Objective. To share our experience in the prenatal diagnosis of agenesis of ductus venosus (ADV) secondary to interrupted inferior vena cava (IIVC) and how does this affect the outcome. Methodology. A prospective study has been conducted in our center regarding the ADV outcome, since October 2016. In all cases, the main features of abdominal fetal circulation were evaluated in all second-trimester ultrasound scans, including the presence of a normal drainage of the umbilical vein, via ductus venosus, and the normal location of inferior vena cava (IVC). We present an analysis regarding the outcome of the ADV cases secondary to IIVC and we compare our data with those from the literature. Results. A total of five cases with prenatally diagnosed ADV and IIVC were identified. The gestational age at diagnosis ranged from 18 to 27 weeks. Karyotyping was performed in all cases but one, with an abnormal result in one case. Two cases were part of left isomerism syndrome and had an unfavorable outcome. Two cases did not present other anomalies and had a good outcome, according to the neonatal and pediatric cardiology follow-up. Conclusions. Postnatal outcome in cases with ADV and IIVC mainly depends on the presence of concomitant malformations. In isolated cases, the prognosis is generally good, but counseling is often difficult in such cases, and it is very important to exclude other structural or genetic anomalies.
Consilierea în agenezia ductului venos secundară venei cave inferioare întrerupte
Counseling in agenesis of ductus venosus secondary to interrupted inferior vena cava
First published: 23 decembrie 2020
Editorial Group: MEDICHUB MEDIA
DOI: 10.26416/ObsGin.68.4.2020.4033
Abstract
Rezumat
Obiectiv. Scopul studiului este acela de a prezenta experienţa noastră în diagnosticul prenatal al ageneziei de duct venos care apare secundar ageneziei venei cave inferioare, precum şi stabilirea modului în care aceasta afectează prognosticul. Metodologie. Din octombrie 2016, în centrul nostru se desfăşoară un studiu prospectiv cu privire la prognosticul cazurilor cu agenezie de duct venos. În toate cazurile, principalele caracteristici ale circulaţiei fetale abdominale au fost evaluate în toate examinările ecografice efectuate în al doilea trimestru de sarcină, inclusiv prezenţa unui drenaj normal al venei ombilicale prin ductul venos şi localizarea normală a venei cave inferioare. Prezentăm o analiză cu privire la prognosticul cazurilor cu agenezie de duct venos secundară absenţei venei cave inferioare şi comparăm datele noastre cu cele din literatura de specialitate. Rezultate. Au fost diagnosticate prenatal cinci cazuri cu agenezie de duct venos secundară ageneziei de venă cavă inferioară. Vârsta gestaţională la diagnostic a variat între 18 şi 27 de săptămâni. Cariotiparea a fost efectuată în patru cazuri. S-a identificat un rezultat anormal. Două cazuri au prezentat izomerism atrial stâng şi au avut un prognostic nefavorabil. Celelalte două cazuri nu au prezentat alte anomalii asociate şi au avut un prognostic bun, potrivit monitorizării cardiologice neonatale şi pediatrice. Concluzii. Prognosticul postnatal în cazurile cu agenezie de duct venos şi agenezie de venă cavă inferioară depinde în principal de prezenţa malformaţiilor concomitente. În cazurile izolate, prognosticul este în general bun, dar consilierea este adesea dificilă şi este foarte important să se excludă alte anomalii structurale sau genetice.
Introduction
The ultrasound (US) examination of the fetal venous system has exposed a wide spectrum of malformations. These abnormalities of the venous system, especially of the caval system, may be associated with anomalies of the heart, intestinal tract and with anomalies of the symmetry of the body.
Azygos continuation of the inferior vena cava (IVC) has a prevalence of about 1.5% in the general population (range: 0.2-3%)(1). Traditionally, this venous anomaly was thought to be strongly associated with congenital heart disease and polysplenia. However, the widespread prenatal diagnosis and postnatal evaluations revealed that interrupted inferior vena cava (IIVC) can evolve isolated and asymptomatic(2). As an isolated finding, IIVC with azygos or hemiazygos continuation requires no treatment.
Improved ultrasound technology with the addition of color and spectral Doppler imaging has changed the assessment of fetal circulation and resulted in the increasing number of cases with a prenatal diagnosis of agenesis of ductus venosus (ADV). Also, it has been proven the ability of first-trimester (FT) screening in the detection of agenesis of the ductus venosus(3). The prognosis of the ADV is also controversial and is related either to the type of the umbilical shunt (intra- or extrahepatic), caliber of the shunt, the association with other fetal abnormalities and the nuchal translucency (NT) measurement(4-7).
