The Limberg flap – or “the amazing Limberg flap” – is an extremely versatile transposition flap based on random circulation. It is part of the cathegory of rhombic transposition flaps, initially described by Alexander A. Limberg in 1946 and published later on, in 1963. Ever since, it has been considered a veritable workhorse flap in the arsenal of the plastic surgeon because of the ease of its design, good aesthetic and functional results, and good applicability to almost any anatomical region and type of tissue. In recent years, the incidence of tumors has become increasingly high, especially in the case of skin cancer, thus making the surgical component an important one in the complex collaboration of the plastic surgeon with the oncologist. The present work is intended to present the versatility of the flap for different types and forms of defects, with an emphasis on oncologic pacients and tumors of several origins.
Flexibilitatea uimitorului lambou Limberg
The versatility of the amazing Limberg flap
First published: 27 martie 2019
Editorial Group: MEDICHUB MEDIA
DOI: 10.26416/OnHe.46.1.2019.2309
Abstract
Rezumat
Lamboul Limberg – sau „lamboul uimitor Limberg” – este un lambou de transpunere extrem de flexibil, bazat pe circulaţia aleatorie. Acesta este parte a categoriei de lambouri de transpunere rombică, descrisă iniţial de Alexander A. Limberg în 1946 şi publicată mai târziu, în 1963. De atunci, a fost considerat un adevărat lambou-miracol în arsenalul chirurgului plastic datorită simplităţii designului său, rezultatelor bune estetice şi funcţionale şi aplicabilităţii pentru aproape orice regiune anatomică şi tip de ţesut. În ultimii ani, incidenţa tumorilor a devenit din ce în ce mai mare, în special în cazul cancerului de piele, componenta chirurgicală având un rol important în colaborarea complexă a chirurgului plastic cu oncologul. Această lucrare are scopul de a evidenţia flexibilitatea lamboului pentru diferite tipuri şi forme de defecte, cu accent pe pacienţii oncologici şi tumorile de diferite origini.
Introduction
The Limberg flap – or “the amazing Limberg flap” – is an extremely versatile transposition flap based on random circulation. It is part of the category of rhombic transposition flaps, initially described by Alexander A. Limberg in 1946 and published later on, in 1963(1,2). Based on multiple models and applications, he described the initial flap as a rhombic transposition flap which had two internal angles: one of 1200 and the second of 600(1,3). Theoretically, having some limitations, other variants of the flap have been described, such as the Dufourmentel, Becker and Webster designs(4-6). The present work is intended to prove the versatility of the flap for different types and forms of defects (even composite ones), with an emphasis on oncologic patients and tumors of several origins.
Anatomy of the flap
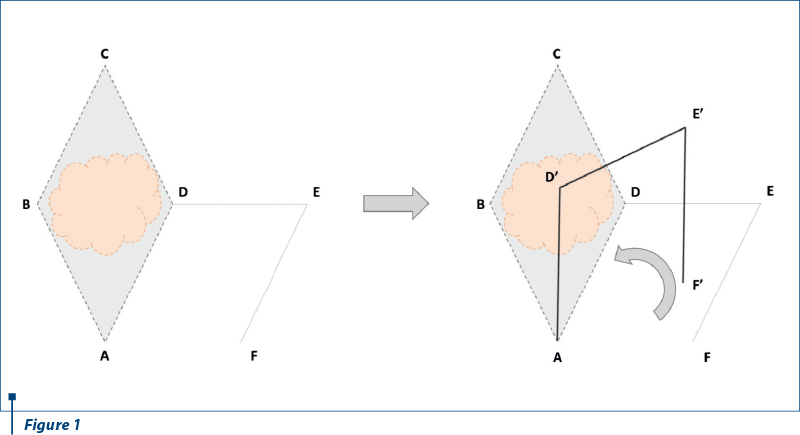
The Limberg flap is the classic rhombic transposition flap. It comprises two opposite equilateral triangles, placed base to base. In other words, it is a parallelogram with angles of 600 and 1200(7). All the sides of the rhombus are equal in length and also with its short diagonal(8).
The versatility of the Limberg flap also derives from the ease of its design. The parallelogram is drawn around the excision margin. For the first side of the flap, the short diagonal of the rhombic defect is extended towards any of the sides, with a length equal to the diagonal. The second line is drawn from the distal end of the first line and it is parallel and equal in length to one of the adjacent defect sides. There is a total of four flaps that can be created around the defect. This type of flap is best suitable for an elliptical lesion(7). After creating the defect, a wide undermining of the flap and the surrounding tissues, in the subdermal plane, should be carried, which recruits sufficient subcutaneous tissue with the elevated flap(2).
When closing the wound, the line of maximum tension is at the donor site (which should also be closed first). Therefore, for this purpose, it is advised to choose the area around the lesion that has the highest skin laxity(1).
Other variations of the rhombic transposition flap (with different angles) which should be noted are the Dufourmentel flap and the Webster flap(9).
Figure 1 depicts the layout of the Limberg flap. It is based on transposition, having a pivot point. When full closure is achieved, point D’ will be in the place of B, E’ in the place of C and F’ in the place of D.
Clinical application
Since its initial description, the Limberg flap has been widely used, being considered a veritable workhorse flap in the arsenal of the plastic surgeon. The arguments for this are multiple(1). It requires simple preoperative planning and measurements which promptly lead to good aesthetic and functional results. It provides predictable scarring if planned accordingly to the lines of maximal extensibility, relaxed tension lines (Langer) and to the aesthetic units and subunits with minimal tension or distortion of the surrounding structures(1).
