Background and objectives. Uterine artery embolization (UAE), or uterine fibroid embolization (EFM), a technique introduced in the conservative treatment of uterine fibroids in the 1990s, has been increasingly used in the last decades. The data accumulated in time revealed also, besides the expected benefits, some undesirable complications, initially unanticipated. The study aims at analyzing the histological changes of myometrium occurred after uterine artery embolization for fibroids. Materials and method. Presentation of a series of three cases that have undergone gynecologic surgery in the Bucur Maternity of the “Sf. Ioan” Emergency Clinical Hospital, Bucharest, after the embolization of the uterine arteries performed (in the past) for fibroids. Results. In two of the three cases presented, it was practiced hysterectomy with bilateral anexectomy and in one case myometrectomy. At the histopathological examination, what was proven to be specific for the long-term effects of UAE was the thickening of vascular structures containing intraluminal amorphous material, with vascular and perivascular infiltration with giant multinucleated histiocytes around the foreign body. This histological aspect corresponds to a nonspecific granulomatous inflammation with giant cells. Conclusions. Embolization of the uterine arteries may cause a giant-cell type inflammation at the level of the myometrium and fibrosis, and this type of changes could be the cause of a poor prognosis for women who want a future pregnancy.
Efectele pe termen lung ale embolizării arterei uterine cauzate de materialul embolic
Long-term effects of uterine artery embolization caused by the embolic material
First published: 25 aprilie 2021
Editorial Group: MEDICHUB MEDIA
DOI: 10.26416/ObsGin.69.2.2021.5009
Abstract
Rezumat
Context şi obiective. Embolizarea arterei uterine (EAU), sau embolizarea fibromului uterin (EFM), tehnică introdusă în tratamentul conservator al fibromului uterin în anii 1990, a fost din ce în ce mai utilizată în ultimele decenii. Datele acumulate în timp au relevat, pe lângă beneficiile scontate, şi unele complicaţii nedorite, iniţial neprevăzute. Studiul vizează modificările histologice ale miometrului apărute după embolizarea arterei uterine pentru fibroame. Materiale şi metodă. Prezentarea unei serii de trei cazuri care au suferit o intervenţie chirurgicală ginecologică în Maternitatea Bucur, Spitalul de Urgenţă „Sf. Ioan”, Bucureşti, după embolizarea arterelor uterine, efectuată (în trecut) pentru fibrom. Rezultate. La două din aceste trei cazuri s-a practicat histerectomie cu anexectomie bilaterală, iar într-un caz, miometrectomie. La examenul histopatologic, ceea ce s-a dovedit a fi specific pentru efectele pe termen lung ale EAU a fost îngroşarea structurilor vasculare care conţin material amorf intraluminal, cu infiltraţie vasculară şi perivasculară cu histiocite gigantice multinucleate în jurul corpului străin. Acest aspect histologic corespunde inflamaţiei granulomatoase nespecifice cu celule gigantice. Concluzii. Embolizarea arterelor uterine poate provoca o inflamaţie cu celule gigante la nivelul miometrului şi fibroză, acest tip de schimbare putând fi cauza unui prognostic nefavorabil pentru femeile care doresc o sarcină viitoare.
1. Introduction
Uterine artery embolization (UAE), or uterine fibroid embolization (EFM), a technique introduced in the treatment of uterine fibroids in the 1990s, has been increasingly used in recent decades. The results of several trials appeared in the middle of the 2000-2010 decade, including those of Mara et al. (2006) randomized controlled trials, the REST and EMMY trials(1-4).
All of these studies reported an improvement of symptoms and of the quality of life following UAE, but they also reported a 28-32% reintervention rate after this initial procedure(3,4). However, for many women of reproductive age, seeking for conservative fibroid management, UAE has become a valid option, which led to an yearly increase in the number of this type of procedure. The accumulation of data on the results of this procedure revealed, besides the expected benefits, also side effects and complications, initially unanticipated(5,6). In order to provide a proper management of the uterine fibroid, both patient and physician should be aware and informed about all UAE possible effects. In fact, all treatment methods for uterine fibroids have advantages and disadvantages and, in order to help the physician and the patient to decide, national or even international dedicated registries should be created for comparing data on different treatment options for uterine fibroids(7,8).