The overall aim of fetal anomaly screening is to identify potential anomalies, so that parents can make an informed choice, and to improve the safety of delivery. The increase of ultrasound use highlighted questions regarding the appropriate management in cases with rare anomalies. Unfortunately, the reports regarding agenesis of ductus venosus with interrupted vena cava are rare and the long-term follow-up is not easy to assess, therefore for further cases the counseling becomes difficult.
Methodology
This is a prospective study conducted in our tertiary center (Prenatal Unit of the County Emergency Clinical Hospital of Craiova), between October 2016 and October 2020. We included the fetuses diagnosed with ADV and interrupted IVC. The examination of the DV was performed with the image magnified, so that the fetal thorax and abdomen occupied the whole screen. The presence of the normal hepatic segment of IVC was confirmed on the abdominal axial planes at the level of circumference biometry plane. In cases with IVC interruption, the azygos or hemiazygos vein were identified and showed in upper planes to drain into the superior vena cava (SVC) – Figure 4. Maternal characteristics and medical history along with fetal associated anomalies were noted. The written informed consent was obtained before US examination. The examinations were carried out by several certified sonographers. We compared our results with the ones from published studies, which were identified via PubMed and Scopus search, using the keywords: inferior vena cava agenesis, ADV outcome.
Results
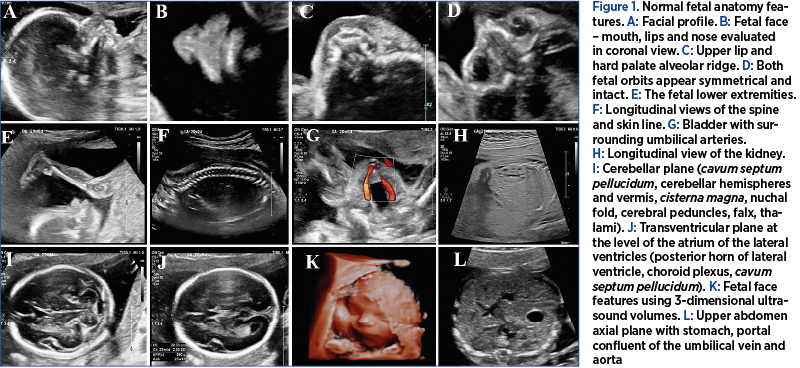
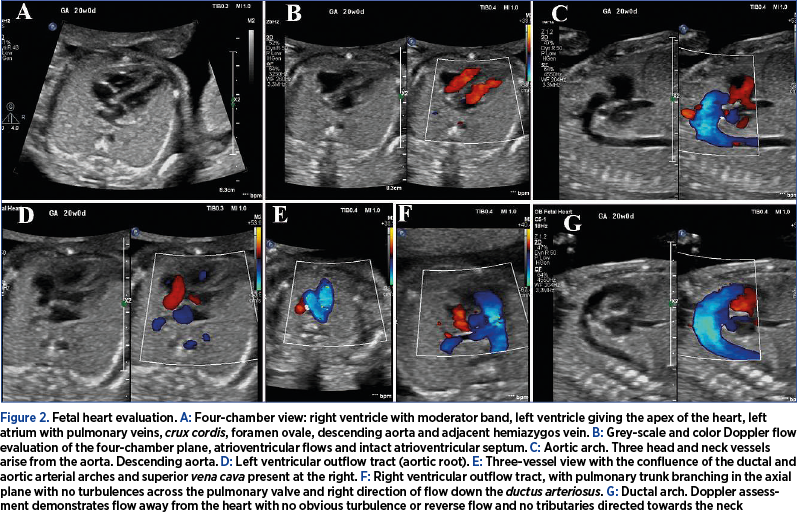
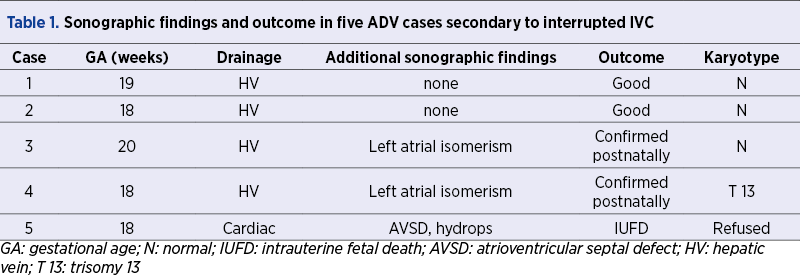
During the study period, the assessment of the DV and IVC was carried out in 4000 pregnancies. We identified a total of five cases with prenatally ADV and IIVC, with a prevalence of 0.12%. The prenatal findings and outcome of the five cases are summarized in Table 1. Two ADV cases with IIVC were isolated (Figure 1), one case was associated with atrioventricular septal defect and hydrops, and two were part of the left isomerism syndrome. The latter two cases of IIVC presented azygos continuation. From the two isolated cases, one presented hemiazygos continuation (Figures 2-4) and the other with azygos drainage. Genetic evaluation was performed in four cases, and trisomy 13 was found in one case. One couple declined genetic assessment.


