Objective. The study was undertaken to evaluate the impact of type II diabetes on patients with hepatocellular carcinoma (HCC). Material and methods. This is an observational study conducted in the Department of Oncology, Clinical Emergency County Hospital of Constanţa, for a period of four years, from 2010 to 2013. A total of 156 patients with HCC were analyzed. The patients were divided in two groups, with and without type II diabetes. Results. In this study, there were included 156 patients with hepatocellular carcinoma. Among all patients with HCC, 94 (60.3%) were male and 62 (39.7%) were female. Of the 156 patients with hepatocellular carcinoma, type II diabetes was found in 37 patients (23.7%). There is no difference between groups in relation to gender. The average age in the group of HCC was 70 years, compared to the group of diabetic patients in which the mean age was of 65.38 years with statistically significant difference. AFP levels were higher in the group of non-diabetic patients (AFP=4386.99 ng/ml) compared with the diabetic group (AFP=3329.12 ng/ml), but no statistically significant difference was found between groups (p>0.05). One-year mortality was higher in diabetic patients with significant difference between the two groups (p<0.05). Conclusion. Hepatocellular carcinoma is a common cancer, with increased incidence in our region, hepatitis C and B being shown to be the most frequent causative agent. Type 2 diabetes was present in 23.7% of cases. The average age at diagnosis of HCC within the group of diabetic patients was significantly lower. Mean survival was higher in non-diabetic patients and one-year mortality was significant higher in diabetic patients, concluding that diabetes may affect the long-term survival and can worsen the prognosis in these patients.
Impactul diabetului de tip 2 asupra prognosticului pacienților cu carcinom hepatocelular
The impact of type II diabetes on prognosis of patients with hepatocellular carcinoma
First published: 07 martie 2017
Editorial Group: MEDICHUB MEDIA
Abstract
Rezumat
Obiectiv. Studiul a fost făcut pentru a evalua impactul diabetului de tip II la pacienții diagnosticați cu carcinom hepatocelular (HCC).
Materiale și metode. Acesta este un studiu observațional desfățurat în Departamentul de Oncologie a Spitalului Județean de Urgență Constanța, cu o durată de patru ani, din 2010 până în 2013. Au fost analizați în studiu 156 de pacienți cu HCC. Pacienții au fost împărțiți în două grupuri, cu și fără diabet de tip II.
Rezultate. Din cei 156 de pacienți incluși în studiu, 94 (60,3%) au fost de sex masculin și 62 (39,7%) au fost de sex feminin. Din cei 156 pacienți, diabet de tip 2 a fost întâlnit la 37 de pacienți (23,7%).
Nu este nici o diferență între grupe în relație cu sexul pacienților. Vârsta medie a grupului fără diabet a fost de 70 de ani, iar la cei cu diabet 65,38 de ani, cu o diferență semnificativă statistic. Nivelul AFP a fost mai mare în grupul pacienților non-diabetici (AFP=4386,99 ng/ml) comparat cu grupul celor cu diabet (AFP=3329,12 ng/ml), dar fără diferențe semnificative statistic(p>0,05). Mortalitatea la un an a fost mai mare la pacienții diabetici, cu semnificație statistică (p<0,05). Concluzie. Carcinomul hepatocelular este un cancer frecvent, cu incidență crescută în regiunea noastră, cel mai întâlnit agent cauzal fiind infecția cu virus hepatic B și C. Diabetul zaharat a fost prezent în 23,7% din cazuri. Vârsta medie la diagnosticul HCC a fost semnificativ mai mică.
Supraviețuirea medie a fost mai mare la pacienții non-diabetici și mortalitatea la un an a fost semnificativ mai mare la pacienții diabetici, relevând că diabetul poate afecta supraviețuirea pe termen lung și că reprezintă un factor de prognostic negativ la acești pacienți.
Introduction
Hepatocellular carcinoma (HCC) is the 6th neoplasia as incidence and the third leading cause of cancer death in the world. Throughout the world, there are diagnosed each year approximately 630,000 new cases of HCC. Hepatocellular carcinoma mortality index reaches 94%(1).The most common and known risk factor are viral infection, hepatitis virus B or C, toxic factors - alcohol and aflatoxin, immune diseases like primary biliary cirrhosis, plus, in recent years, metabolic risk factors like diabetes and non-alcoholic hepatic steatosis(2,3).
A possible explanation for the association of diabetes with hepatocellular carcinoma is that diabetes is often part of the metabolic syndrome characterized by clinical and biochemical changes that include alterations in glucose metabolism and insulin, causing hyperglycemia and hyperinsulinemia, dyslipidemia and hypertension. Metabolic disorders associated with metabolic syndrome can cause diabetes and furthermore contribute to the development of NAFLD (non-alchoolic fatty liver disease) and its most severe form, non-alcoholic steatohepatitis, so HCC can result from liver cirrhosis caused by NAFLD(4,5,6). Type II diabetes has an increased incidence worldwide. Epidemiologically, the relationship between HCV infection and diabetes is known, diabetes being reported to increase the risk of hepatocellular carcinoma in patients with chronic hepatitic C and also contributes to the excess mortality in this patients(7,8).
