Introduction. Given how common caesarean section (C-section) has become, our objectives are: 1) to analyze the way Romanian women want to give birth, and 2) to draw a profile of patients and doctors in whose case the actual birth method has changed from the preferred method after admission in the labor ward. Materials and method. We conducted a statistical analysis based on an observational, analytical and cross-sectional survey in a tertiary level maternity from Romania. Results. We calculated an increase of almost 58% in the actual childbirth mode against preferred childbirth by caesarean section, rather difficult to justify based only on medical emergencies. 31.8% preferred natural birth, and 68.2% preferred C-section. The profiles of patients with concordant and nonconcordant delivery modes are different and indicate a statistically significant difference between the preference for delivery and the actual birth method. Doctors’ profiles show that specialists and consultants attend the largest share of nonconcordant births, while residents and young senior doctors attend mostly vaginal births. Conclusions. We emphasize health system particularities in Romania as triggers of high C-section rates that favor women’s preferences against C-section medical indication. Improving patients’ confidence in the healthcare system, built on competence and fitted hierarchical team position, may lead to choosing the optimal way of birth for childbirth safety and pain control.
Cine stabileşte indicaţia operaţiei cezariene? Studiu transversal într-o maternitate de nivel III, despre profilul doctorilor şi al pacientelor la naştere
Who indicates caesarean section? A cross-sectional survey in a tertiary level maternity on patients and doctors’ profiles at childbirth
First published: 25 aprilie 2021
Editorial Group: MEDICHUB MEDIA
DOI: 10.26416/ObsGin.69.2.2021.4977
Abstract
Rezumat
Introducere. Având în vedere cât de frecventă este acum operaţia cezariană, obiectivele noastre sunt: 1) să analizăm felul în care româncele doresc să nască şi 2) să trasăm un profil al pacientelor şi medicilor în cazul cărora calea naşterii s-a schimbat după internarea în sala de naştere faţă de indicaţia stabilită anterior. Materiale şi metodă. S-a efectuat o analiză statistică, bazată pe un sondaj observaţional, analitic şi transversal, într-o maternitate de nivel terţiar din România. Rezultate. S-a calculat o creştere de aproape 58% a ratei cezarienelor, destul de dificil de justificat doar pe baza urgenţelor medicale. 31,8% au preferat naşterea naturală şi 68,2% au preferat operaţia cezariană. Profilurile pacientelor cu moduri de naştere concordante şi neconcordante sunt diferite şi indică o diferenţă semnificativă statistic între preferinţa de naştere şi metoda reală de naştere. Profilurile medicilor arată că specialiştii şi consultanţii participă la cea mai mare parte a naşterilor neconcordante, în timp ce rezidenţii şi tinerii medici seniori participă în principal la naşteri vaginale. Concluzii. Subliniem particularităţile sistemului de sănătate din România ca factori declanşatori ai unor rate ridicate ale operaţiei cezariene, care favorizează preferinţele femeilor faţă de indicaţiile medicale ale acestei proceduri. Îmbunătăţirea încrederii pacientelor în sistemul sanitar, bazată pe competenţele şi poziţia ierarhică adecvată a echipei, poate duce la alegerea modului optim de naştere, în siguranţă şi controlând durerea.
Introduction
Evidence from database registries shows a considerable increase in birth rates by caesarean section (C-section), especially in urban areas of middle- and high-income countries, reaching a rate of up to 50% of deliveries in several countries(1-3). Former European communist states have higher C-section rates when compared with Western European countries. In 2018, Romania had a 44.50% rate, Bulgaria – 44.58%, Poland – 38.92%, and Hungary had a 38.03% rate(4). Data between 2009 and 2017 reveal a decline by 65% of infant mortality, but with an increased by 44.11% of C-sections in Romania(5,6).
Although World Health Organization does not any longer recommend an ideal rate for C-sections, the range of 10-15% at the population level is used pragmatically for international monitoring, aiming at ensuring maternal and perinatal health benefits and reduce potential harms(2,7). Given how common C-section has become, it could be of much importance to understand this phenomenon in countries with high C-section rates.