Being extremely versatile, it can be applied to almost any anatomical region(2). If the defect is rhombic by nature, it may represent a perfect indication for a Limberg flap. If not, the defect may be tailored in such a manner. Our work is intended to prove that Limberg flap can be applied in any region or even employed a modified version of it to other tissues (i.e., muscle); the only consideration being that it uses local tissues and depends on the capacity of the tissue to extend, which makes it easy to use, perhaps with the exception of the scalp, where the skin and the galea are highly inextensible, thus being unable to recruit local tissue and closure of the donor defect may require a skin graft(10,11).
The incidence of tumors being increasingly high, especially in the case of skin cancer, the surgical component is an important one in the complex collaboration of the plastic surgeon with the oncologist. These patients being fragile and immunocompromised, it is of outmost importance to recruit the easiest and yet most efficient solution of margin-free excision, good cover of the defect, with the best postoperative result, low morbidity, low cost, and rapid time of surgery, the oncologic patient being considered a delicate one(12,13).
Discussion
The amazing Limberg flap is an extremely versatile one, easy to use, with low costs, low complications, high success rate and good patient satisfaction, being useful in many types of defects and pathologies, frequently proving a good covering measure in the delicate case of the oncologic patient.
Clinical case 1

Clinical case 2
Clinical case 3

Clinical case 4
Clinical case 5
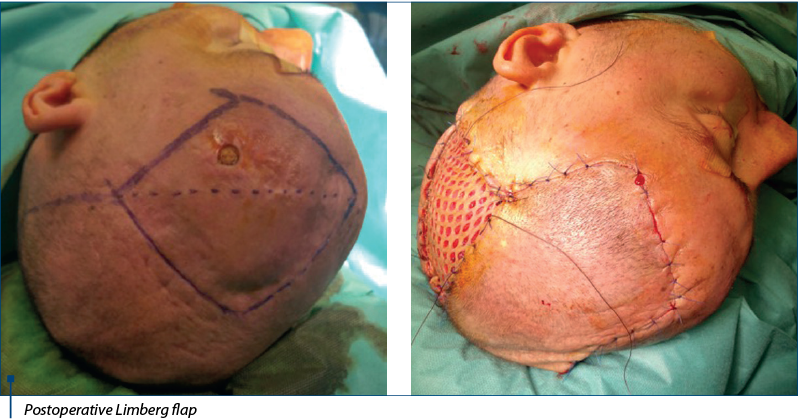
An important defect resulted after the excision of this tumor. Yet again, the Limberg flap was used. To be noted that here is one of the limitations of the flap, because in this specific anatomical region it cannot be closed primarily due to the lack of elasticity of the galea and of the skin. Consequently, the donor site must be closed by using a skin graft. This procedure involves bringing a flap to the zone of the resulting defect, while placing a skin graft in the less visible one.
Conflict of interests: The authors declare no conflict of interests.
Bibliografie
- Baker S. Rhombic Flaps, 3rd Ed. Local Flaps in Facial reconstruction. Sunders, 2014.
- Chasmar LR. The versatile rhomboid (Limberg) flap. Can J Plast Surg. 2007; 15(2):67-71.
- Limberg AA. Design of local flaps. In: Gibson T (editor). Modern trends in plastic surgery. Sevenoaks, England: Butterworth, 1966.
- Becker FF. Rhomboid flap in facial reconstruction. New concept of tension lines. Arch Otolarygol. 1979; 105:10.
- Dufourmentel C. An L-shaped flap for lozenge-shaped defects. In: Transactions of the Third International Congress of Plastic Surgery. Amsterdam: Excerpta Medica, 1964.
- Webster RC, Davidson TM, Smith RC. The 30-degree transposition flap. Laryngoscope. 1978; 88:85.
- Mathew J, Varghese S, Jagadeesh S. The Limberg Flap for Cutaneous Defects – a two-year experience. Indian J. Surg. 2007 Oct; 69:184–186.
- Limberg AA, Wolf SA. The Planning of Local Plastic Operations on the Body Surface: Theory and Practice, Lexington. MA/Toronto, Cullamore Press, 1984.
- https://emedicine.medscape.com/article/879923-treatment
- Aydin OE, Tan O, Algan S, Kuduban SD, Cinal H, Barin EZ. Versatile use of rhomboid flaps for closure of skin defects. Eurasian J Med. 2011; 43(1):1-8.
- Khan AAG, Shah KM. Versatility of Limberg flap in head and neck region. IJCRI. 2012; 3(6):13-18.
- Faenza M, Pieretti G, Lamberti R, et al. Limberg fasciocutaneous transposition flap for the coverage of an exposed hip implant in a patient affected by ewing sarcoma. Int J Surg Case Rep. 2017; 41:516-519.
- Blake BP, Simonetta CJ, Maher IA. Transposition Flaps: Principles and Locations. Dermatol Surg. 2015 Oct; 41 Suppl 10:S255-64.
Articole din ediţiile anterioare
Can we achieve successfully local control by IMRT radiotherapy in the treatment of male breast cancer? A case report
Această prezentare descrie un caz rar de cancer mamar la un pacient de gen masculin, patologie care are o incidenţă mai mică de 1% din toate cazur...
Breviar terapeutic al cancerului pulmonar fără celule mici, din perspectiva oncologiei medicale
Acest ghid sumarizează recomandările Societăţii Americane de Oncologie Clinică şi prezintă într-o manieră schematică principalele modalităţi de abo...
Oncologia geriatrică: principii şi perspective
Incidenţa şi prevalenţa cancerului la persoanele în vârstă sunt în creştere odată cu îmbătrânirea populaţiei.
Integrated Palliative Outcome Scale (iPOS) for the early detection of palliative care needs of cancer patients
În cadrul unui studiu prospectiv, a fost aplicat chestionarul iPOS la 103 pacienţi. Cu ajutorul întrebărilor la care au răspuns pacienţii, s-au i...