Pain is a complex symptom, with implications regarding biological, psychological,social and spiritual factors (the concept of Total Pain). Bone metastasis are constant presence in the evolution of numerous cancers, sometimes affecting over 50% of patients(breast, prostate cancer). The presence of the primary bone tumour or of the bone metastasis is associated with skeletal related events (SREs) - pathologic fracture, spinal cord compression, necessity for surgery or radiation to bone (for pain or impending fracture). This last indication is the subject of this study. In this article there are investigated descriptive and observational studies which present information regardin the role and importance of radiotherapy, with or without radioisotopes, in controlling pain of patiens with primary bone cancer or bone metastasis. A special attention is offered to Quality of Life(QOL) of these patients. (Because of economic reasons, we used only free acess data bases.)
Rolul radioterapiei în controlul durerii la pacienții cu cancer osos/metastaze osoase
The role of radiotherapy in controlling pain in patients with bone cancer/bone metastasis
First published: 07 martie 2017
Editorial Group: MEDICHUB MEDIA
Abstract
Rezumat
Durerea este un fenomen complex, cu implicații profunde de ordin biologic, psihologic, social și spiritual (conceptul de „durere totală”). Metastazele osoase sunt o prezență constantă în evoluția a numeroase neoplazii, uneori afectând peste 50% din pacienți (cancer de sân, prostată). Prezența tumorii primare osoase sau a metastazelor este asociată cu riscul de evenimente legate de schelet (skeletal related events) - fractură pe os patologic, compresie vertebrală, necesitatea intervenției chirurgicale și necesitatea radioterapiei (pentru ameliorarea durerii și iminența fracturii). Această ultimă indicație face obiectul studiului prezent. În acest articol sunt investigate studii de tip descriptiv și observațional care prezintă informații legate de rolul și importanța radioterapiei, cu sau fără radioizotopi, în controlul durerii pacienților cu cancer primar de os sau metastaze osoase. Este acordată o atenție deosebită calității vieții acestor pacienți. (Din cauza rațiunilor de ordin economic, am folosit doar bazele de date cu acces liber.)
The concept of “total pain” comprises all the factors that produce pain: biological factors (physical), psychological factors (mental, emotional, behavioural), social factors (the relation with other people) and spiritual factors.
Pain is one of the most feared symptoms in cancer patients. The Oncologic Radiotherapy Group reported that most doctors think that pain is an undertreated symptom in cancer patients from various reasons: inadequate pain assessment, under-reported pain by patients, fear of opioid addiction, and other social and legal issues(10).
Many cancer patients have metastases at the time of diagnosis or will present metastases in the course of the disease. When curative treatment is impossible, the therapy must focus on maintaining the quality of life(1).
American Pain Society (APS) provided well-documentated guides for pain management in cancer patients. Most guides were focused on the pharmacological treatment of neoplastic pain, represented by nonsteroidal anti-inflamatory drugs, opioids and anticonvulsants. Palliative radiotherapy as a pain treatment measure in cancer patients is briefly mentioned in these guides. The recent recommendations of American Pain Society underlined the importance of a multimodal approach to the treatment of pain in oncologic patients(10).
Bone metastases are a frequent complication of cancer, found in half of the oncologic patients who died. Breast cancer and prostate cancer are the most frequent types that present bone metastases, with an incidence of 75%, respectively 68%(7).
The palliative approach of pain in patients with bone metastases is of major importance in the clinical management of advanced-staged cancer(4).
Up to 70% of bone metastases are localized at the spine cord level. Spinal metastases can cause pain, which most often progresses in time, leading to a decrease in the quality of life. Conventional radiotherapy was used along the years in palliation for treating pain caused by bone metastases. It was observed that a decrease in the intensity of pain would be achieved in 2/3 of the radio-treated patients after 4-6 weeks of irradiation, and the reirradiation will be necessary in approximately 24% of cases(1).
Palliative radiotherapy for painful bone metastases was intensively studied, proving that is effective, relieving pain in about 90% of cases. External radiation therapy is the standard of care in patients with bone metastases, and studies show that the use of radiopharmaceuticals, like Sr89, is beneficial in pain management(10).