Betrán et al. identify two categories of interventions to reduce unnecessary C-sections: clinical (obstetrical) interventions and nonclinical interventions, that could overlap each other(7). Nonclinical interventions target the psychosocial level of women and childbirth education, but also guidelines for healthcare professionals and second opinion on C-sections(8).
Objectives
The objectives of this study are: 1) to analyze the way Romanian women want to give birth, and 2) to draw a profile of patients and doctors in whose case the actual birth method is different from the preferred method after admission in the labor ward. Both objectives are important for understanding the patients’ preference for birth delivery methods, and for capturing patients and doctors’ characteristics that are connected to these methods. Moreover, this helps in a better apprehension of the motives behind changes in patients’ preference regarding the way of giving birth and of the high rate of C-sections in Romania, but also in similar countries.
Materials and method
We conducted an observational, analytical and cross-sectional non-anonymous survey based on hospital database registries and on a questionnaire distributed at a tertiary level maternity hospital in Bucharest, Romania, in February 2014, within a research project (additional file: distributed questionnaire). The questionnaire was discussed with doctors from the maternity and further validated. The final number of respondents (117) offers a level of confidence of 95% and an error margin of 9% when benchmarked against all births in Romania in 2014, and it is due to available data from the project.
The questionnaire was distributed to all full-term pregnant women when admitted in the hospital for giving birth, and when discharged at home from hospital during February 2014. The inclusion criteria were: more than 36 weeks of gestational age, singleton pregnancy, expecting a child without assessed congenital anomalies, and understanding written Romanian. The participation was voluntary, and the study was approved by the hospital’s Commission of Ethics. A 1-10 scale was used to assess birth experience and pain during labor, and doctors’ (obstetrician and anesthetist) and midwives’ performance (1 – Worst; 10 – Best). Patients’ assessments were transformed into the following categories: Very good – 9 to 10; Good – 7 to 8; Satisfactory – 5 to 6; Not satisfactory – 1 to 4.
