Basal cell carcinoma (BCC) is the most common human malignancy worldwide. This paper bring in discussion the case of a 58-year-old patient who presented in our clinic with a protuberant formation at the internal left canthus having 2,3 cm in width and 3,5 in height, waxy surface, covered by telangiectases and central depression (3 mm in diameter). The tumor appeared 12 months ago as a small bump, with smooth surface, non-ulcerated and it had a small but constant growth achieving the present dimension. A surgical plan was made to find the suitable technique for covering the large defect of the internal canthus in the left eye. The purpose of the reconstruction is to restore the normal function of the periocular region with good aesthetic appearance and to diminish the donor site morbidity. We chose to cover the defect by using a local rotated cutaneo-adipos flap from the median forehead, known as the Indian flap. The result was very good. This procedure represents a perfect choice to reconstruct the defect of the face after excision of the periocular tumors.
Carcinom bazocelular al unghiului intern al orbitei - prezentare de caz
Basal cell carcinoma of the medial canthus - case presentation
First published: 24 noiembrie 2015
Editorial Group: MEDICHUB MEDIA
DOI: 10.26416/OnHe.33.4.2015.4344
Abstract
Rezumat
Carcinomul bazocelular este una dintre cele mai comune neoplazii cutanate la nivel mondial. Această lucrare prezintă cazul unui pacient în vârstă de 58 de ani, care s-a prezentat la clinica noastră cu o formaţiune protuberantă la nivelul unghiului intern al orbitei, având 2,3 cm în lăţime şi 3,5 cm în înălţime, suprafaţă ceroasă, acoperită de teleangiectazii şi cu o depresiune centrală (de 3 mm diametru). Tumora a apărut în urmă cu 12 luni, ca o mică excrescenţă cu suprafaţa netedă, fără ulceraţii, având o creştere lentă, dar constantă, până a atins dimensiunile de la momentul prezentării. A fost făcută o planificare chirugicală minuţioasă pentru a găsi tehnica potrivită de a acoperi defectul larg rămas în urma rezecţiei de la nivelul unghiului intern al ochiului stâng. Scopul reconstrucţiei este de a reface funcţia normală a regiunii perioculare, cu rezultate bune din punct de vedere estetic şi cu afectarea minimă a zonei de unde se prelevează grefa cutanantă. Am ales să acoperim defectul folosind un lambou local rotat cutaneo-adipos de la nivelul frunţii, procedură cunoscută ca „lambou indian”. Rezultatul a fost foarte bun. Această procedură reprezintă o alegere perfectă pentru reconstrucţia unui defect cutanat la nivelul feţei după excizia tumorilor periorbitare.
Introduction
Basal cell carcinoma (BCC) is the most common human malignancy worldwide. This type of cancer arises from nonkeratinizing cells that originate in basal layer of the epidermis. Although the incidence has risen sharply over the last several decades, the average age of diagnosis has steadily decreased because of improved awareness and surveillance. People having white skin and males (male-to-female ratio: 3:2) are predominantly affected. Elderly individuals are commonly affected, but BCC is becoming increasingly frequent in people younger than 50 years old. Basal cell carcinoma is rare in dark skin because of the inherent photoprotection of melanin and the melanosomal dispersion. Overall incidence is increasing worldwide significantly by 3-10% per year.
The vast majority of BCCs were located on the head and neck (70%). The most common clinical forms are the nodular and the superficial form which account for 90% of the cases. In the case of periocular tumors the most common site are: lower eyelid (48.9-72.1%), medial canthus (25-30%), upper eyelid (15%), lateral canthus (5%).
Risk factors for BCC have been well characterized and include ultraviolet light (UVL) exposure, light hair and eye colour, northern European ancestry, and inability to tan. An Italian study shows that sunburns have an important role in the development of BCC, and therefore intense sun exposure, rather than prolonged sun exposure, lead to the increase risk of BCC. A history of BCC is an increased risk for developing other lesions, thus 40% of patients who had one BCC will develop another lesion within five years.
There are several clinical variants of BCC (nodular - the most common type of BCC and it can extend into ulcerative or cystic pattern, infiltrative, pigmented, morpheaform, superficial, fibroepithelioma of Pinkus). This article focuses on the infiltrative form. BCC is a slow-growing tumor, which rarely metastasizes and most often invades localy.