The indications of radiotherapy in spinal metastases are: pain, reducing the risk of fracture, nerve compression, and preventing local recurrences. Management of spinal hemangiomas and osteolytic metastases at the cervical spine is a real clinical challenge. In this case, the role of radiotherapy is palliative: controlling pain, stabilization of the spinal cord, improving or maintaining the neurological function, and obtaining the local control of cancer(6).
A major problem that doctors are confronted with is the treatment of refractory bone pain from advanced cancer. It was revealed that two types of cancer - breast cancer and prostate cancer - metastasize to bone in approximately half of the cases, therefore pain relief and improving the mobility are the main goals, in some cases being the only objective of management in those patients. Radiotherapy proved to be efficient in patients with bone-localized cancer, and also in cases where the objectives were the treatment of imminent fractures and of spinal cord compression. In case of bone metastases, which most often have multiple localizations, a systemic treatment to reduce pain is needed, thus radioactive medication treatment with 32P and 89 Sr is a therapeutic possibility(9).
Palliative radiotherapy in painful osteolytic processes is an important component of the multiple myeloma treatment, different doses of radiation being used for this purpose(8).
Palliative radiotherapy represents a stable instrument in the management of symptoms caused by cancer, being efficient in the treatment of locally advanced cancer and of metastatic cancer, whith symptoms as pain, hemorrhage or obstruction. Nevertheless, most data on palliative radiotherapy are those regarding its utilization in the treatment of painful bone metastases(10).
Bone metastases are frequent in patients with breast or prostate cancer, causing pain and other conditions, such as hypercalcemia, pathological fractures and spinal cord compression(2).
Bone is the most frequent and potentially debilitating localization of prostate cancer metastases. When bone metastases are present at the initial diagnosis, palliative radiotherapy associated with androgen ablation seldom lead to the remission of the disease. Along with the proliferation of an androgen-independent tumor, bone metastases can lead to pain, spinal cord impairment, with loss of function and hematopoietic reserve deterioration. In this situation, palliation is the only goal, because no other approach demonstrated life-prolongation. For a patient with painful lesions, the external beam radiation is the most effective and durable treatment for pain alleviation(5).
The metastatic impairment of the skeleton is common in breast cancer patients. Pain is an important symptom caused by these metastases. The standard therapy for bone metastases is external radiotherapy, often associated with the administration of radioisotopes(3).
Internal therapy with radioisotopes, focused on the affected bony areas, is used for pain controlling and improving the quality of life as an alternative to conventional therapies(4).
Purpose
To investigate the importance of radiotherapy, with or without radioisotopes, in the management of pain in patients with bone cancer or bone metastases.
Inclusion criteria for revision studies
Types of studies:
For this revision, we searched and considered eligible descriptive studies and observational analytical studies that presented information on the role and importance of radiotherapy, with or without radioisotopes, in controlling pain in patients with bone cancer or bone metastases.
Types of participants:
In this revision, we included studies in which patients were adults or children, regardless of their gender, race and age, who were diagnosed with bone cancer or bone metastases and experienced pain, whatever the intensity, and who benefited from palliative radiotherapy as a treatment method.
Types of interventions:
We considered for revision all the studies on patients diagnosed with bone cancer or bone metastases, who experienced pain, for which they underwent palliative radiotherapy. There were included studies in which radiotherapy was administered with or without radioisotopes, without considering the number of the treated areas, the irradiated surface, the radiation dose, the irradiation time, and the number of sessions. We also included studies in which patients with neoplastic bone lessions who were radiotreated experienced pain regardless of the intensity, painfull area(s), number and types of pain, pathways and the characteristic of pain(1-19).
Types of followed indicators
There were observed the following indicators:
- the type of pain
- the initial intensity of pain
- the intensity of pain after radiotherapy
- the irradiation dose used
- whether radioisotopes were used.
Where possible, there were also observed:
- the number of painful areas
- the duration of irradiation
- the number of radiation therapy sessions
- the adverse reactions of radiotherapy
- the quality of life after radiation.