We conducted a statistical analysis using the Statistica software. Firstly, we performed descriptive statistics of the responses in the form of frequencies (absolute and relative) and means and standard deviations, depending on the type of variables (qualitative versus quantitative). We compared the preferred and actual modes of delivery using the Chi-square and V-square tests, and we applied the t-test for independent samples differences in mean scores. We also used McNemar non-parametric significance tests for two dependent samples for the analysis of the matched samples presenting the choice of pregnant women before delivery and the actual method of birth (the after-effect). P-values of less than 0.05 (p<0.05) indicate the statistical significance.
Results
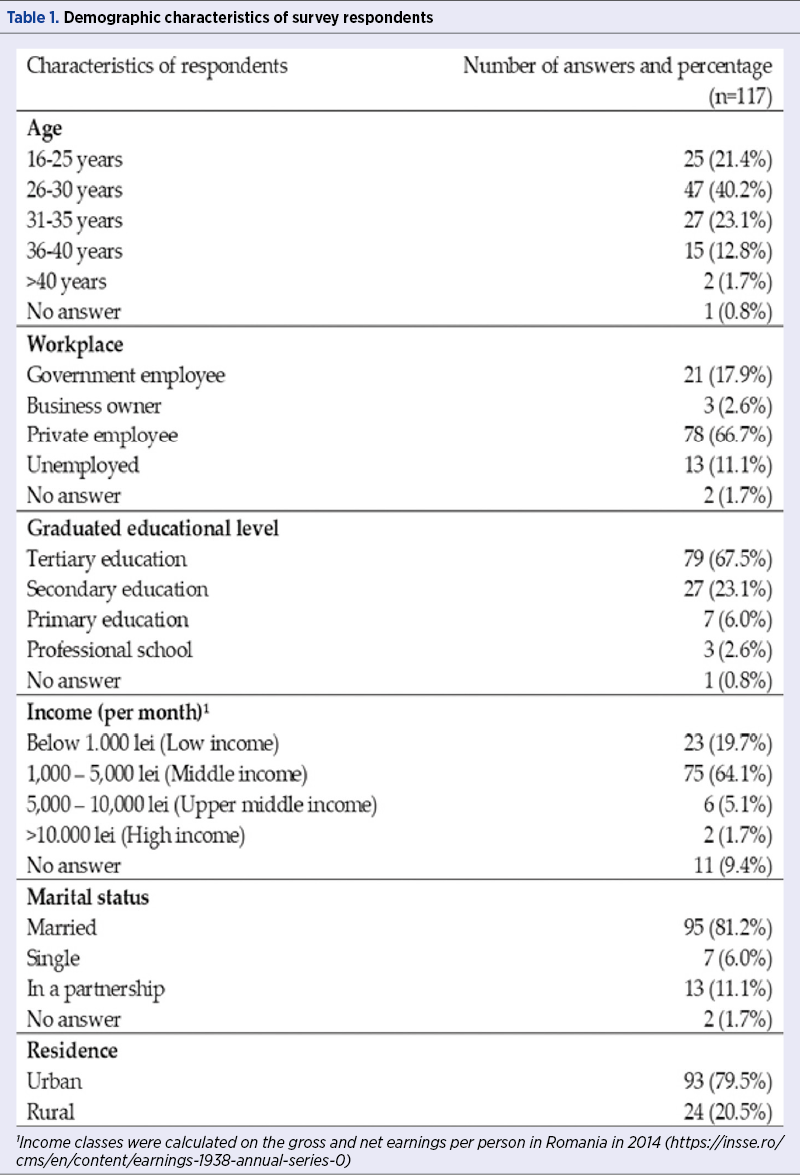
There were 168 deliveries in the hospital in February 2014, of which 51 spontaneously, 10 instrumental vaginal deliveries (forceps in eight cases and vacuum in two cases), and 107 through C-section. The final number of women who consented to participate in our survey was 117 (69.64%). Their demographic characteristics are presented in Table 1.
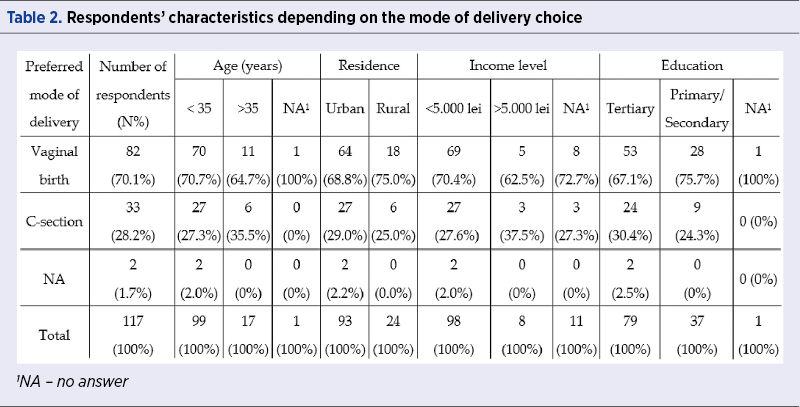
On the day of labor ward admission, according to the birth plan established in the third trimester with the doctor, 70.1% (n=82) of women preferred vaginal birth, 28.2% (n=33) preferred C-section and two women (1.7%) did not respond. Younger and more educated women, mostly living in urban areas and the low-to-middle income categories, showed a higher preference for a vaginal birth (Table 2).
Out of the 117 respondents, 55.6% (n=65) had vaginal births and 44.4% (n=52) had C-sections (Table 3 ). For 19 patients, the preferred and actual ways of delivery were different. None of the women who chose C-section had undergone vaginal birth.