The treatment for BCC varies depending on the anatomic region and the histopathological features. Mohs micrographic surgery, destruction by various modalities, standard surgical excision and topical chemotherapy are the most common treatment options(1,2,3,4,5).
Clinical case
This paper bring in discussion the case of a 58-year-old patient who presented in our clinic with a protuberant formation at the internal left canthus having 2,3 cm in width and 3,5 cm in height, waxy surface, covered by telangiectases and central depression (3 mm in diameter). The tumor appeared 12 months ago as a small bump, with smooth surface, non-ulcerated and it had a small but constant growth achieving the present dimension. Taking in consideration its clinical features, the age, the sex and the region of the tumor, we guided our clinical diagnosis toward a basal cell carcinoma.
From his medical history, he denied any relevant pathological condition. He is non-smoker and he doesn’t drink alcohol.
An MRI was performed to determine the depth and how the surrounding tissues were infiltrated. The result showed a formation of 35/30/23 mm, well shaped, having ulceration and necrotic areas. It is situated in close relation to the left nasal bone that present thinning due to the pressure atrophy. It does not exceed the orbicularis oculi muscle fascia, it is not penetrating the intraorbital fat and the nasolacrimal duct is unaffected.
Blood test and the X-ray for the chest were normal.
A surgical plan was made to find the suitable technique for covering the large defect of the internal canthus if the left eye. There are numerous procedures available to reconstruct the defect, but it should be chosen in relation to the patient need and compliance.
The purpose of the reconstruction is to restore the normal function of the periocular region with good aesthetic appearance and to diminish the donor site morbidity.
We chose a technique used around 600-700 BC by Sushruta in India. The method was introduced in the 15th century in Europe and it became known as the Indian Flap or the median forehead flap. It is supplied and innervated by the supratrochlear vessels of the contralateral part.
We excised the tumor with safety margins of 3 mm and continued dissection into the deep tissues reaching the left nasal bone, from which we took some periosteum in order to determine the tumoral extension. During the surgery samples from the tumor were sent to the anatomopathologist to verify the clear limits of excision. The diagnostic was confirmed by this microscopic investigation, which revealed: baso-cellular carcinoma infiltrative form, with tumoral cell in the periosteum of the left nasal bone and clear margins.
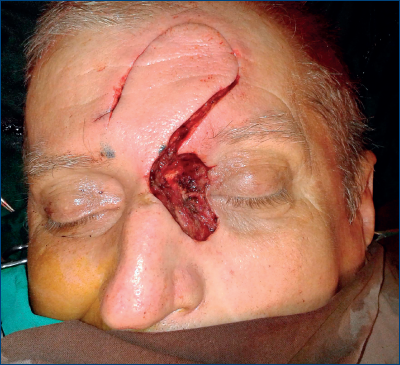
The defect created had to be covered by a good quality tissue because of the exposed bone. The pattern of the defect was used to mark the flap dimension and using a stretched out gauze we measured the flap length on the forehead. Gauze was rotated 180º to ensure adequate flap length. The pivot point was in the internal point of the right eyebrow. The superior end of the gauze was rotated over the forehead and the glabella to estimate the distance between the donor area and the area that need to be covered(6).


The flap is cut according to the markings, down to the underlying fascia. Dissection at the pivot point is done very carefully, not to damage the supratrochlear vessels. Hemostasis is performed in both areas, the recipient and the donor site. The flap is rotated 90 degree to internal canthus and the subcutaneous fat from flap is trimmed to have a better vacularization and a better aesthetic outcome. The donor area is covered by a full thickness skin graft taken from the proximal third of the internal left arm. Some buried stitches from an absorbable material are placed under the flap and in different canthal area to shape the new appearance. The skin is closed with 4-0 non-absorbable stitches. Dressing was made using antibiotic ointments along with i.v. medications (antibiotic, antiaggregants, NSAI and gastric protector).
The skin graft was covered by a tie-over wet gauze that was removed after 3 days.