The aim of this study was to evaluate the complications and side effects due to the foreign material on the myometrium and ovaries and, thus, the unwanted consequence of UAE, starting from a series of three cases.
2. Presentation of the case series
2.1. Case 1
A 41-year-old woman was admitted in our unit (“Sf. Ioan” Emergency Clinical Hospital, Bucur Maternity, Bucharest) for severe pelvic-abdominal pain. The symptoms started many years before and progressively increased in intensity in the last previous days. From the medical documents, we noticed that, eight years before, the patient underwent myomectomy for uterine fibroids, followed by UAE four years ago, for the reappearance of multiple fibroids.
The medical report indicated that polyvinyl alcohol (PVA) particles were used for UAE. The physical gynecological examination revealed globally enlarged uterus, similar to a 12-week pregnancy size, irregular, difficult to delimit, flanked to the left border by a structure of cystic consistency of approximately 9/8 cm. Abdominal and transvaginal ultrasound scan indicated enlarged uterus (97/75/50 mm), irregular, in an intermediate position, myometrium with inhomogeneous structure, and irregular thin endometrium; on the left board of the uterus there was a 87/79 mm structure with mixed appearance, both solid and liquid, without Doppler signal acoustic shadow and that could not be mobilized, suggesting adherence to the uterus.
At the general physical examination, there were noted grade III obesity (BMI 35.6) and varicose veins of the lower limbs. The surgical treatment was chosen, and at the surgery, an adhesion syndrome with the pelvis blocked by adhesions between the omentum, ileum, sigmoid colon, rectum and genitals was found. After lysis of adhesions, there could be noticed: an enlarged and irregular uterus, one endometriotic cyst in the left ovary of approximately 9 cm in diameter, multiple foci of endometriosis in the ovary and right salpinges, as well as disseminated in the pelvic area. Total hysterectomy with bilateral anexectomy was performed. The evolution was favorable and the patient was discharged on the seventh day postoperatively.
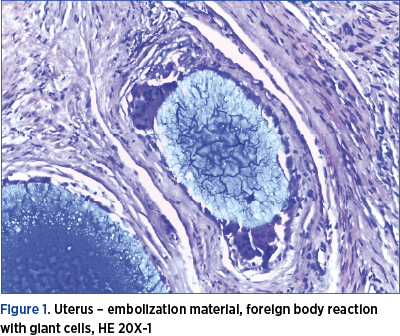
In addition to confirming endometriosis and adenomyosis, the histopathological exam revealed “diffuse fibrosis in the wall thickness, vascular structures with thickened wall and intraluminal amorphous material, perivascular inflammatory infiltration with giant multinucleate histiocytes of foreign body. Histological appearance of nonspecific giant-cell granulomatous inflammation” (Figure 1).
2.2. Case 2
A 52-year-old patient came to the “Sf. Ioan” Emergency Clinical Hospital, Bucur Maternity, Bucharest, for pelvic pain and irregular bleeding not responding to treatment. From the anamnesis, it was recorded that about 3 years ago she had been treated by a uterine artery embolization session, with polyvinyl alcohol particles, for multiple uterine fibroids. The gynecological and ultrasound examination confirmed the existence of an enlarged uterus, of 16/14/10 cm in volume, by the presence of several formations with dimensions up to 5 cm in diameter. The patient opted for total hysterectomy with bilateral adnexectomy. Pelvic adhesion syndrome was found intraoperatively. The postoperative evolution was good, the patient being discharged on the sixth postoperative day.