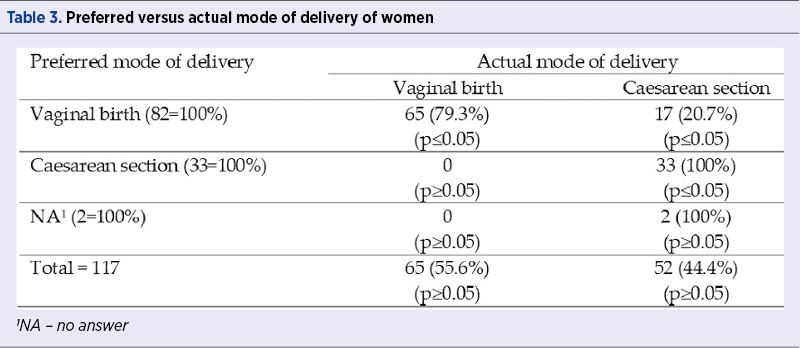
All women who preferred C-section and declared an indication for C-section gave birth this way. C-section on request was preferred by 6.8% (n=8) of women. They were aged below 35 years old, were higher education graduates, six out of eight had middle to high income and lived in urban areas. For all eight women, C-section indications were not concordant when patients’ and doctors’ indications in medical records were compared.
Scarred uterus is the most frequent indication for C-section (30.76% of C-sections) and all breech presentations were delivered by C-section, although some patients would have preferred a natural birth. Besides these indications, there were 22 primiparas with nonconcordant C-section indications between preferred and actual mode of birth; seven of them (31.8%) preferred natural birth and 15 (68. 2%) preferred C-section. The most frequent nonconcordant C-section indications were placenta praevia, oligohydramnios <39 weeks, and failed induction of labor.
Almost half of women who preferred vaginal birth (49; 59.8%) and 48.5% of the women who preferred C-section chose epidural anesthesia. Most women who preferred vaginal birth also preferred epidural anesthesia (59.5%; n=49); 38 of them (77.6%) had vaginal birth, while 11 (22.4%) had C-section. Eighteen out of 33 women (54.5%) which preferred C-section were primipara, and all of them gave birth by C-section.
Time spent in the labor ward, birth pain perception and professional doctors’ degree are presented from women’s perspective of preferred versus actual type of birth (Table 4). The patients with concordant vaginal births were younger, in the middle-to-low income category, less educated, but have undergone all recommended screening during their pregnancies. They were attended mostly by consultants and preferred epidural anesthesia. They assessed birth experience as good to very good, and birth pain as good. Patients with concordant C-section were in an elder group, with middle income mostly, and educated. They were attended mostly by consultants and specialists, and had the lowest preference for epidural anesthesia. They assessed highly their birth, but the rate birth pain was assessed only as satisfactory. The patients with nonconcordant modes of delivery were mature women (mostly aged between 26 and 35 years old), in the middle-to-high income category, and more educated. They mostly preferred epidural anesthesia, they assessed their birth as good to very good, and their birth pain as good.
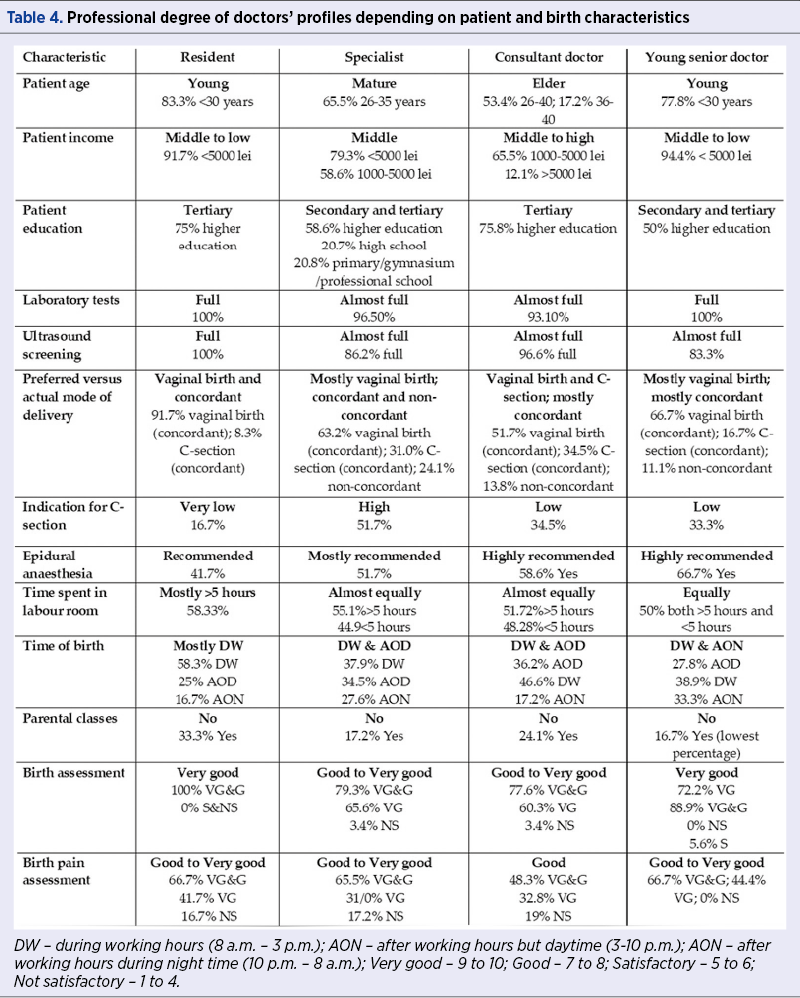
Resident and young senior doctors attended younger patients, in the middle-to-low income category, which have undergone full sets of laboratory tests during pregnancy. Specialists and consultant doctors attended more mature women, in the middle-to-high income category, mostly with higher education and full prenatal test screenings. They attended the largest share of nonconcordant births.
