Burkitt lymphoma is one of the most aggressive non-Hodgkin lymphomas. The disease can be associated with extranodal involvement, especially in the structures of the neck and head, abdomen, kidneys and bone marrow. Breast involvement is rare. This type of lymphoma has an intrinsic propensity for central nervous system involvement. We report the case of an elderly patient diagnosed with Burkitt lymphoma with breast tumor and central nervous system infiltrates.
ONCOHEMATOLOGY
A rare case of highly aggressive Burkitt lymphoma with multiple extranodal involvements of the elderly
Un caz rar de limfom Burkitt agresiv cu multiple infiltrate extranodale la un vârstnic
Iuliana Iordan,
Andreea Neculcea,
Diana Emanuela Bonea,
Dragoş-Claudiu Popescu,
Alina Mititelu,
Andreea Spînu,
Paul Findrihan,
Raluca Nistor,
Ana Maria Prof. Dr. Vlădăreanu
First published: 25 martie 2022
Editorial Group: MEDICHUB MEDIA
DOI: 10.26416/OnHe.58.1.2022.6235
Abstract
Rezumat
Limfomul Burkitt este unul dintre cele mai agresive limfoame non-Hodgkin. Poate fi însoţit de determinări extranodale, cele mai frecvente fiind la nivelul extremităţii cefalice, abdomenului, rinichilor şi al măduvei osoase. Afectarea la nivelul sânului este mai rară. Are o tendinţă intrinsecă pentru determinări secundare la nivelul sistemului nervos central. Prezentăm cazul unei paciente vârstnice diagnosticate cu limfom Burkitt cu determinare mamară la debut, cu infiltrate ale sistemului nervos central în evoluţie.
Introduction
Burkitt lymphoma is one of the most aggressive types of non-Hodgkin lymphomas, characterized by a high turnover, a Ki-67 proliferation index approaching 100% and by elevated serum LDH levels(1,2). Burkitt lymphoma is often associated to Epstein-Barr virus and human immunodeficiency virus infections(3).
The malignant tissue in characterized by an increased proliferation of malignant cell and by increased apoptosis, resulting in a “starry sky” appearance(3). The neoplastic cells are intermediate-sized, having basophilic cytoplasm with vacuoles, and round nuclei with lacy chromatin and nucleoli(3).
The incidence in Europe is about 2 cases/1,000,000 people every year. The disease is classified by the World Health Organization (WHO) into three subtypes, based on epidemiology, risk factors and clinical presentation: sporadic, endemic and immunodeficiency-associated. However, their morphological and immunophenotypical features are similar(1,2).
Extranodal masses are common in Burkitt lymphoma. The most affected sites are the structures of the neck and head, bowels, kidneys and bone marrow. In women, it is possible for the primary involvement site to be either in the breast tissue or confined to the genital organs(4). Primary breast Burkitt type lymphoma occurs more rarely than in other types of lymphoma(2,5).
Case presentation
We report the case of a 76-year-old female admitted to our clinic for a rapidly progressive and painful left breast tumor, with extensive cutaneous infiltration extended in the chest and left arm and with axillary adenopathies. She had a good performance status – ECOG 1 (Eastern Cooperative Oncology Group). Her history was positive for neuroendocrine pancreatic tumor (diagnosed four years before presentation; in remission after octreotide and surgical treatment – pancreatectomy, splenectomy), hemorrhagic stroke (five years before presentation) and for SARS-CoV-2 infection (two months before presentation).
The clinical appearance of the left breast at the beginning was impressive – the tumor was about twice the size of the right breast, had a cyanotic color, with the appearance of orange peel, it was hardy and very painful to the touch.