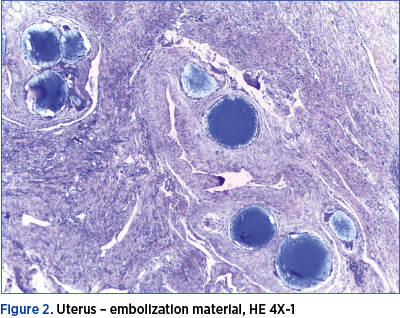
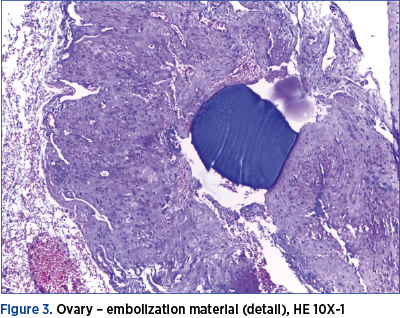
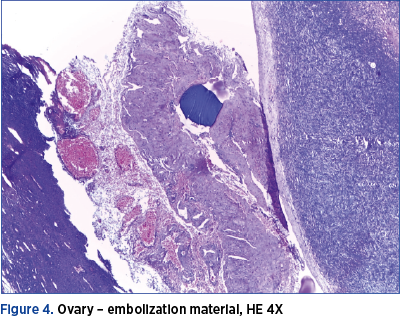
At the histopathological examination, beside the confirmation of the presence of fibroids, there were found vascular intraluminal amorphous material, vascular and perivascular infiltration with giant multinucleated histiocytes, diffuse fibrosis in the thickness of the uterine wall and also intravascular foreign body in the ovaries, with inflammatory reaction of the same type (Figures 2, 3 and 4).
2.3. Case 3
A 29-year-old patient presented herself at the “Sf. Ioan” Emergency Clinical Hospital, Bucur Maternity, Bucharest, for a uterine tumor, that was supposed to be a uterine fibroid of approximately 9 cm in diameter.
Following the anamnesis, it was recorded that, four years before, she had an UAE for a fibroid of about 8 cm in diameter and then, one year ago, she repeated the procedure because, after an initial reduction in size, to 5-6 cm in diameter, the uterine tumor began to grow again.
At her first UAE, there were used 700-900-micron gelatin microspheres (Embosphere®) and fragments of gelaspon for the second PVA particles. However, even after the second UAE, the tumor continued to grow. The patient was administered GnRH analogues for six months, but without remarkable results, and after that she was operated and myometrectomy was performed.
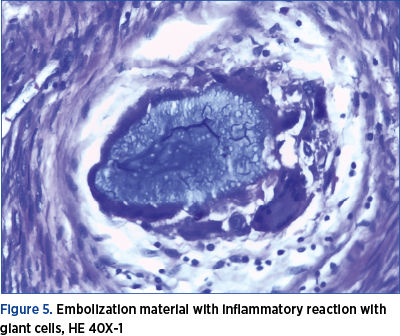
Intraoperatively, the tumor removal was difficult because it had an uneven, soft consistency and the uterine wall was also altered in terms of consistency and it was not possible to find a satisfactory cleavage space. Postoperatively, the evolution was favorable, the patient being discharged on the sixth day. The histopathological examination confirmed the diagnosis of uterine leiomyoma, but there were also observed in the surrounding myometrium the thickening of vascular structures containing intraluminal amorphous material, with vascular and perivascular infiltration with giant multinucleated histiocytes. The histological aspect corresponds to nonspecific granulomatous inflammation with giant cells (Figure 5).
3. Discussion
Historically, it is cited that the first successful embolization of the uterine arteries, for persistent metrorrhagia, in a woman with uterine fibroids, was performed in 1974, in Paris, by Dr. Jean-Jaques Merland(9). Afterwards, this method was adopted by Dr. Jacques Ravina, who initially used it preoperatively, to improve the conditions for performing myomectomy and reduce intraoperative bleeding. However, he found that, in a significant number of patients, the symptoms disappeared and the fibroids were significantly reduced in size.
In 1995, Dr. Ravina and Dr. Merland published in Lancet the first study, that included 16 pacients, about the use of UAE as a treatment for symptomatic fibroids(9). The symptoms were resolved in 11 patients, three patients had partial improvement, and there were two failures which required surgery(10).
In the USA, the promoter of the method was Dr. Goodwin, who published the results for the first 11 patients in 1997 in the Journal of Vascular and Interventional Radiology(11).
In a comparative study, Borah et al. (2017) showed that 82% of women with fibroids underwent hysterectomy as their first treatment procedure, almost 15% had myomectomy, and 3% underwent UAE and other modern sparing procedures(12).
The number of UAE has increased worldwide, Parker (2018) estimating that almost 30,000 procedures were performed in the USA and another 20,000 in the rest of the world(13).