Fifty-two women (44.4%) gave birth during working hours (DW; 8 a.m. – 3 p.m.), 39 births (33.3%) occurred during the evening shift (AOD; 3 to 10 p.m.) and 26 births (22.2%) during the night shift (AON; 10 p.m. to 8 a.m.). There were more C-sections than vaginal births performed DW, but more vaginal births than C-sections were performed after working hours. Concordant births took place mostly AOD for vaginal births (25), but DW for C-sections (23).
The patients distinguish clearly between birth pain alone and their overall birth experience. Patients’ mean scores for their birth pain were 7.535 (SD=2.756) for vaginal birth and 6.111 (SD=3.745) for C-section; thus, patients who would have chosen C-section assessed lower their birth pain (p<0.05). The mean scores based on the actual mode of delivery were 7.625 (SD=2.666) for vaginal birth, and 6.511 (SD=3.501) for C-section (p>0.05).
Birth pain is best rated for AOD (7.73), followed by AON (7.33) and DW (6.59). The largest proportion of unsatisfied women by their birth pain is found in patients who gave birth DW. The average scores of patients’ assessment of their birth and birth pain depending on the time of birth indicate that women rate the highest births AON (9.04) compared to births during daytime (8.83 is the score for DW and AOD).
Patients who preferred C-section and gave birth by C-section offered higher mean scores for the medical personnel, compared to patients who preferred vaginal birth (p>0.05) – 9.97 (SD=0.40) versus 9.91 (SD=0.18) for obstetricians, 9.69 (SD=0.99) versus 9.69 (SD=0.68) for anaesthetists, and 9.75 (SD=0.67) versus 9.72 (SD=0.80) for midwives.
Discussion
In our study, 28.2% of women preferred C-section, and 70.1% preferred vaginal birth. After birth, the percentage of C-sections increased to 44.4%, showing a difference between the actual and the preferred mode of delivery of 16.2 percentage points (57.4%) in favour of C-section. The preference for C-section in our sample seems higher than 0.3 to 16%, revealed by meta-analyses and other observational reviews(9-11).
Doctors’ profiles reveal that specialists and consultants attended the largest share of nonconcordant births, while residents and young senior doctors attended mostly vaginal births. There are no significant differences in the time spent in the labor room among doctors’ categories, except for residents, who had the highest share of births beyond 5 hours (58.3%). But patients do not seem to differentiate their assessment of birth and birth pain depending on the type of doctor who attended their delivery. We found a negative correlation between the time spent in the labor room and birth pain assessment. Less than 5 hours spent in the labor room were correlated with very good scores for birth and birth pain.
Studies from countries with a low incidence of C-section show that patient’s satisfaction is not influenced by the delivery method, but patients would have preferred to be involved in the decision of delivery method(12,13). In our study, patients who would have chosen C-section assessed better their birth.