Management of hepatocellular carcinoma is influenced by tumor status, liver function and by comorbidities, and diabetes is one of them(9,10).
Material and methods
This is an observational study conducted in the Department of Oncology, Clinical Emergency County Hospital of Constanţa, for a period of four years, from 2010 to 2013. One hundred and sixty-five patients diagnosed with hepatocellular carcinoma were included in this study.Patients were divided in two groups regarding the presence or absence of type II diabetes. Demographic profile, clinical features, etiology, tumor size, and presence of portal vein thrombosis were compared between groups. Biological parameters were determined, including AST, ALT, total bilirubin, albumin, INR, AFP.
Data were evaluated using the statistical program SPSS 21.0. Qualitative data included descriptive statistics, continuous variables are expressed as Mean and Standard Deviation, and T test was used to compare the two groups. P value <0.05 was considered statistically significant.
Results
In this study, there were included 156 patients with hepatocellular carcinoma. Demographic data are shown in Table 1.Among all patients with HCC, 94 (60.3%) were male and 62 (39.7%) were female. Mean age was 64.39 years for males and 69.53 years for female.
The etiology of HCC was in higher percentage for HCV: 51 (32.70%), and HBV: 34 (21.80%), alcohol etiology was present in 23 cases (14.70%) and in 48 cases the etiology of HCC was unknown. Cirrhosis was present in 94 patients and absent in 62. Among patients with hepatic cirrhosis, the higher percentage was class Child-Pugh B: 39 (41.49%), followed by class C with 30 cases (31.91%) and class A with 25 cases (26.60%).
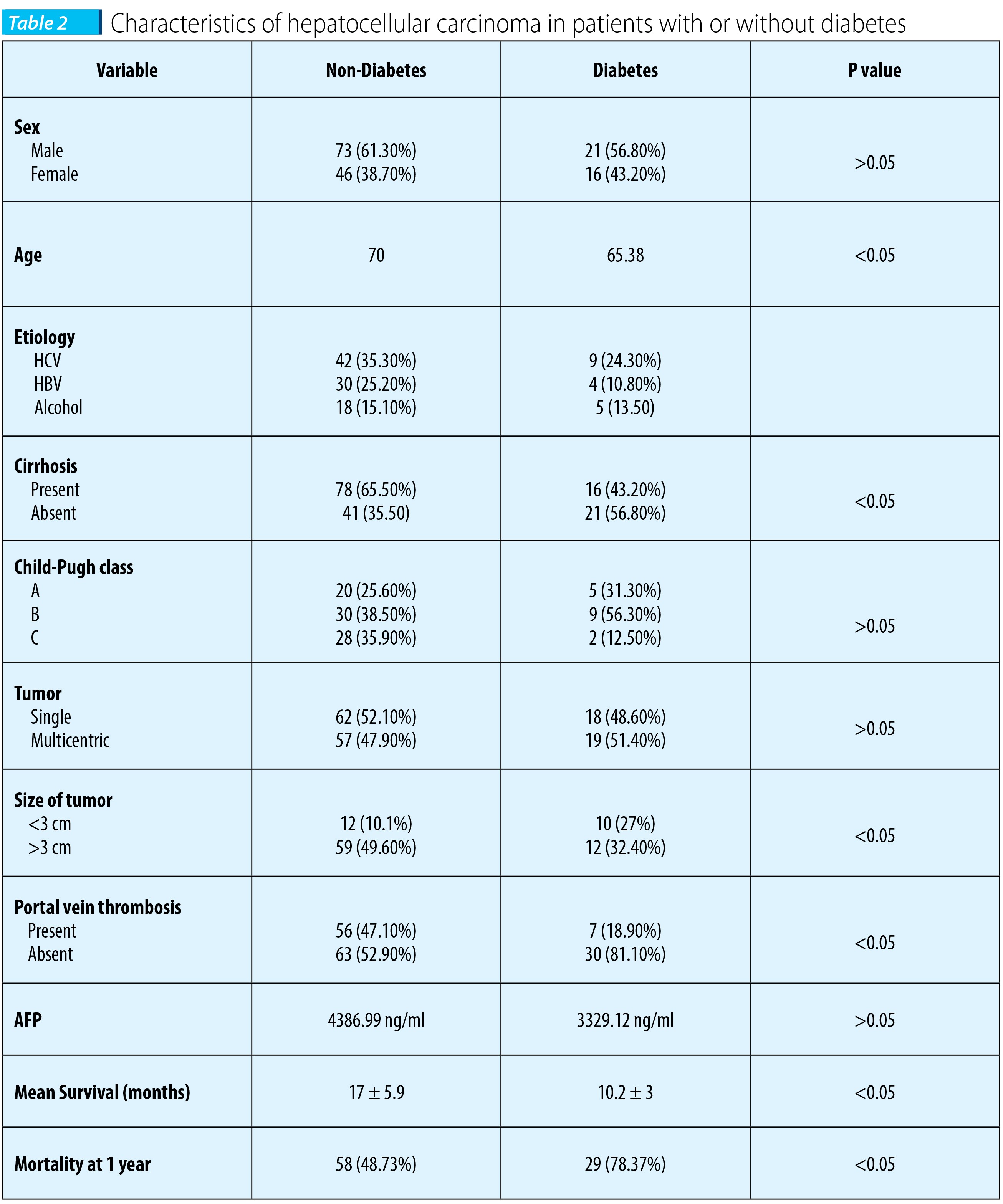
Of the 156 patients with hepatocellular carcinoma, type II diabetes was found in 37 patients (23.7%). In table 2, there are shown the clinical features at the time of diagnosis of hepatocellular carcinoma with or without type II diabetes. There is no difference between groups in relation to gender. The average age in the group of HCC was 70 years, compared to the group of diabetic patients in which the mean age was of 65.38 years, with statistically significant difference.
