The 11-13-week scan is gaining a greater importance with the passing of time, as the diagnosis of more and more birth defects can be achieved at this time in pregnancy. The available guidelines for this scan are increasing, including new pieces of information that can be obtained on this occasion, and the diagnosis of open spina bifida and cleft lip and palate could be among them. The accuracy of the first-trimester detection of these two conditions has significantly increased during the past 10 years, and some of the views available for their diagnosis seem to offer a better performance in this instance.
REVIEW ARTICLES
Modalităţi de îmbunătăţire a diagnosticului anomaliilor fetale noncromozomiale la ecografia de rutină efectuată la 11-13 săptămâni de gestaţie
Ways of improving the diagnosis of fetal non-chromosomal abnormalities on routine ultrasound examination at 11-13 weeks of gestation
First published: 23 decembrie 2020
Editorial Group: MEDICHUB MEDIA
DOI: 10.26416/ObsGin.68.4.2020.4025
Abstract
Rezumat
Ecografia de screening de prim trimestru devine, cu timpul, tot mai importantă, odată cu posibilitatea diagnosticării a tot mai multe defecte fetale cu această ocazie. Ghidurile disponibile includ în mod progresiv tot mai multe informaţii care se pot obţine cu ocazia acestei examinări, iar diagnosticarea spina bifida deschise şi a cheilopalatoschizisului ar putea face parte dintre acestea. Acurateţea diagnosticului ecografic de prim trimestru în aceste două patologii a crescut semnificativ în ultimii 10 ani, iar unele dintre secţiunile utilizate în diagnosticul lor par a fi mai utile pentru a creşte rata de detecţie pentru fiecare caz în parte.
Introduction
Many years ago, the routine ultrasound (US) scans performed during the first trimester of pregnancy used to be dedicated mainly to the diagnosis of pregnancy, its location, the viability of the pregnancy, the gestational age and, of course, to the number of fetuses(1). The technological advances of the past decades led to an impressive increase in diagnostic possibilities, making the first-trimester scan one the most important exams performed during pregnancy.
In 2013, the International Society of Ultrasound in Obstetrics and Gynecology (ISUOG) issued a guideline on the performance of the first-trimester fetal ultrasound scan and, in 2014, the Romanian Society of Ultrasound in Obstetrics and Gynecology (SRUOG) issued the first Romanian guideline on the subject.
The last revision of the Romanian guideline was in 2019(2,3).
Birth defects detectable as early as the first-trimester scan
There is a growing number of birth defects that can now be detected at the early scans of the pregnancy. Out of these, some have proven to be so accurate in detection and easy to obtain, that they could be introduced in the routine of performing this scan.
Open spina bifida (OSB)
Intracranial translucency (IT) was first described in midsagital view in 2009. It is now widely used as an early diagnosis tool for OSB(4,5). The assessment of the IT can be performed in a sagital view of the fetus, the same view used for the assessment of the nuchal translucency (NT), but the view needed for the IT visualisation is rather less strict than the one for the NT, as this view doesn’t have to be perfectly midsagital in order to have a good IT assessment(4,5). The IT can also be assessed in an axial view, but with less acuracy for an unexperienced sonographer(5).
The IT is actually the fourth ventricle, but visualised in the NT view between the image of the brain stem (BS) and the one of the future cisterna magna (CM)(4,5). The translucency is bordered superiorly (or on the anterior) by the echogenic posterior edge of the BS and inferiorly (or on the posterior) by the choroid plexus of the 4th ventricle(4,5). It has normally a median size ascending from 1.5 to 2.5 mm in the period the crown-rump length (CRL) increases from 45 to 84 mm(4). It is abnormal or appears to be absent in cases with OSB, as the 4th ventricule, the choroid plexus of the 4th ventricle and the developing cisterna cerebellomedullaris are compressed by the caudal displacement of the brain(4,5). Common abnormal signs of an OSB are represented by the BS, which appears thickened, and the ratio of the brainstem to the brainstem – occipital bone (OB) distance, which is increased (>1)(5). In a recent meta-analysis, this ratio showed a high accuracy in detecting OSB(6) (Figures 1 and 2).


Cleft lip and palate (CLP)
Another birth defect that can be diagnosed today during the first trimester is the CLP. This diagnosis was initially detected at the time of the 11-13-week US examination using a coronal view, called the retronasal triangle(5), but it was also later detected using a sagital view, the maxilary gap(6), and then using a transverse view(7), which seems to be the most accurate view for detection at this time during pregnancy(8).
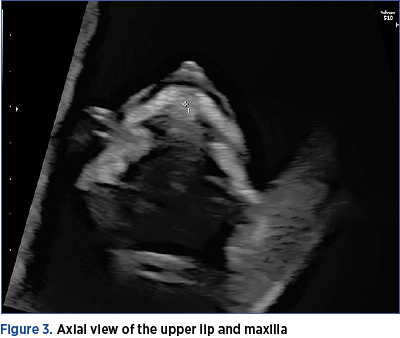
When we want to obtain the axial view of the lips and palate, we need to start from the view checking the fetal eyes and lenses and move slightly inferior until we reach the desired view and we should see the entire anterior part of the palate and the superior lip without any gaps. The fetal head should be oriented towards 12 o’clock (Figure 3).
