoscopic procedures and COVID-19. Royal College of Obstetricians and Gynecologists. 2020.05.21.
-
5. Board EE. Equipment PP. ESGE Recommendations on Gynaecological Laparoscopic Surgery during COVID-19 Outbreak.
-
6. Joint statement on minimally invasive gynecologic surgery during the COVID-19 pandemic. J Minim Invasive Gynecol. 2020 July-August;27(5): 1027–1029.
-
7. Vigneswaran Y, Prachand VN, Posner MC, Matthews JB, Hussain M. What Is the Appropriate Use of Laparoscopy over Open Procedures in the Current COVID-19 Climate? J Gastrointest Surg. 2020 Apr 13;1–6.
-
8. Team TNCPERE. The epidemiological characteristics of an outbreak of 2019 novel coronavirus diseases (COVID-19) in China. Zhonghua Liu Xing Bing Xue Za Zhi. 2020 Feb 10;41(2):145-151.
-
9. Team CC-19 R. Characteristics of health care personnel with COVID-19 – United States, February 12 – April 9. MMWR Morb Mortal Wkly Rep. 2020;69:477:81.
-
10. Folgueira MD, Munoz-Ruiperez C, Alonso-Lopez MA, Delgado R. SARS-CoV-2 infection in Health Care Workers in a large public hospital in Madrid, Spain, during March 2020. medRxiv [Internet]. 2020 Jan 1;2020. Available at: http://medrxiv.org/content/early/2020/04/27/2020.04.07.20055723.abstract
-
11. Larochelle MR. “Is It Safe for Me to Go to Work?” Risk Stratification for Workers during the Covid-19 Pandemic. N Engl J Med. 2020 Jul 30;383(5):e28.
-
12. Zhu N, Zhang DW, W, Li X, Yang B, Song J, Zhao X, Huang B, Shi W, Lu R, Niu P, Zhan F, Ma X WD, Xu W, Wu G, Gao GF TW; China Novel Coronavirus Investigating and Research Team. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N Engl J Med. 2020;(382(8)):727–33.
-
13. Centers for Disease Control and Prevention. Healthcare professionals. Available at: https://www.cdc.gov/coronavirus/2019-ncov/hcp/index.html
-
14. Mintz Y, Arezzo A, Boni L, Chand M, Brodie R, Fingerhut A. A Low Cost, Safe and Effective Method for Smoke Evacuation in Laparoscopic Surgery for Suspected Coronavirus Patients. Ann Surg. 2020 Jul;272(1):e7-e8.
-
15. van Doremalen N, Bushmaker T, Morris DH, et al. Aerosol and surface stability of SARS- CoV-2 as compared with SARS-CoV-1. New Engl J Med. 2020 Apr 16;382(16):1564-1567.
-
16. Forrester JD, Nassar AK, Maggio PM, Hawn MT. Precautions for Operating Room Team Members during the COVID-19 Pandemic. J Am Coll Surg. 2020 Jun;230(6):1098-1101.
-
17. WHO. Rational use of personal protective equipment for coronavirus disease (COVID-19) and considerations during severe shortages. 2020 April; 1–28.
-
18. Tao KX, Zhang B, Zhang P, et al. Recommendations for general surgery clinical practice in novel coronavirus pneumonia situation. Zhonghua Wai Ke Za Zhi. 2020 Feb 14;58(0):E001.
-
19. American College of Surgeons. Post-COVID-19 Readiness Checklist for Resuming Surgery. 2020. Available at: https://www.facs.org/covid-19/checklist
-
20. Chiofalo B. Practical recommendations for gynecologic surgery during the COVID-19 pandemic. Int J Gynaecol Obs. 2020;150.10.1002/ijgo.13248.
-
21. Liang ZC, et al. COVID-19 and Elective Surgery: 7 Practical Tips for a Safe, Successful and Sustainable Reboot. Ann Surg. 2020 May 20;10.1097/SLA.0000000000004091.
-
22. Al-Balas M, Al-Balas HI, Al-Balas H. Surgery during the COVID-19 pandemic: A comprehensive overview and perioperative care. Am J Surg. 2020 Jun; 219(6):903–906.
Articole din ediţiile anterioare
Managementul infecţiei cu SARS-CoV-2 în cazul pacientelor gravide. Cunoştinţele actuale privind COVID-19 în sarcină
SARS-CoV-2 – un nou tip de betacoronavirus ARN – infectează celulele epiteliale de la nivelul căilor respiratorii. Pacienţii cu COVID-19 manifestă ...
Infecţiile asociate plăgilor operatorii în pandemia de COVID-19: un studiu comparativ
Pandemia de COVID-19 a impus noi abordări, cu singurul scop de a prioritiza resursele în oferirea, în continuare, de servicii medicale calitative.
Coagulopatia asociată COVID-19 şi anticoagulantele
Pacientele infectate cu SARS-CoV-2 prezintă un status protrombotic. Incidenţa complicaţiilor tromboembolice la pacientele cu boală severă este mult...