One of the major points of interest yet unclarified in radiotherapy refers to choosing the optimal irradiation technique in breast cancer cases. The purpose of this retrospective study is to determine the optimal irradiation technique in breast cancer irradiation, applicable in most clinical cases, depending on the organ at risk which requires the highest level of protection. We start from the premises that 3D conformational technique remains the standard technique used in breast cancer irradiation, especially in cases that do not benefit from respiratory gating or breath hold system. The aim of this study is to implement a clinical protocol which, depending on planning target volume (PTV) location and size, might predict whether dose limits in organs at risk shall be complied with medical guides (RTOG, Quantec etc.), especially in cases where stricter limitations are intended than such specified in this guides by using 3D conformational technique or a better result would be obtained in case of using the IMRT technique.
Studiu retrospectiv în iradierea cancerului mamar
A retrospective dosimetrical study in breast irradiation
First published: 27 octombrie 2017
Editorial Group: MEDICHUB MEDIA
DOI: 10.26416/OnHe.40.3.2017.1156
Abstract
Rezumat
Una dintre problemele de interes major încă neclarificate în radioterapie se referă la alegerea optimă a tehnicii de iradiere a neoplasmului mamar. Acest studiu retrospectiv are scopul de a determina tehnica optimă de iradiere, aplicabilă în majoritatea cazurilor clinice în funcție de organul la risc critic pentru fiecare situație în parte. Se pornește de la premisa că tehnica 3D conformațională rămâne tehnica standard utilizată în iradierea neoplasmului mamar, în special în cazurile în care nu se beneficiază de sisteme de monitorizare a respirației. Se urmărește realizarea unui protocol clinic cu ajutorul căruia, în funcție de localizarea și dimensiunea volumului-țintă planificat (PTV), să se poată prezice dacă se vor respecta limitele de doză în organele la risc, în special pentru cazurile în care sunt urmărite constrângeri mai stricte decât cele specificate în ghidurile medicale (RTOG, Quantec, ş.a.) utilizând tehnica 3D conformațională sau rezultatul ar fi îmbunătățit utilizând tehnica IMRT.
Introduction
Together with the global technological development, various targeted irradiation techniques have emerged, which enable the supply of a lower dose to healthy organs. This study refers strictly to external X-ray radiotherapy and intends to weigh up the 3D conformational technique versus IMRT technique. The IMRT technique gives the possibility to modulate beam intensity, providing a dose distribution as homogenous as possible and simultaneously avoids the supply of a high dose to healthy tissues in the immediate vicinity of the target volume to be irradiated.Nevertheless, the 3D conformational technique remains a standard breast cancer irradiation technique for several reasons. Firstly, modulated intensity techniques provide the possibility of a far more precise irradiation than conformational techniques and they face the problem regarding patient’s respiratory movement, under the conditions in which a respiratory control system of the patient is not provided, such as breath hold or respiratory gating(2).
A second issue encountered refers to the discussion related to delayed toxicity caused by low radiation doses in large healthy tissue volume(3). Comparative studies have outlined that by using the 3D conformational technique, healthy tissues near the planning target volume (PTV) collect high doses in a small volume, and by using the modulated intensity technique one can avoid the supply of a large dose of radiation in health tissues(4). One disadvantage of the IMRT technique regarding organs at risk is given by the increase of the median dose due to the supply of a small dose in a large part of the healthy volume(5). Up until now, it has been certified that the supply of a small dose in a large volume of healthy tissue may be negligible on long term survival.