The average total monthly income of Romanian households increased by 80.3% between 2006 and 2014, and it almost doubled in 2019. There is an increase in the average age of mothers at first birth from 22.3 years old in 1990 to 27.4 years old in 2018(14). The increase in hospital beds in the private sector was 97.2 times between 1999 and 2014(15). Correspondingly, women giving birth are not reluctant in paying for the C-section bill either in a public or private hospital, although the costs are not meager. Therefore, it is not surprising to find that the percentage of women giving birth in some Romanian clinics and hospitals reached 80%(15).
To the best of our knowledge, this is the first survey about the preferred versus actual mode of birth in a Romanian hospital. There seems to be a degree of awareness and mature consciousness and preparedness towards the excess of C-section in Romania, as proven by some recent political actions. In 2019, the Commissions for Public Health and Human Rights, Equal Opportunities, Cults, and Minorities of the Romanian Parliament organized a debate on public strategies and policies for supporting natural birth and management of caesareans in Romania(16). The debate ended with a statement that encouraged giving birth by vaginal delivery, which adds to the consolidation of indications for C-section at the level of the Romanian Gynecological Society. Other countries’ example(17,18) proves that interventions focused only on the medical side were not successful.
Strengths and limitations. The strengths of this preliminary study are represented by a homogenous population, given that the same obstetrician who supervised pregnancy delivered the baby as well. This represents an optimal doctor-patient communication situation during pregnancy. The sample size represents a limitation due to the available data and the general lack of official data on C-sections and birth process in Romania. The C-section rate in February 2014 in the unit was 64%, but only 44% of the 117 women interviewed underwent a C-section; as a result, women who had a C-section were underrepresented in the sample. For these reasons, our findings cannot be generalized to all women giving birth in Romania. Nevertheless, we offer first-time insight into Romanian women’s preferences for their mode of delivery and sketch a profile of both patients and doctors involved in the process. Thus, C-section rates across countries should be similar and based on patients’ medical situations, and not on subjective approaches.
Conclusions
Our work aims at raising awareness about the high rate of C-sections in Romania by outlining the profile of patients and doctors behind the choice of C-section as a mode of delivery. We show that, despite the preference of vaginal birth before the onset of labor, the difference between the preferred versus actual birth method may be explained by patients’ perception on C-section as a better and faster procedure, with a lower degree of pain and safer for the fetus. Moreover, the Romanian healthcare system particularities regarding birth have consolidated a higher weight of patients’ voice in the decision regarding the mode of delivery, beyond and despite medical indications. Improving patients’ confidence in the healthcare system, built on competence and fitted hierarchical team position, may lead to choosing the optimal way of birth for childbirth safety and pain control.
Still, questions remaine to be addressed as further research directions. Among them, the critical ones refer to the reliability and accuracy of information sources that pregnant women use before deciding on their mode of delivery, the link between sexual education and the choice of delivery mode, and the desired communication patterns between doctors and patients during pregnancy. One important further research direction should address doctors’ motivations towards performing more C-sections than medically needed and the proper public policy measures to encourage safe natural births.
Declarations. Ethics approval and consent to participate. Data for this study were collected in 2014, within a research grant 20062, approved by the “Carol Davila” University of Medicine and Pharmacy, Bucharest, Romania, and by the maternity management. The participation in the study was voluntary. Datasets used for analysis in the current study are available from the corresponding author on request.
Acknowledgments: We would like to express our deepest appreciation for the time and invaluable comments and suggestions received from Professor Ana Pilar Betrán, leading WHO expert on caesarean sections, regarding our manuscript. The current version reflects the engaging insight that professor Betrán offered to us.
Conflict of interests: The authors declare no conflict of interests.
Bibliografie
-
Boerma T, Ronsmans C, Melesse DY, et al. Global epidemiology of use and disparities in caesarean sections. Lancet. 2018;392(10155):1341-8.
-
Betrán AP, Ye J, Moller A-B, et al. The increasing trend in caesarean section rates: global, regional and national estimates: 1990-2014. PLoS One. 2016;11(2):e0148343.