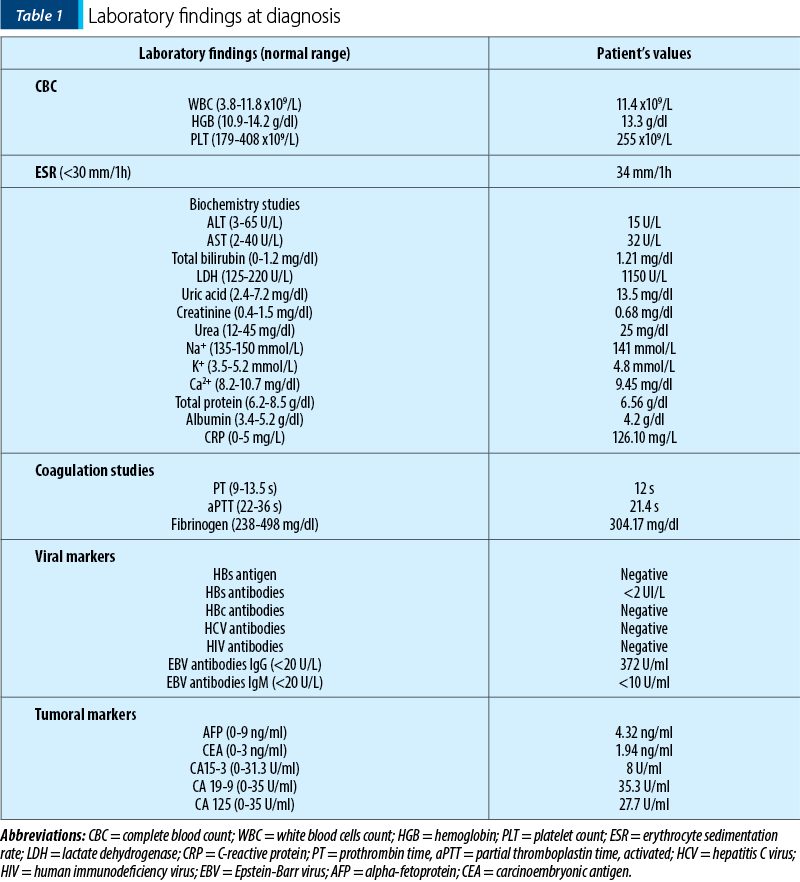
The laboratory findings at diagnosis were slight leukocytosis with left shift, significantly elevated LDH (lactate dehydrogenase), hyperuricemia and high inflammation markers (Table 1). The EBV IgG antibodies were positive.
A breast tumor biopsy was obtained. Histopathological and immunohistochemical tests confirmed the diagnosis of a high-grade B-cell non-Hodgkin lymphoma with a high proliferative index (Ki-67 98%), namely Burkitt lymphoma.
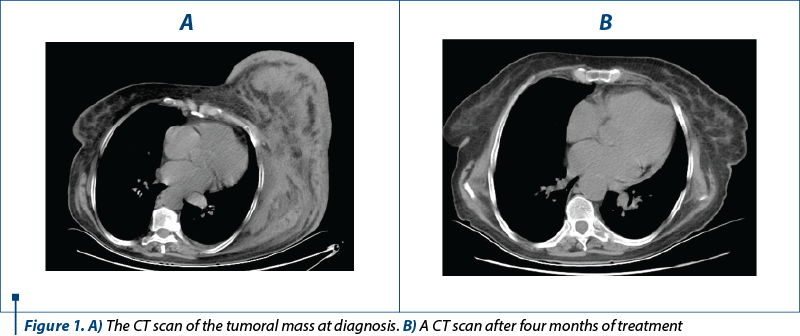
A CT scan (computed tomography) showed a proliferative tumor in the left mammary gland, infiltration in the soft tissue of the chest, and a large adenopathic mass in the left axilla (90/100/85 mm) – Figure 1A. No other lymphadenopathies were observed.
We established the diagnosis of stage IVB diffuse large B-cell non-Hodgkin lymphoma, Burkitt type. The International Prognostic Index stratified the patient as high-risk.
We started the treatment with chemoimmunotherapy, namely mini-hyper-CVAD associated with monoclonal antibody – anti-CD20 – rituximab, and intrathecal therapy. The patient was carefully monitored with repeated tests, considering the recent SARS-CoV-2 infection and the risk of reactivation. The most important complication of the first cycle was related to the tumor lysis syndrome, successfully managed with fractionated doses of chemotherapy, uricosuric treatment and intensive hydration.