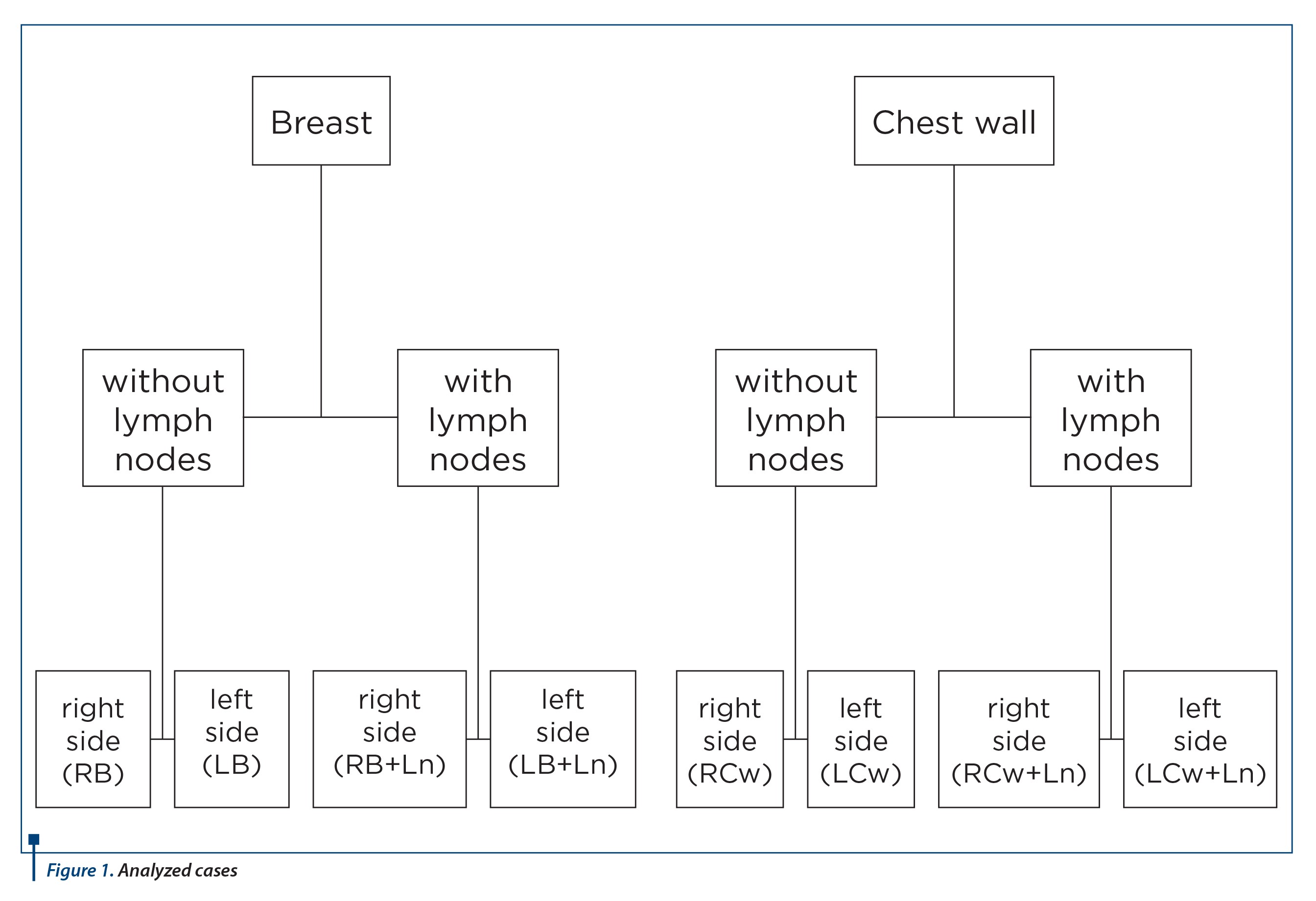
Breast cancer cases that went into treatment during 2016 in the Radiotherapy Department of OncoHelp Foundation have been selected. In the end we have analyzed 114 clinical cases which fit the criteria to be analized in this retrospective study. The selection has been made strictly on prescribed dose (all cases with dose prescription of 50 Gy in 25 fractions have been analyzed). Selected cases have been divided into 8 categories, depending on the position, geometry and size of the PTV, in order to be analyzed as divided in Figure 1.
All cases benefited from a 3D conformational treatment plan with X-ray beam, of 6 MeV, Eclipse planning system using the AAA calculus algorithm.
For each reviewed category, conformity and homogeneity indexes have been analyzed. And regarding the organs at risk, the dose collected by all health organs present near the target volume has been analyzed (ipsilateral lung, contralateral lung, contralateral breast and heart).