Discussion
In 2011, A. Syngelaki analyzed the performance of the first-trimester screening for non-chromosomal abnormalities in a group of over 45,000 patients scanned between 2006 and 2009, and discovered a detection rate of only 5% for facial clefts and 15% for open spina bifida, a result which confirmed the findings for CLP from other previously published studies that were also showing a detection rate smaller than 10% at the 11-13-week scan(9). At the time, the author suggested placing all anomalies in three different categories, based on the possibility of detection during the first-trimester scan: anomalies that should always be detected, anomalies that are undetectable, and anomalies that are potentially detectable at this stage(9). Both open spina bifida and CLP fell in the third category at the time(9).
Following the publishing of different ways of diagnosing the open spina bifida and the CLP in the recent years, in 2019 A. Syngelaki has repeated the performance analysis for over 100,000 patients scanned between 2009 and 2018 and discovered a detection rate of 59% for open spina bifida and of 35% for CLP, with a major increase in the diagnosis rate since the last assessment.
In 2018, M.M. Zheng reported a detection rate of 100% for abnormal axial view of the maxilla in a smaller group of 2982 fetuses (including 315 twins), with 8 confirmed cases of CLP(8).
The variations in the severity of the condition will, however, keep these diagnoses in the third category, as the most severe cases are more likely to be discovered, while the less severe ones could pass undetected, but on the other hand, the severe cases are the ones that we are most interested in finding, as they pose the bigest threats to the fetus.
It is important to mention that the cleft lip only and the cleft palate only were not included in these numbers in the Syngelaki studies, as they are more difficult to be diagnosed, and they aren’t good candidates for routine check in the first trimester.
Conclusions
The abundance of anatomical elements that can be assessed today during the first-trimester screening scan created the need of guidelines on performing this exam and maximising its findings.
Based on a view that is already recommended in today’s guidelines, an important finding such as OSB could be detected just by recognising a pattern or by applying a measurement together with another measurement collected from that view anyway, so the assessment of OSB could be implemented as a routine check during the 11-13-week scan.
The CLP can also be detected during this scan, but for this diagnosis there is another view that might be necessary, as the palate in an axial view is not a standard view at this time, but it is fairly easy to obtain if we start from the view checking the fetal eyes and lenses.
Bibliografie
-
1. Pelinescu-Onciul D. Ecografia în obstetrică. Ed. Med. Amaltea, 1998.
-
2. Pelinescu-Onciul D, Vlădăreanu R, Stamatian F, Calomfirescu MV, Mărginean C, Mureşan D, Pleş L, Ceauşu I, Tudorache Ş, Iliescu D, Steriu M, Cheleş C, Rădulescu-Botică R, Veduţă A. Ghid de examinare ecografică de screening pentru anomalii de sarcină în trimestrul I. Societatea de Obstetrică şi Ginecologie din România; Societatea de Ultrasonografie în Obstetrică şi Ginecologie din România; Colegiul Medicilor din România, 2019.
-
3. Salomon LJ, Alfirevic Z, Bilardo CM, Chalouhi GE, Ghi T, Kagan KO, Lau TK, Papageorghiou AT, Raine-Fenning NJ, Stirnemann J, Suresh S, Tabor A, Timor-Tritsch IE, Toi A, Yeo G. ISUOG Practice Guidelines: performance of first-trimester fetal ultrasound scan. Ultrasound Obstet Gynecol. 2013;41(1):102-113.
-
4. Chaoui R, Benoit B, Mitkowska-Wozniak H, Heling KS, Nicolaides KH. Assessment of intracranial translucency (IT) in the detection of spina bifida at the 11-13-week scan. Ultrasound Obstet Gynecol. 2009 Sep;34(3):249-52.
-
5. Chaoui R, Nicolaides KH. Detecting open spina bifida at the 11-13-week scan by assessing intracranial translucency and the posterior brain region: mid-sagittal or axial plane? Ultrasound Obstet Gynecol. 2011 Dec;38(6):609-12.
-
6. Sirico A, Raffone A, Lanzone A, Saccone G, Travaglino A, Sarno L, Rizzo G, Zullo F, Maruotti GM. First trimester detection of fetal open spina bifida using BS/BSOB ratio. Arch Gynecol Obstet. 2020 Feb;301(2):333-340.
-
7. Sepulveda W, Wong AE, Martinez-Ten P, Perez-Pedregosa J. Retronasal triangle: a sonographic landmark for the screening of cleft palate in the first trimester. Ultrasound Obstet Gynecol. 2010 Jan;35(1):7-13.
-
8. Chaoui R, Orosz G, Heling KS, Sarut-Lopez A, Nicolaides KH. Maxillary gap at 11-13 weeks’ gestation: marker of cleft lip and palate. Ultrasound Obstet Gynecol. 2015 Dec;46(6):665-9.
-
9. Mărginean C, Săsărean V, Mărginean CO, Melit LE, Mărginean MO. Prenatal diagnosis of cleft lip and cleft lip palate – a case series. Med Ultrason. 2018 Dec 8;20(4):531-535.
-
10. Zheng MM, Tang HR, Zhang Y, Ru T, Li J, Xu BY, Gu Y, Xu Y, Hu YL. Improvement in early detection of orofacial clefts using the axial view of the maxilla. Prenat Diagn. 2018 Jun;38(7):531-537.
-
11. Syngelaki A, Chelemen T, Dagklis T, Allan L, Nicolaides KH. Challenges in the diagnosis of fetal non-chromosomal abnormalities at 11-13 weeks. Prenat Diagn. 2011 Jan;31(1):90-102.
-
12. Syngelaki A, Hammami A, Bower S, Zidere V, Akolekar R, Nicolaides KH. Diagnosis of fetal non-chromosomal abnormalities on routine ultrasound examination at 11-13 weeks’ gestation. Ultrasound Obstet Gynecol. 2019 Oct;54(4):468-476.