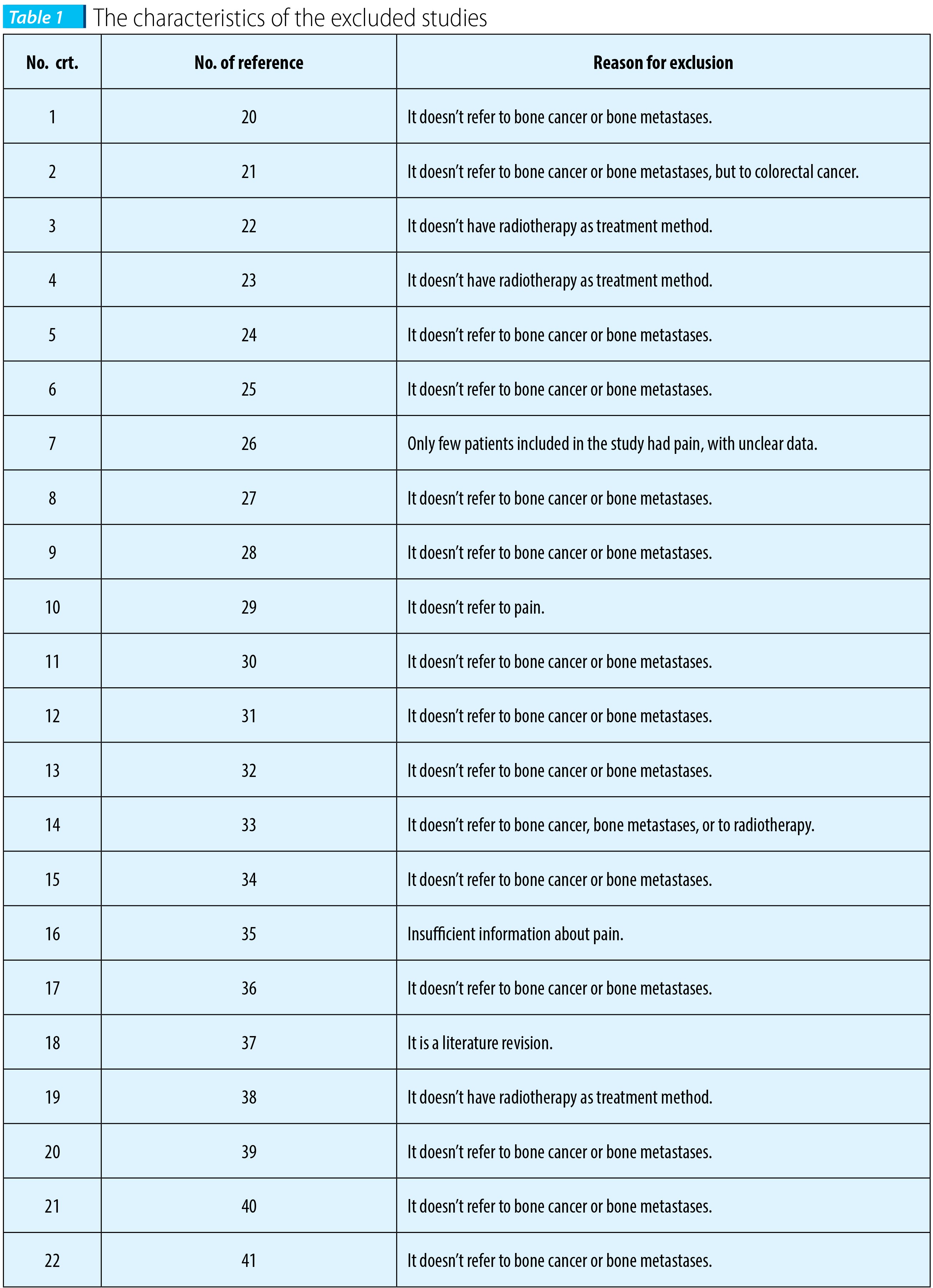
Exclusion criteria for revision studies:
- studies that don’t correspond to the inclusion criteria
- studies in which radiotherapy was administered for other types of cancer than bone cancer or bone metastases
- studies in which radiotherapy wasn’t administered for the treatment of pain
- studies in which the treatment of pain didn’t involve radiotherapy(20-41).