Results
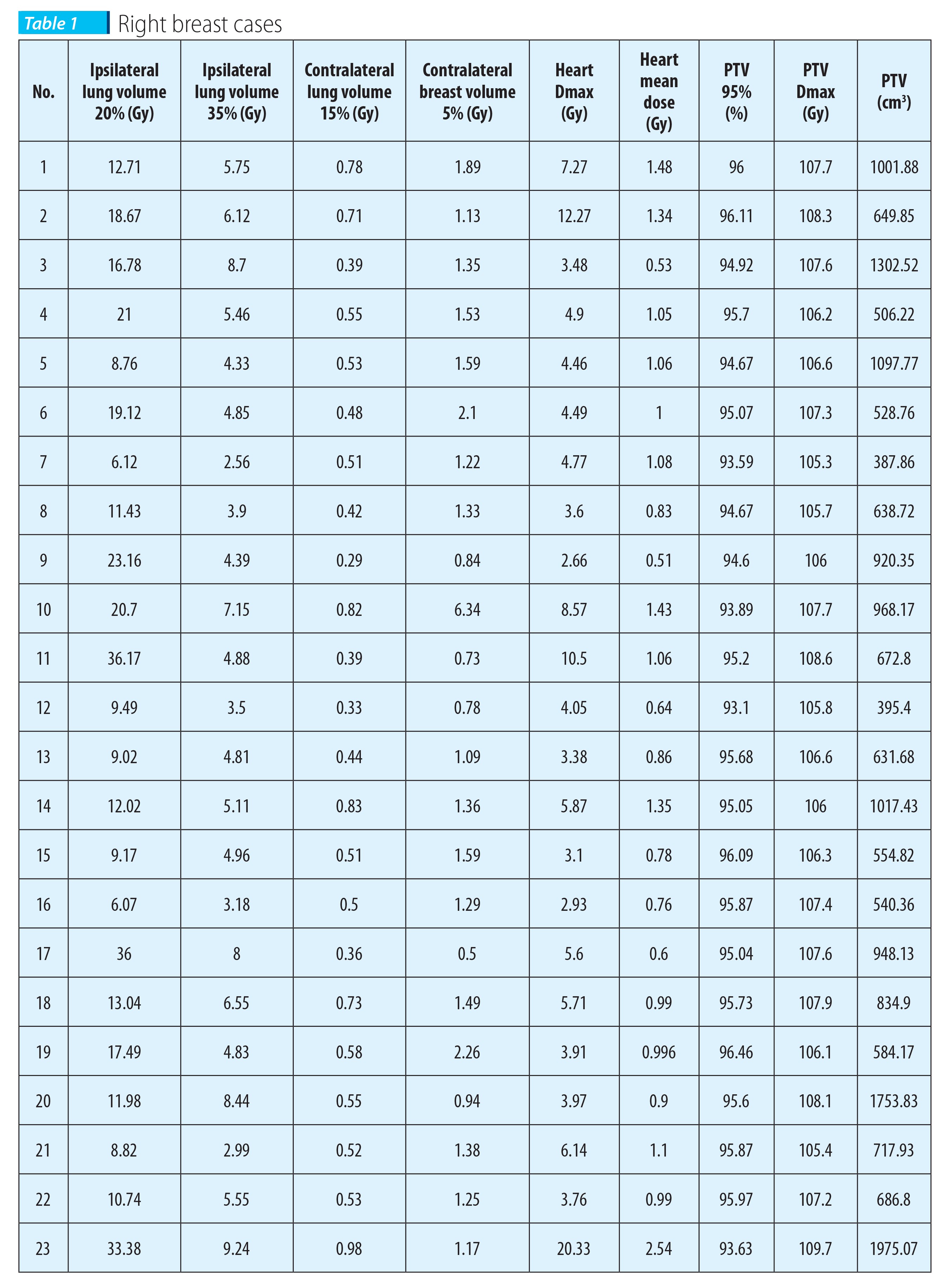
The tables below display the results obtained for all cases analyzed depending on PTV geometry. Table 1 details the data analyzed in the case of right breast irradiation, analysis of cases without lymph nodes included in the volume to be irradiated. We may observe an increased dose in the ipsilateral lung interdependent to the increase of PTV volume, as well as a larger hotspot in the PTV in the same reviewed cases.