The postoperative evolution was satisfactory and the patient was discharged at 7 days post-surgery. He was periodically checked-up to assess flap nourishment and possible complications that may arise in the donor area. The flap was reshaped after 3 weeks from surgery to obtain a more natural aspect.
The patient was sent to an oncologist for further investigation and treatment. He had no indication for radiotherapy or chemotherapy. At 12 months post-surgery he had a MRI for check-up that showed no relapses.

Discussion
BCC is a very common skin cancer that may become very aggressive, with destruction of the surrounding tissues and mutilation. Its surgical treatment is indicated due to its local invasion effects.
Its invasiveness lies also in the high risk of recurrence that can reach 40% at five years(4).
BCC is a tumor that is sensitive to radiotherapy and it may be used in patients with advanced and extended lesions, as well for lesion that could not be properly excised due to anatomical limits and failure of clear margins(7).
The risk of recurrence of tumors situated in areas like the periocular region is between 57-82%(8).
A study published in 1983 by Dubin and Kopf, regarding recurrence of BCC in 1417 patients, showed that overall five-year recurrence rates by therapy were 9.7% after X-ray therapy, 9,3% surgical excision(9).
The basal cell carcinoma presented histopathological as thin bundles of basaloid cells with nest-like configuration which can be found between the collagen fibers on the dermis and infiltrating in the depth. There can be hyperesthesia of the surrounding area on the face, due to the perineural infiltration(3).
Conclusion
Although eyelid cancer is rare, BCC represents more than 90% of the malignancies(10,11).
The most predilect area is the lower eyelid (48.9-72.1%), followed by the internal canthus (25-30%), upper eyelid (15%) and the lateral canthus (5%)(7).
BCC with dimension greater than or equal to 6 mm in diameter in high risk areas (e.g., central face, nose, lips, eyelids, eyebrows, periorbital skin, chin, mandible, ears, preauricular and postauricular areas, temples, hands, feet) has a high probability in recurrence(8).
The particularity of the case consists in the fact that the tumor is situated at the junction between the left side of the nose and the internal canthus of the left eye and it affected the periosteum of the nasal left bone. Clinically, the BCC had nodular appearance but after the histopathological examination it turned out to be an infiltrative form.
The dimension of the tumor required the use of a local rotated cutaneo-adipos flap from the median forehead, known as the Indian flap.
The margins of soft tissues excision were clear, but due to the risk of the nasal periosteum invasion, the patient was sent to oncology department for radiotherapy. He did not required oncological treatment and he is now periodically followed-up by the plastic surgery team.
Bibliografie
2. Charles Thorne, Scott Bartlett, Robert Beasley, Sherrell Aston, Geoffrey Gunter, Scott Spear - Dermatology for plastic surgeons, Grabb and Smith’s Plastic Surgery, Sixth Edition, LLW – 2006.
3. Lyubomi Dourmishev, Darena Rusinova, Ivan Botev- Clinical variants, stages, and management of basal cell carcinoma, Indian Dermatol Online J. 2013 Jan-Mar; 4(1): 12–17.
4.Peggy A Wu MD, Robert S Stern, June K Robinson MD, Rosamaria Corona - Epidemiology and clinical features of basal cell carcinoma (www.uptodate.com).
5. Robert S Bader, MD; William D James, MD - Basal Cell Carcinoma - Clinical Presentation, www.medscape.com..
6. A. M. Rotunda, MD, R. G. Bennett, MD, The bump Forehead Flap for Nasal Reconstruction: How We Do It, www.skintherapyletter.com.
7. Robert S Bader, MD, Andrew Scott Kennedy, MD, Andrew Scott Kennedy, MD, Laura Diomede, Basal Cell Carcinoma, www.medscape.com.
8. Sumaira Aasi, Timothy Chartier, Treatment of basal cell carcinomas at high risk for recurrence, Feb 19, 2014, www.uptodate.com.
9. Dubin N, Kopf AW, Multivariate risk score for recurrence of cutaneous basal cell carcinomas, Arch Dermatol. 1983; 119(5):373.
10. Eyelid Cancer: Statistics, Approved by the Cancer.Net Editorial Board, 08/2015, www.cancer.net
11. http://www.asoprs.org, EYELID TUMORS – basal cell carcinoma.