Search strategy for finding studies:
We looked for studies in the following electronic databases:
- PubMed
- Medscape
- Cochrane Library.
Because some electronic databases require subscription or can only be accessed for purchase using a password, the revision studies were searched for exclusively in databases with free access.
The search strategy was realized for PubMed, being adapted according to the requirements of other databases.
In the search strategy, we used both words or text, and MeSH terms:
- bone cancer pain
- bone cancer radiotherapy/radiation
- bone metastasis pain
- bone metastasis radiotherapy/radiation
- cancer radiotherapy/radiation
- oncology radiotherapy/radiation
- oncology treatment bone cancer
- oncology treatment bone metastasis
- pain radiotherapy/radiation
- pain relief
- pain treatment
- pain therapy
- palliative care
- palliative radiotherapy
- palliative therapy
- palliative treatment
- radiation
- radiotherapy painful bone metastases
- radiotherapy
- total pain.
The studies we considered relevant were searched for in their publication language or in English. Besides the studies we searched using the aforementioned strategy, different literature revisions and studies that partially referred to the subject were looked for as supplimentary studies for our revision.
Methods of revision
Selection of studies
After the searching phase, the abstracts of studies we had found were evaluated using the inclusion criteria already established. In case we couldn’t establish according to the abstract if the study can be included, we tried to obtain the whole article.
Data extraction from studies
For data extraction, a simple electronic data sheet was used, in which we looked for the following information:
- the study design
- the duration of the study
- the number of patients
- the inclusion criteria
- the initial intensity of pain
- the intensity of pain after radiotherapy.
Data analysis
For data analysis, we developed a quantitative synthesis to evaluate the initial pain, and the pain after radiotherapy. Because the quantitative synthesis couldn’t be done (prospective and retrospective heterogeneous studies, case studies, the lack of randomized trials, different methodologies used, the administration of medication without clearly specifing whether it was simultaneous with radiotherapy, uncertainties regarding the inclusion of patients in studies), a descriptive synthesis of the included studies was done.
Assessing the quality of the studies
Each study which satisfied the inclusion criteria was qualitatively evaluated according to the design proposed in the evaluation datasheet, in order to obtain the minimum quality standard. The search strategy didn’t take into consideration those studies whose abstract provided valuable but only partial information for our revision because in extenso articles couldn’t be freely accessed.
Description of the studies
According to our search strategy, there were highlighted 37 studies, out of which:
- 10 prospective studies
- 11 retrospective studies
- 8 clinical randomized trials
- 2 literature revisions
- 3 case studies
- 1 multicentric study
- 2 review articles on the subject.
Twenty-two studies were excluded from our revision, with reasons presented in Table 1.
Fifteen studies were included in our revision, the information obtained being presented in the Results section.
Results
The studies included in our revision revealed the following:
- 5 studies were retrospective
- 10 studies were prospective
- 4 studies were clinical randomized trials
- one study was multicentric prospective randomized
- one study compared the conventional radiotherapy with stereotatic radiotherapy in controlling pain
- two studies compared the administration of one radiotherapy session with the administration of multiple radiotherapy sessions in controlling pain
- in 7 studies there were used different radioisotopes for controlling pain, while simple radiotherapy was used in 8 studies
- in 4 studies, Rhenium 186 was the most frequently radioisotope used for controlling pain
- 14 studies recorded a good control of the pain after radiotherapy
- 3 studies mentioned toxicity at high levels of radiation
- in one study, the selected patients had multiple myeloma
- in one study, the selected patients had bone cancer
- in 13 studies, the selected patients had bone metastases
- in 4 studies, the radiaton dose was between 8 Gy and 30 Gy
- in 2 studies, high doses of radiation were used
- 3 studies recorded a good control of the pain at one month after treatment
- aside from controlling pain, 3 studies also evaluated the costs of radiotherapy
- one study revealed the increase of bone recalcification.
Discussions
This literature revision tried to bring evidence on the administration of radiotherapy in patients with bone cancer or bone metastases who experience pain.
Due to the need for economic resources in order to have access to most databases, this literature revision contains only partial data on the subject, as we only used free online databases.