After four months of treatment, the clinical and imaging parameters significantly improved. The clinical aspect of the left breast had a good resolution with only a residual hyperpigmentation. The size of the left breast returned to normal and the pain subsided after the first weeks of treatment.
The post-treatment CT scan showed only millimetric lesions in the left axilla, thus confirming the favorable evolution and the complete response (Figure 1B).
When recovering from medullary aplasia, the patient presented marked thrombocytosis – almost 1500x109/L. We excluded an associated myeloproliferative neoplasm – the JAK2, CALR, MPL mutations, and the BCR-ABL transcript were negative. After three weeks, the thrombocyte count returned to normal.
Only one month after completing treatment, erythematous plaques appeared on the left arm, which quickly developed into painful erythematous nodules. A second biopsy was taken from the plaques of the left arm and the diagnosis of skin involvement of non-Hodgkin lymphoma, mainly Burkitt lymphoma (Ki-67 100%), was established. We decided the start another line of treatment with the R-EPOCH regimen, dose adjusted for elderly, continuing also the CNS prophylaxis. After completing the first cycle, the patient was in close contact with a SARS-CoV-2 infected family member, therefore there was a treatment delay.
The patient received five cycles of R-EPOCH and obtained a significant regression of the skin lesions, but she started to develop various infections successfully treated according to the antibiogram.
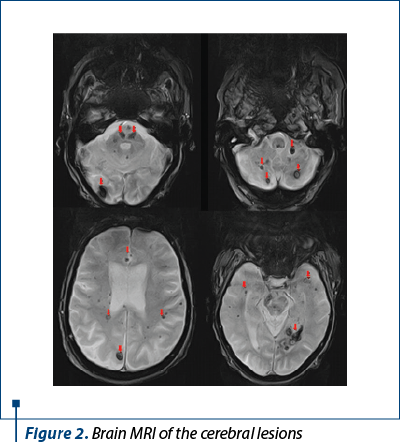
The patient developed paresthesia and decreased muscle strength in the upper limbs which progressively evolved into tetraparesis. A spinal MRI (magnetic resonance imaging) was done and showed hernias of the C4, C5, and C6 intervertebral discs and several stigmas for hemorrhage in the brainstem, cerebellum and spinal cord. We decided to perform a brain MRI that revealed multiple lesions in the brainstem, cerebellum, and cerebral hemispheres, suggestive of parenchymal involvement in amyloidosis or in the context of Burkitt lymphoma (Figure 2).
Cerebrospinal fluid was harvested for examination. The macroscopic and cellularity study showed blood contamination (RBC 7x109/L), probably from the multiple hemorrhages described on MRI. Therefore, immunophenotyping by flow cytometry could not be performed, and other methods for diagnosis (e.g., biopsy) were not feasible. The cerebrospinal fluid cultures were negative. Blood workup for systemic amyloidosis was negative. A CT scan excluded the subarachnoid hemorrhage.
Over time, the patient developed tetraparesis, more important in the left part of the body, severe paresthesia, and inability to maintain orthostatis. Due to the clinical context, we considered the brain lesions as secondary infiltration of the CNS by Burkitt lymphoma.
After almost eight months of treatment, the patient was frail (ECOG 4), had multiple and difficult to treat infections, therefore she could not tolerate systemic therapy with high doses of methotrexate. We considered radiation therapy as an appropriate treatment.
However, during the aplasia, the patient developed a neutropenic fever. An infectious screening was performed, including urinalysis, blood cultures, and a COVID-19 RT-PCR test. The results showed urinary tract infection with extensively drug-resistant Klebsiella pneumoniae that rapidly evolved towards sepsis. The patient also tested positive for SARS-CoV-2 infection. She received antibiotic therapy guided by the antibiogram and antiviral – remdesivir.
The clinical status of the patient deteriorated, despite the best supportive care and anti-infectious treatment. She developed severe anemia, thrombocytopenia and difficult to correct hydroelectrolytic disturbances: hypokalemia, hypocalcemia, hypomagnesemia due to comorbidities.