Discussion
Agenesis of the ductus venosus results from the failure to form the “critical anastomoses” between the portal-umbilical venous system and the hepatic-systemic venous system, shunting the umbilical blood through an aberrant vessel. Two main subgroups can be distinguished: intrahepatic drainage through the portal sinus to the portal venous system (PVS) or a hepatic vein, without giving rise to the DV (umbilicoportal-hepatic shunt). The other group is the one with extrahepatic course of the umbilical vein with liver bypass; the UV does not connect to the PVS and drains into a systemic vein (the inferior vena cava, right atrium or, rarely, the left atrium, coronary sinus or iliac vein)(8,9). Intrahepatic drainage has been reported to have a favorable prognosis, 80-100% of cases having a normal outcome(4,10).
In our study, less than half of the cases with IIVC and secondary ADV were isolated and presented a good outcome. However, the small number of cases, due to the rarity of the disease, did not allow us to draw strong conclusions. In our cases, IIVC associated an umbilical drainage usually into the hepatic circulation – hepatic veins and portal system. One case presented with extrahepatic drainage, into the right atrium, with the subsequent development of hydrops. The poor prognosis seems to be related to the associated abnormalities rather than to the site of umbilical vein drainage.
IIVC is a rare congenital anomaly. This anomaly results from the primary failure of the right subcardinal vein to connect with the hepatic segment of the inferior vena cava, shunting its blood directly into the right supracardinal vein. The blood which drains the inferior part of the body reaches the heart by way of the azygos or hemiazygos vein and superior vena cava(11). This anomaly seems to be a good indicator for the presence of atrial isomerism and the polysplenia syndrome(12,13). We identified a total of five ADV cases with IIVC, out of which 40% were part of the left isomerism syndrome. This study is in line with previous publications, IIVC being usually associated with cardiac and extracardiac malformations, as part of the isomerism syndrome. The association of IIVC with congenital heart diseases has been reported to be an important marker of symptoms severity and a prognostic factor(14). The two survivors with left atrial isomerism had a two-year follow-up, with the developing of heart block and surgical correction.
In cases of isolated IIVC, usually there is no treatment regime required. The patients are often asymptomatic, but deep venous thrombosis rate seems to be increased after birth(15,16). The evaluation of the cases from our study had a multidisciplinary approach along with a fetal cardiologist. 40% of our cases were isolated and had a good outcome at birth and on short-term follow-up. A detailed cardiac evaluation was performed at two-month postnatal age, which confirmed the prenatal diagnosis of inferior vena cava agenesis with hemiazygos and azygos continuation to superior vena cava. The isolated cases were followed-up on a period of one year postnatally and the development of the infants was according to their age.
Usually, the isolated abnormality of the venous system represents a self-limiting clinical problem. Most of the previous cases of IIVC and hemiazygos continuation have been reported in adults(4), while the few cases reported in fetuses do not have a long-term follow-up. The key finding of this study represents the diagnosis of ADV associated with IIVC, showing a good outcome on the short-term evaluation in isolated cases. Of course, there are limitations of the study, due to the lack of follow-up, which could provide information about the long-term consequences.
The value that the study adds to the current literature is represented by the recognition and description of ADV secondary to IIVC and hemiazygos or azygos continuation and its short-term outcome. We would like to underline the fact that counseling is often difficult in such cases, where a conflict emerges when combining the contradictory prognosis of two rare conditions: the reserved ADV outcome and the well-known overall good development of the IIVC individuals.
The postnatal outcome in cases with ADV and IIVC mainly depends on the presence of concomitant malformations. Thus, in such cases, we believe that it is very important to exclude other structural or genetic anomalies. Limited postnatal long-term follow-up does not allow us to draw safe conclusions, but prenatal counseling for this anomaly should include the likelihood of later increased risk for venous thrombosis.
Bibliografie
-
1. Bass JE, Redwine MD, Kramer LA, et al. Spectrum of congenital anomalies of the inferior vena cava: cross-sectional imaging findings. Radiographics. 2000 May-Jun;20(3):639-52.