According to the information drawn by studies included in our revision, the administration of a single radiotherapy session seems to have similar effects on pain as more sessions of radiotherapy. For this reason, one session is to be preferred, and it’s also associated with fewer and lower adverse reactions.
The use of radioisotopes compared to conventional radiotherapy doesn’t seem to have more benefits in controlling pain in patients with bone cancer or bone metastases.
Conclusions
Radiotherapy provides a good control of pain in patients with bone cancer or bone metastases.
High doses of radiation are associated with major toxicity, therefore is preferred the administration of low doses.
The use of radioisotopes doesn’t bring extra benefits in controlling pain, compared to simple radiotherapy.
Pain control is assured for a period up to several months since the last dose of radiations. n
Bibliografie
2. Chow et al. Confirmatory factor analysis of brief pain inventory (BPI) functional interference clusters in patients with bone metastases. J Pain Manag 2010; 3(3): 247–253(63).
3. de Kierk et al. Pharmacokinetics of Rhenium- 186 After Administration of Rhenium- 186-HEDP to Patients with Bone Metastases. The Journal of Nuclear Medicine 1992; 3(5)(32).
4. Giammarile et al. Bone Pain Palliation with 85Sr Therapy. The Journal of Nuclear Medicine 1999; 40:4.(28).
5. Graham et al. Rhenium-186-labeled Hydroxyethylidene Diphosphonate Dosimetry and Dosing Guidelines for the Palliation of Skeletal Metastases from Androgen-independent Prostate Cancer. Clinical Cancer Research 1999; 5: 1307–1318(31).
6. Guo et al. CT-Guided Percutaneous Vertebroplasty of the Upper Cervical Spine via a Translateral Approach. Pain Physician 2012; 15:E733-E741(3).
7. Li et al. A multidisciplinary bone metastases clinic at Toronto Sunnybrook Regional Cancer Centre – A review of the experience from 1999 to 2005. Journal of Pain Research 2008:1 43–48(43).
8. Matuschek et al. Effects of Radiotheraphy in the treatment of multiple myeloma: a retrospective analysis of a single institution. Radiation Oncology 2015: 10: 71(12).
9. Narendra Nair. Relative Efficacy of 32P and 89Sr in Palliation in Skeletal Metastases. The Journal of Nuclear Medicine 1999; 40: 256-261(40).
10. Sun et al. Palliative Radiation Therapy of Symptomatic Recurrent Bladder Cancer. Pain Physician 2007; 10: 285-290(1).
11. Kapoor et al. Analysis of Patterns of Palliative Radiotherapy in North West India: A Regional Cancer Center Experience. Indian J Palliat Care. 2015; 21(2): 168–173.
12. Eisenhut et al. Iodine-131-Labeled Diphosphonates for Palliative Treatmentof Bone Metastases: II. Preliminary Clinical Results with Iodine- 131 BDP3. The Journal of Nuclear Medicine 1986; 27: 1255-1261.
13. Klerk et al. Pharmacokinetics of Rhenium- 186 after Administration of Rhenium- 186-HEDP to Patients with Bone Metastases. The Journal of Nuclear Medicine 1992; 33: 646-651.
14. Needham et al. Radiotherapy for bone pain. J Royal Soc Med 194; 87.
15. van den Hout et al. Single- versus Multiple-Fraction Radiotherapy in Patients With Painful Bone Metastases: Cost–Utility Analysis Based on a Randomized Trial. Journal of the National Cancer Institute 2003; 95(3).
16. Han et al. The Placorhen Study: A Double-Blind, Placebo Controlled, Randomized Radionuclide Study with 186Re-Etidronate in Hormone-Resistant Prostate Cancer Patients with Painful Bone Metastases. J Nucl Med 2002; 43:1150–1156.
17. Minutoli et al. 186 Re-HEDP in the palliation of painful bone metastases from cancers other than porstate and breast. Q J Nucl Med Mol Imaging 2006; 50: 355-362.
18. Andrade et al. A simple and effective daily pain management method for patients receiving radiation therapy for painful bone metastases. Int J Radiat Oncol Biol Phys. 2010; 78(3): 855–859.