The intensive treatment for the current clinical and biological status of the patient is no longer an option. Thus, she receives only palliative care.
Discussion
Despite intensive treatment that substantially improved the prognosis of Burkitt lymphoma in children, in adults it remains poor. The prognosis depends also on the clinical and histological staging, serum LDH, additional cytogenetic anomalies besides MYC translocation, lack of response to therapy, and relapse disease(3). At diagnosis, our patient had multiple poor prognosis factors, such as advanced age (76 years old), advanced disease – stage IV B, infiltrative large tumoral mass, elevated serum LDH (more than five-fold the upper limit), and extranodal onset. The molecular and cytogenetical exams were not available. Despite the short-time poor prognosis of the disease, she had an impressive response to chemoimmunotherapy in the beginning, with remission of breast tumor and cutaneous infiltrate. During the treatment of cutaneous infiltrate, the disease progressed with CNS involvement.
The CNS involvement complicates 15-30% of cases and could be highlighted from the beginning or as a complication of a relapsed or resistant disease(6,7). The CNS involvement confers a particularly poor outcome(7). There are numerous risk factors for CNS involvement in aggressive B-cell lymphomas that consist in the histologic subtype (e.g., Burkitt lymphoma, diffuse large B-cell lymphoma), the extranodal involvement (e.g., uterus, testicle, breast), bone marrow involvement, and HIV-associated lymphoma(8,9). In our case, the patient had multiple risk factors for CNS involvement: the histologic subtype, breast involvement, age and the high value of serum LDH.
The clinical, biological and imagistic evaluations were not suggestive for CNS involvement at diagnosis. The neurological symptoms appeared progressively, during treatment, despite the CNS chemoprophylaxis according to the guidelines, and evolved rapidly towards tetraparesis.
The CNS involvement poses an even higher therapeutic challenge. Taking into account the severe immunosuppression and the low performance status, our patient is a candidate for palliative care at this moment.
Conclusions
We presented a rare case of Burkitt lymphoma of the elderly. The evolution of the disease was progressive, at the beginning the tumor affected only the left breast, after which the disease relapsed cutaneously – on the left arm and, finally, the disease involved the central nervous system.
Conflict of interests: The authors declare no conflict of interests.
The complications described in this article are not considered an adverse reaction to the medication.
Bibliografie
-
Greer JP, Rodgers GM, Glader B, et al. Wintrobe’s Clinical Hematology, 14th edition. Lippincott Williams and Wilkins, 2019.
-
Jacobson C, Ann LaCasce A. How I treat Burkitt lymphoma in adults. Blood. 2014;124(19):2913–2920.
-
Graham BS, Lynch DT. Burkitt Lymphoma. [Updated 2021 Oct 17]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available at: https://www.ncbi.nlm.nih.gov/books/NBK538148/
-
Vlădăreanu AM. Actualităţi în limfoamele nonhodgkiniene. Editura Amaltea, Bucureşti, 2016.
-
Wei J, Lin C, Xu C, et al. Primary Burkitt’s lymphoma of the breast without Epstein-Barr virus infection: A case report and literature review. Indian J Pathol Microbiol. 2015;58(4):546-549.
-
Blum KA, Lozanski G, Byrd JC, et al. Adult Burkitt leukemia and lymphoma. Blood. 2004;104(10):3009-3020.
-
Zayac AS, Evens AM, Danilov A, et al. Outcomes of Burkitt lymphoma with central nervous system involvement: evidence from a large multicenter cohort study. Haematologica. 2021;106(7):1932-1942.
-
Schmitz N, Zeynalova S, Nickelsen M, et al. CNS International Prognostic Index: A Risk Model for CNS Relapse in Patients with Diffuse Large B-Cell Lymphoma Treated With R-CHOP. J Clin Oncol. 2016;34(26):3150-3156.
-
Chin CK, Cheah CY. How I treat patients with aggressive lymphoma at high risk of CNS relapse. Blood. 2017;130(7):867-874.