As the number of UAE increases, it has become possible to have a clearer image about the effectiveness of the treatment and also about the possible failures, risks and complications(5,6,14). Numerous recent studies have shown that this procedure is effective, in selected cases, in reducing or remitting bleeding in 80-90% of cases, dysmenorrhea by 77%, in reducing the size of fibroids by 35-60% and the volume-related symptoms in 90% of cases(15-19).
At the same time, even though they are considered rare, there were recorded a series of complications and side effects. The complications may be related to the technique of the procedure or to the effect of the procedure itself. In the first category, there are included: arterial dissection, pseudoaneurysm, emboli in the lower limbs, hematoma at the puncture site, nerve damage, infection, allergic reaction to the contrast substance or nephropathy(18).
In the second category, there are the major complications of the embolization (itself): pulmonary embolism, uterine ischemia, necrosis, sepsis and death, but also other complications, such as necrosis of tissues other than the target, expulsion necrotic material, chronic leucorrhea, ovarian and sexual dysfunction, as well as a failure rate of the method ranging from 12% to 30%(18). The risk of death is 1 in 6,000 procedures (for comparison to hysterectomy, it is almost double).
The fertility may be compromised because some complications, even though they are rare, they can lead to hysterectomy, or the ovaries and fallopian tubes may be damaged by accidental embolization of their vascularization.
There were also studies that considered the consequences on the evolution of a future pregnancy(20,21).
In the study conducted by McLucas et al. (2001) on 139 women who wanted to maintain fertility, even though only 52 were below 40 years of age, after the procedure 17 pregnancies were obtained, of which five resulted in abortion(21).
According to another study, by Pron et al. (2005), 24 pregnancies were reported in 172 patients under the age of 40 who underwent UAE for the treatment of fibroids, of which six ended in abortion, four had premature births, four children had intrauterine growth retardation, and there were three cases with abnormal placenta (two with placenta praevia and one patient with placenta accreta)(22).
Walker and McDowell (2006) announced a series of 56 completed pregnancies in 33 women after UAE, ended with 33 live births(23).
Bonduki et al. (2011), in a retrospective study on 187 cases with UAE procedure for fibroids, reported only 16 pregnancies, but with a success rate of 87.5%, 14 births by caesarean section and, as serious complications, two cases of placenta accreta, one of them requiring hysterectomy for hemostasis(24).
Although pregnancy is possible, the risk of miscarriage, premature birth, postpartum hemorrhage and abnormal presentations is at least double than in women who haven’t performed UAE(25).
In a meta-analysis, Torre et al. (2014) summarized 6042 cases of UAE, of which 285 became pregnant after the procedure, being obtained 362 pregnancies, but only 208 pregnancies reached at term and eight were still ongoing at that time(26).
Some of the most plausible causes of these reserved pregnancy outcomes are the histological changes of the myometrium that occur after the UAE. At the level of fibroids, necrosis, dystrophic calcifications and vascular thrombosis typically appear, and the existence of foreign intravascular material determines the appearance of a giant-cell histiocytic reaction to a foreign body. Occasionally, however, foreign material was found in the myometrium, with the appearance of inflammatory phenomena, necrosis and microabscesses(27).
We noticed, in the cases we presented, long after UAE, the presence of the foreign material, detected in the vessels of the myometrium, generating inflammatory phenomena in the surrounding tissue, wearing the appearance of nonspecific giant-cell granulomatous inflammation. Somewhat surprisingly was the long-time persistence of the inflammatory processes. Perhaps this was one of the causes of the adhesion syndrome. This could also be the cause of the diffuse fibrosis in the thickness of the uterine wall. We also found embolic material in the ovaries in one of the cases, which confirms that embolic material can reach this level, unwanted, and can affect the ovaries.
One of the ways to refine this technique is to improve the materials used for embolization. New embolic materials have been tested and there are comparative studies on both their efficacy and tolerability.
Unfortunately, the data obtained so far do not reveal significant differences regarding the occurrence of the inflammatory reaction with giant cells at the presence of foreign material(28-30).
4. Conclusions
Important persistent giant-cell granulomatous inflammation around the embolic material is present long after UAE in the myometrium.