19. Dmajumder et al. Single Fraction versus Multiple Fraction Radiotherapy for Palliation of Painful Vertebral Bone Metastases: A Prospective Study Indian J Palliat Care. 2012; 18(3): 202–206.
20. Yi et al. Palliative Radiation Therapy of Symptomatic Recurrent Bladder Cancer. Pain Physician 2007; 10:285-290.
21. Bae et al. Palliative radiotherapy in patients with a symptomatic pelvic mass of metastatic colorectal cancer. Radiation Oncology 2011, 6:52.
22. Guo et al. CT-Guided Percutaneous Vertebroplasty of the Upper Cervical Spine via a Translateral Approach. Pain Physician 2012; 15:E733-E741.
23. Athwal et al. Coonrad-Morrey total elbow arthroplasty for tumours of the distal humerus and elbow. J Bone Joint Surg [Br] 2005; 87-B:1369-1374.
24. Edyta et L. Whole Liver Palliative Radiotherapy for Patients with Massive Liver Metastases. Asian Pac J Cancer Prev 2015; 16 (15), 6381-6384.
25. Juffermans et al. Reirradiation and Hyperthermia in Rectal Carcinoma. A Retrospective Study on Palliative Effect. Cancer 2003; 98(8).
26. Jensen et al. Incidence of bone metastases and skeletal-related events in breast cancer patients: A population based cohort study in Denmark. Cancer 2011, 11:29.
27. Allen et al. Effective bone palliation as related to various treatment regimens. Cancer 37:984-987, 1976.
28. Soffen et al. Palliative Radiotherapy for Symptomatic Adrenal Metastases. Cancer 65:1318-1320, 1990.
29. Wagner et al. Splenic Irradiation in the Treatment of Patients with Chronic Myelogenous Leukemia or Myelofibrosis with Myeloid Metaplasia. Results of Daily and Intermittent Fractionation with and without Concomitant Hydroxyurea. Cancer 58:1204-1207, 1986.
30. Rubin et al. Systemic Hemibody Irradiation for Overt and Occult Metastases. Cancer 552210-222 I, 1985.
31. Reddy et al. The Role of Radiation Therapy in the Palliation of Metastatic Genitourinary Tract Carcinomas. A Study of the Radiation Therapy Oncology Group. Cancer 52:25-29, 1983.
32. Corn et al. Recurrent Ovarian Cancer Effective Radiotherapeutic Palliation after Chemotherapy Failure. Cancer 1994; 742979-83.
33. Gebhardt et al. Implanted Intrathecal Drug Delivery Systems and Radiation Treatment. Pain Medicine 2013; 14: 398–402.
34. Ma et al. Meta-analysis comparing higher and lower dose radiotherapy for palliation in locally advanced lung cancer. Cancer Sci 105 (2014) 1015–1022.
35. Biersack et al. Palliation and Survival after Repeated 188Re-HEDP Therapy of Hormone-Refractory Bone Metastases of Prostate Cancer: A Retrospective Analysis. J Nucl Med 2011; 52:1721–1726.
36. Plataniotis et al. Palliative Hypofractionated Radiotherapy for Non-Small-Cell Lung Cancer (NSCLC) Patients Previously Treated by Induction Chemotherapy. J Thorac Dis 2009; 1: 5-10.
37. McDonald et al. Quality of life after palliative radiotherapy in bone metastases: A literature review. Journal of Bone Oncology 4 (2015) 24–31.
38. Galvez et al. Analgesic efficacy of zoledronic acid and its effect on functional status of prostate cancer patients with metastasis. Patient Preference and Adherence 2008: 2 215–224.
39. Kumar et al. Radiation Induced Oral Mucositis. Indian J Palliat Care. 2009; 15 (2): 95–102.
40. Kim et al. Short-course palliative radiotherapy for uterine cervical cancer. Radiat Oncol J 2013; 31(4):216-221.
41. Yamashita et al. Symptom relief effect of palliative high dose rate intracavitary radiotherapy for advanced esophageal cancer with dysphagia. Oncology letters 9: 1747-1752, 2015.