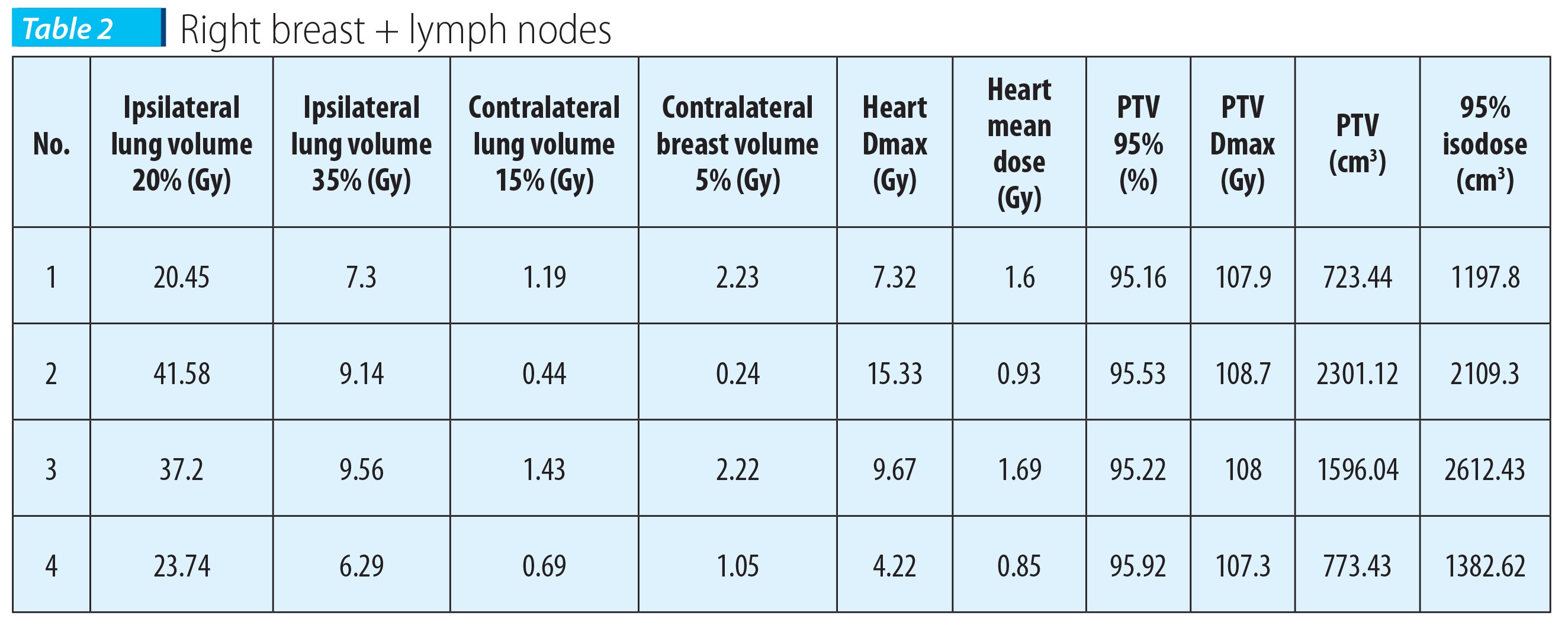
The same remarks may be made in the case of right breast irradiation with related lymph nodes included in the irradiated volume (Table 2), with the specification that 20% of the ipsilateral lung volume collects a significantly higher dose than cases with related lymph nodes not included in the target volume.
In the case of a PTV volume significantly higher than in all other reviewed cases, we may observe a few particular cases where the maximum heart dose exceeds 10 Gy, thus we may conclude that the heart may collect a significantly higher dose, including in right side breast irradiation, but which does not depend on PTV sizes, but strictly on the anatomy of each individual patient.