If the UAE is practiced in women who want a future pregnancy, the changes that may occur in the myometrium are likely to lead to a worse prognosis in terms of the evolution of the pregnancy.
Although the technique has evolved and the embolic material has diversified, accidental damage to the annexes is possible and can have significant consequences in terms of their functional capacity.
Bibliografie
-
Mara M, Fucikova Z, Maskova J, Kuzel D, Haakova L. Uterine fibroid embolization versus myomectomy in women wishing to preserve fertility: preliminary results of a randomized controlled trial. Eur J Obstet Gynecol Reprod Biol. 2006;126(2):226–233.
-
Mara M, Maskova J, Fucikova Z, Kuzel D, Belsan T, Sosna O. Midterm clinical and first reproductive results of a randomized controlled trial comparing uterine fibroid embolization and myomectomy. Cardiovasc Intervent Radiol. 2008;31(1):73–85.
-
Moss JG, Cooper KG, Khaund A, et al. Randomised comparison of uterine artery embolisation (UAE) with surgical treatment in patients with symptomatic uterine fibroids (REST trial): 5-year results. BJOG. 2011;118(8):936–944.
-
Hehenkamp WJ, Volkers NA, Birnie E, Reekers JA, Ankum WM. Symptomatic uterine fibroids: treatment with uterine artery embolization or hysterectomy – results from the randomized clinical Embolisation versus Hysterectomy (EMMY) Trial. Radiology. 2008;246(3):823–832.
-
Carrillo TC. Uterine artery embolization in the management of symptomatic uterine fibroids: an overview of complications and follow-up. Seminars in Interventional Radiology. 2008;25(4):378–386.
-
Memtsa M, Hayden H. Complications Associated with Uterine Artery Embolisation for Fibroids. Obstetrics and Gynecology International. 2012; Article ID 290542. https://doi.org/10.1155/2012/290542.
-
Stewart EA, Lytle BL, Thomas L, Wegienka GR, Jacoby V, Diamond MP, Nicholson WK, Anchan RM, Venable S, Wallace K, Marsh EE, Maxwell GL, Borah BJ, Catherino WH, Myers ER. The Comparing Options for Management: Patient-centered Results for Uterine Fibroids (COMPARE-UF) registry: rationale and design. Am J Obstet Gynecol. 2018;219(1):95.e1-95.e10.
-
Pleş L, Sima RM, Carp D, Florescu C, Dimitriu MCT, Ionescu CA. UPA effects on endometrium – what is the significance? Rom J Morphol Embryol. 2018;59(4):1127-1132.
-
Spies JS, Pelage JP. Uterine artery embolization and gynecologic embolotherapy. Philadelphia: Lippincott Williams & Wilkins; 2005, p. 3–18
-
Ravina JH, Herbreteau D, Ciraru-Vigneron N, et al. Arterial embolization to treat uterine myoma. Lancet. 1995;346:671–672.
-
Goodwin SC, Vedantham S, McLucas B, et al. Preliminary experience with uterine artery embolization for uterine fibroids. J Vasc Interv Radiol. 1997;8(4):517–526.
-
Borah BJ, Yao X, Laughlin-Tommaso SK, Heien HC, Stewart EA. Comparative Effectiveness of Uterine Leiomyoma Procedures Using a Large Insurance Claims Database. Obstet Gynecol. 2017;130(5):1047-1056.
-
Parker WH. Uterine Artery Embolization and Focused Ultrasound. Page last updated 2018. http://www.fibroidsecondopinion.com/uterine-artery-embolization/
-
Gonsalves C. Uterine Artery Embolization for Treatment of Symptomatic Fibroids. Semin Intervent Radiol. 2008 Dec;25(4):369-377.
-
Spies JB, Ascher SA, Roth AR. Uterine artery embolization for leiomyoma. Obstet Gynecol. 2001;98:29–34.
-
Walker WJ, Pelage JP. Uterine artery embolization for symptomatic fibroids: clinical result in 400 women with imaging follow up. BJOG. 2002;109:1262–1272.
-
Pron G, Bennett J, Common A, et al. The Ontario Uterine Fibroid Embolization Trial. Part 2. Uterine fibroid reduction and symptom relief after uterine artery embolization for fibroids. Fertil Steril. 2003;79(1):120–127.