Regarding liver cirrhosis, in the non-diabetic group it was present in a higher percentage compared with the group of diabetic patients, 78 cases (65.5%), and respectively 16 cases (43.2%), with statistical significance. Comparing the two groups with respect to Child-Pugh class, we did not find any significant differences (p>0.05). Comparing the two groups based on the size of liver tumors, there is a statistically significant difference (p<0.05).
Portal vein thrombosis is present in the group of non-diabetic patients in a percentage of 47.1% compared with the group of diabetic patients, in which portal vein thrombosis was present in 18.9% of the cases (p<0.05).
AFP levels were higher in the group of non-diabetic patients (AFP=4386.99 ng/ml) compared with the diabetic group (AFP=3,329.12 ng/ml), but no statistically significant difference was found between the groups (p>0.05).
One-year mortality was higher in diabetic patients, with significant difference between the two groups (p<0.05).
Conclusions
Hepatocellular carcinoma is a common cancer, with an increased incidence in our region, hepatitis C and B being shown to be the most frequent causative agent.Type II diabetes was present in 23.7% of cases, a percentage which falls within the data from literature, showing an incidence of diabetes between 15.8% and 43.3%. The average age at diagnosis of HCC within the group of diabetic patients was significantly lower (p<0.05) compared with the average age of the group of non-diabetic patients.
Liver cirrhosis is one of the most important risk factors for HCC development - 94 cases from both groups of patients had cirrhosis at the diagnosis of HCC, and of these, type II diabetes was present in 16 cases, which shows that HCC in patients with type II diabetes can occur in the absence of cirrhosis (p<0.05). The analysis of groups according to tumor appearance showed a higher percentage of multicentric tumors in diabetic patients, without statistical significance (p>0.05). The analysis according to liver tumor size showed statistically significant difference between groups (p<0.05) - in non-diabetic patients, there were observed more advanced HCC.
The average values of AFP were higher in the group of non-diabetic patients compared with the diabetic group, but no statistically significant difference was found between groups (p>0.05).
Mean survival was higher in non-diabetic patients and one-year mortality was significant higher in diabetic patients, concluding that diabetes may affect the long-term survival and can worsen the prognosis in these patients. n
Bibliografie
2. Davila JA, Morgan RO, Shaib Y, McGlynn KA, El-Serag HB. Diabetes increases the risk of hepatocellular carcinoma in the United States: a population based case control study. Gut, 2005; 54: 533-539.
3. El-Serag HB, Tran T, Everhart JE. Diabetes increases the risk of chronic liver disease and hepatocellular carcinoma. Gastroenterology, 2004; 126: 460-468.
4. Chuang SC, Vecchia CL, Boffetta P. Liver cancer: Descriptive epidemiology and risk factors other than HBV and HCV infection. Cancer Lett, 2008, 15.
5. Caronia S, Taylor K, Pagliaro L, Carr C, Palazzo U, Petrik J, et al. Further evidence for an association between non-insulindependent diabetes mellitus and chronic hepatitis C virus infection. Hepatology, 1999; (4): 1059-63.
6. Rathmann W, Giani G. Global prevalence of diabetes: estimates for the year 2000 and projections for 2030. Diabetes Care, 2004; (5): 1047-53.
7. Nasir Khokhar. Association of chronic hepatitis C virus infection and diabetes mellitus. Pak J Med Res, 2002; 41(4): 155-8.
8. Adami HO, Chow WH, Nyrén O, Berne C, Linet MS, Ekbom A, et al. Excess risk of primary liver cancer in patients with diabetes mellitus. J Natl Cancer Inst, 1996; (20): 1472-7.
9. Toyoda H, Kumada T, Nakano S, Takeda I, Sugiyama K, Kiriyama S, Tanikawa M, Sone Y, Hisanaga Y. Impact of diabetes mellitus on the prognosis of patients with hepatocellular carcinoma. Cancer, 2001; (5): 957-63.
10. Di Costanzo GG, De Luca M, Tritto G, Lampasi F, Addario L, et al. Effect of alcohol, cigarette smoking, and diabetes on occurrence of hepatocellular carcinoma in patients with transfusion-acquired hepatitis C virus infection who develop cirrhosis. Eur J Gastroenterol Hepatol, 2008; 20: 674-679.