-
2. Ghandour A, Partovi S, Karuppasamy K, Rajiah P. Congenital anomalies of the IVC – embryological perspective and clinical relevance. Cardiovasc Diagn Ther. 2016;6(6):482-492.
-
3. Iliescu DG, Cara ML, Tudorache S, Antsaklis P, Novac LV, Antsaklis A, Cernea N. Agenesis of ductus venosus in sequential first and second trimester screening. Prenat Diagn. 2014;34(11):1099-105.
-
4. Berg C, Kamil D, Geipel A, et al. Absence of ductus venosus – importance of umbilical venous drainage site. Ultrasound Obstet Gynecol. 2006;28:275–281.
-
5. Jaeggi ET, Fouron JC, Hornberger LK, Proulx F, Oberhänsli I, Yoo SJ, Fermont L. Agenesis of the ductus venosus that is associated with extrahepatic umbilical vein drainage: prenatal features and clinical outcome. Am J Obstet Gynecol. 2002;187(4):1031-7.
-
6. Shen O, Valsky DV, Messing B, Cohen SM, Lipschuetz M, Yagel S. Shunt diameter in agenesis of the ductus venosus with extrahepatic portosystemic shunt impacts on prognosis. Ultrasound Obstet Gynecol. 2011;37(2):184-90.
-
7. Iliescu DG, Tudorache S, Cernea D. Agenesis of ductus venosus with complex intra- and extrahepatic umbilical drainage. J Obstet Gynaecol Res. 2014 Apr;40(4):1163-4.
-
8. Yagel S, Kivilevitch Z, Cohen SM, Valsky DV, Messing B, Shen O, Achiron R. The fetal venous system. Part II: ultrasound evaluation of the fetus with congenital venous system malformation or developing circulatory compromise. Ultrasound Obstet Gynecol. 2010;36(1):93-111.
-
9. Strizek B, Zamprakou A, Gottschalk I, Roethlisberger M, Hellmund A, Müller A, Gembruch U, Geipel A, Berg C. Prenatal Diagnosis of Agenesis of Ductus Venosus: A Retrospective Study of Anatomic Variants, Associated Anomalies and Impact on Postnatal Outcome. Ultraschall Med. 2019;40(3):333-339.
-
10. Contratti G, Banzi C, Ghi T, Perolo A, Pilu G, Visentin A. Absence of the ductus venosus: report of 10 new cases and review of the literature. Ultrasound Obstet Gynecol. 2001;18:605–609.
-
11. Fasouliotis SJ, Achiron R, Kivilevitch Z, Yagel S. The human fetal venous system: normal embryologic, anatomic, and physiologic characteristics and developmental abnormalities. J Ultrasound Med. 2002;21(10):1145-58.
-
12. Pepes S, Zidere V, Allan LD. Prenatal diagnosis of left atrial isomerism. Heart. 2009;95:1974–7.
-
13. Phoon CK, Villegas MD, Ursell PC, Silverman NH. Left atrial isomerism detected in fetal life. Am J Cardiol. 1996;77:1083–8.
-
14. Colak MH, Rahman A, Kocaturk H, Bayram E, Kocakoc E. Interrupted inferior vena cava and partial anomalous pulmonary venous return with atrial septal defect in a 38-year-old adult: a case report. Cases Journal. 2009;2(1):7346–7351.
-
15. Lambert M, Marboeuf P, Midulla M, Trillot N, Beregi JP, Mounier-Vehier C, et al. Inferior vena cava agenesis and deep vein thrombosis: 10 patients and review of the literature. Vasc Med. 2010;15:451–9.
-
16. Saba L, Mallarini G. A study of inferior vena cava anomaly: Evaluation using multi-detector-row CT angiography. Eur J Radiol Extra. 2008;68:37–40.
Articole din ediţiile anterioare
Prognosticul în cazul pentalogiei lui Cantrell
Pentalogia lui Cantrell este un sindrom congenital rar, considerat letal, care asociază în forma sa completă următoarele cinci defecte: defect la n...
Provocări în evaluarea feţei fetale – diagnostic şi management
The ultrasound assessment of the fetal face is the first way of interaction of the parents with their unborn baby, therefore recent achievements in...
Omfalocel, scrot bifid, hipospadias şi micropenis: rezultate clinice în cazuri cu cariotip normal
Acest studiu îşi propune să descrie caracteristicile, monitorizarea şi managementul unei malformaţii complexe: omfalocel, hipospadias, scrot bifid ...
Managementul prenatal şi postnatal în tetralogia Fallot
Anomaliile morfologice ale aparatului cardiovascular reprezintă o cauză majoră de morbiditate şi mortalitate neonatală. O ecografie fetală de rutin...