-
Goodwin SC, Spies JB, Worthington-Kirsch R, et al. Uterine artery embolization for treatment of leiomyoma: long-term outcomes from the FIBROID Registry. Obstet Gynecol. 2008;111(1):22–33.
-
Hovsepian DM, Siskin GP, Bonn J, et al. Quality improvement guidelines for uterine artery embolization for symptomatic fibroids. J Vasc Interv Radiol. 2004;15:535–541.
-
Carpenter TT, Walker WJ. Pregnancy following uterine artery embolisation for symptomatic fibroids: a series of 26 completed pregnancies. BJOG. 2005;112:321–325.
-
McLucas B, Goodwin S, Adler L, Rapparort A, Perrella R. Pregnancy following uterine fibroid embolization. Int J Gynaecol Obstet. 2001 Jul;74(1):1-7.
-
Pron G, Mocarski E, Bennett J, et al. Pregnancy after uterine artery embolization for leiomyoma: Ontario multicenter trial. Obstet Gynecol. 2005;105(1):67–76.
-
Walker WJ, McDowell SJ. Pregnancy after uterine artery embolization for leiomyoma: a series of 56 completed pregnancies. Am J Obstet Gynecol. 2006;195:1266–1271.
-
Bonduki CE, Feldner PC, Silva J, Castro RA, Sartori MG, Girão MJ. Pregnancy after uterine arterial embolization. Clinics. 2011;66(5):807-810.
-
Goldberg J, Pereira L, Berghella V. Pregnancy after uterine artery embolization. Obstet Gynecol. 2002;100(5 Pt 1):869-72.
-
Torre A, Paillusson B, Fain V, Labauge P, Pelage JP, Fauconnier A. Uterine artery embolization for severe symptomatic fibroids: effects on fertility and symptoms. Hum Reprod. 2014; 29(3):490-501.
-
McCluggage WG, Ellis PK, McClure N, Walker WJ, Jackson PA, Manek S. Pathologic features of uterine leiomyomas following uterine artery embolization. Int J Gynecol Pathol. 2000;19(4):342-7.
-
Chiesa AG, Hart WR. Uterine artery embolization of leiomyomas with trisacryl gelatin microspheres (TGM): pathologic features and comparison with polyvinyl alcohol emboli. Int J Gynecol Pathol. 2004;23(4):386-92.
-
Rasuli P, Hammond I, Al-Mutairi B, French GJ, Aquino J, Hadziomerovic A, Goulet S, Jolly EE. Spherical versus conventional polyvinyl alcohol particles for uterine artery embolization. J Vasc Interv Radiol. 2008;19(1):42-6.
-
Lacayo EA, Richman DL, Acord MR, Wolfman DJ, Caridi TM, Desale SY, Spies JB. Leiomyoma Infarction after Uterine Artery Embolization: Influence of Embolic Agent and Leiomyoma Size and Location on Outcome. J Vasc Interv Radiol. 2017 Jul;28(7):1003-1010.
Articole din ediţiile anterioare
Impactul fibromului intramural asupra reproducerii la pacienţii supuşi procedurilor de FIV
Fibromul uterin este o tumoră benignă cu potenţial de alterare a procesului implantaţional. În acest studiu ne-am propus să examinăm impactul pe ca...
Sarcina cicatricială după operaţia cezariană – o continuă dilemă terapeutică. Serie de cazuri şi review al literaturii
Sarcina cicatricială după operaţie cezariană (CSP) este o tulburare iatrogenă care pune viaţa în pericol, cu o incidenţă tot mai mare, din cauza cr...
Inflamaţia în obezitatea maternă – mecanisme patologice şi impactul asupra rezultatelor naşterii şi a sănătăţii fătului
Creşterea prevalenţei obezităţii în rândul femeilor de vârstă reproductivă a condus la o proporţie semnificativă a sarcinilor la femei cu indice de...
Fibroamele uterine asociate sarcinii – este fezabilă miomectomia în sarcină? Review şi prezentare de caz
Mioamele uterine afectează 2-10% dintre femeile însărcinate. Sunt tumori dependente hormonal şi, în consecinţă, 30% dintre ele vor creşte ca răspun...