-
Visser GHA, Ayres-de-Campos D, Barnea ER, et al. FIGO position paper: how to stop the caesarean section epidemic. Lancet. 2018;392(10155):1286-7.
-
STATISTA : https://www.statista.com/topics/5217/cesarean-sections/ Accessed: Oct 2020.
-
STATISTA: https://www.statista.com/statistics/807132/infant-mortality-in-romania/ Accessed: Oct 2020.
-
https://www.macrotrends.net/countries/ROU/romania/infant-mortality-rate Accessed: Oct 2020.
-
Betrán AP, Torloni MR, Zhang JJ, Gülmezoglu AM, WHO Working Group on Caesarean Section. WHO Statement on Caesarean Section Rates. BJOG. 2016;123(5):667-70.
-
Opiyo N, Kingdon C, Oladapo OT, et al. Non-clinical interventions to reduce unnecessary caesarean sections: WHO recommendations. Bull World Health Organ. 2020;98(1):66-8.
-
Mazzoni A, Althabe F, Liu NH, et al. Women’s preference for caesarean section: a systematic review and meta-analysis of observational studies. BJOG. 2011;118(4):391-9.
-
Kingdon C, Baker L, Lavender T. Systematic review of nulliparous women’s views of planned cesarean birth: the missing component in the debate about a term cephalic trial. Birth. 2006;33(3):229-37.
-
McCourt C, Weaver J, Statham H,et al. Elective cesarean section and decision making: a critical review of the literature. Birth. 2007;34(1):65-79.
-
Loke AY, Davies L, Mak YW. Is it the decision of women to choose a cesarean section as the mode of birth? A review of literature on the views of stakeholders. BMC Pregnancy Childbirth. 2019;19(1):286.
-
Karlström A, Nystedt A, Hildingsson I. A comparative study of the experience of childbirth between women who preferred and had a caesarean section and women who preferred and had a vaginal birth. Sex Reprod Healthc. 2011;2(3):93-9.
-
National Institute of Statistics. Tempo database. https://insse. www.insse.ro. Accessed: May 2020.
-
National Institute of Statistics. Social trends, 2019. https://insse.ro/cms/sites/default/files/field/publicatii/social_trends_in_2020_0.pdf. Accessed: June 2020.
-
Botnariu E. România este pe primul loc în Europa în privinţa proporţiei naşterilor prin cezariană din totalul naşterilor din ţară. Ro Health Review. 2019. https://rohealthreview.ro/botnariu-romania-este-pe-primul-loc-in-europa-in-privinta-proportiei-nasterilor-prin-cezariana-din-totalul-nasterilor-din-tara/. Accessed: June 2020.
-
Montilla P, Merzagora F, Scolaro E, et al. Lessons from a multidisciplinary partnership involving women parliamentarians to address the overuse of caesarean section in Italy. BMJ Global Health. 2020;5(2):e002025.
-
Eide KT, Morken NH, Bærøe K. Maternal reasons for requesting planned cesarean section in Norway: a qualitative study. BMC Pregnancy Childbirth. 2019;19(1):102.
Articole din ediţiile anterioare
Managementul obstetrical al septului vaginal longitudinal descoperit în timpul travaliului – prezentare de caz
Septul vaginal longitudinal este o anomalie congenitală cu o incidenţă rară, având simptome limitate sau chiar inexistente. De cele mai multe ori, ...
Tipuri actuale de naştere şi impactul lor asupra mamei şi fătului
În urma evoluţiei modalităţii de naştere, am constatat, potrivit unui studiu observaţional efectuat în clinica noastră în perioada 2017-2021, o ten...
Naşterea la domiciliu în România – studiu retrospectiv
Cu toate că naşterea vaginală este considerată un proces fiziologic, specialiştii consideră că este un act care se recomandă a fi asistat de cadre ...
Sarcina cicatricială după operaţia cezariană – o continuă dilemă terapeutică. Serie de cazuri şi review al literaturii
Sarcina cicatricială după operaţie cezariană (CSP) este o tulburare iatrogenă care pune viaţa în pericol, cu o incidenţă tot mai mare, din cauza cr...