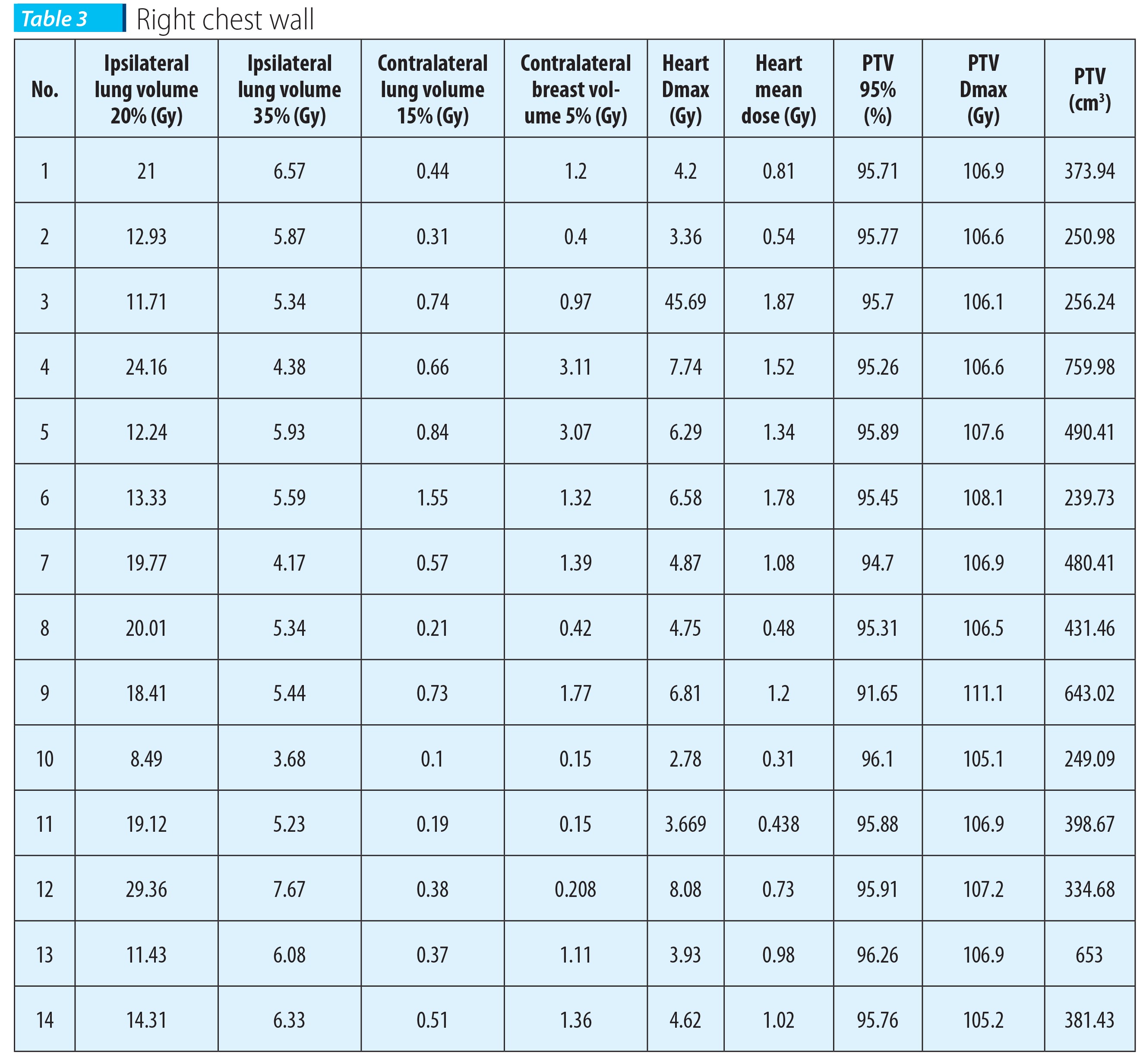
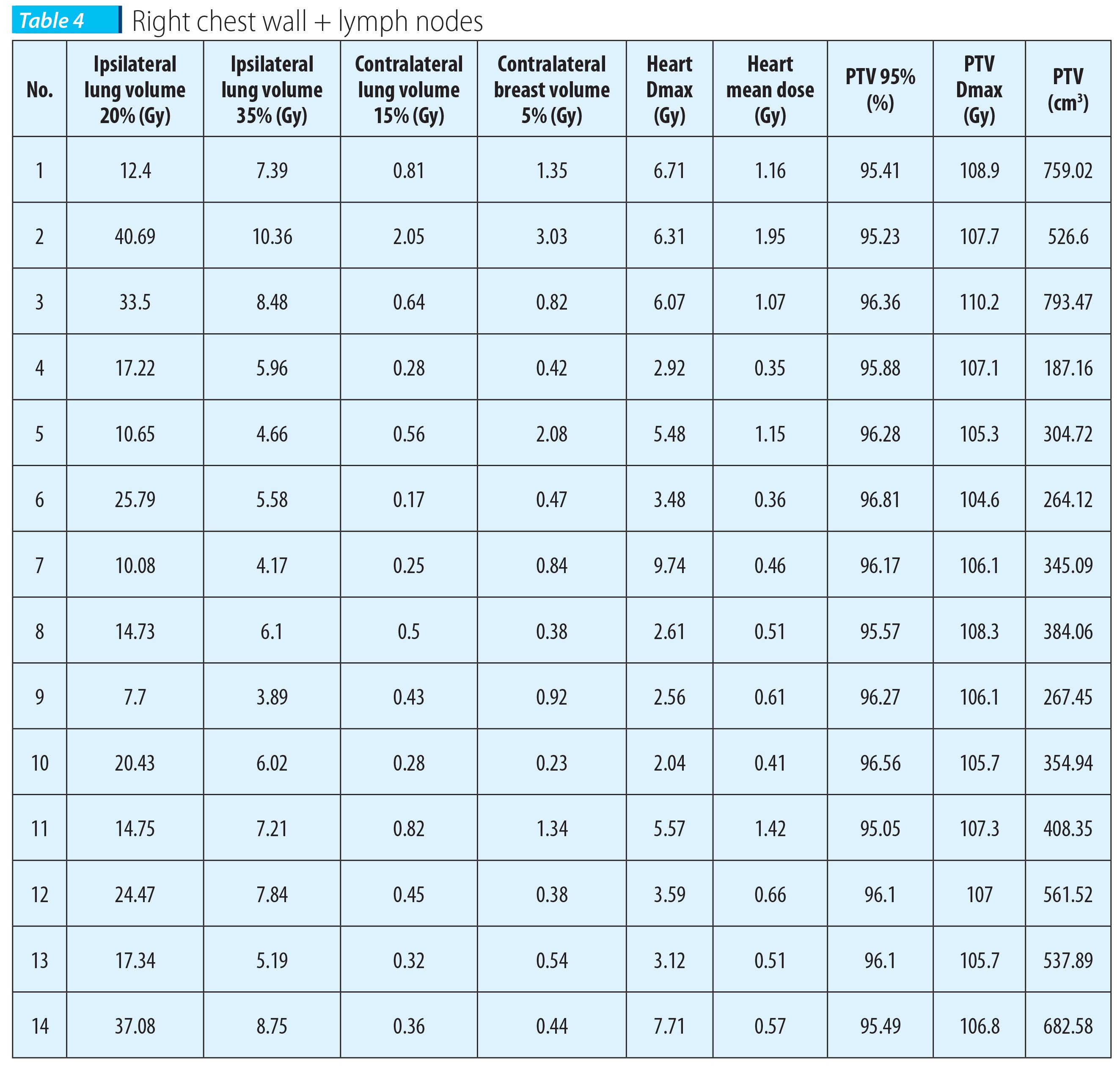
For the irradiation of the thoracic wall on the right side, with or without lymph nodes included (Table 3 and Table 4), we may observe a decrease of collected dose by the 35% volume from the ipsilateral lung, with a dose average in the 35% volume of the contralateral lung under 1 Gy as compared with the average dose collected by the 35% volume of the contralateral lung in cases analyzed for right side irradiation without mastectomy which fall below the 1 Gy dose.
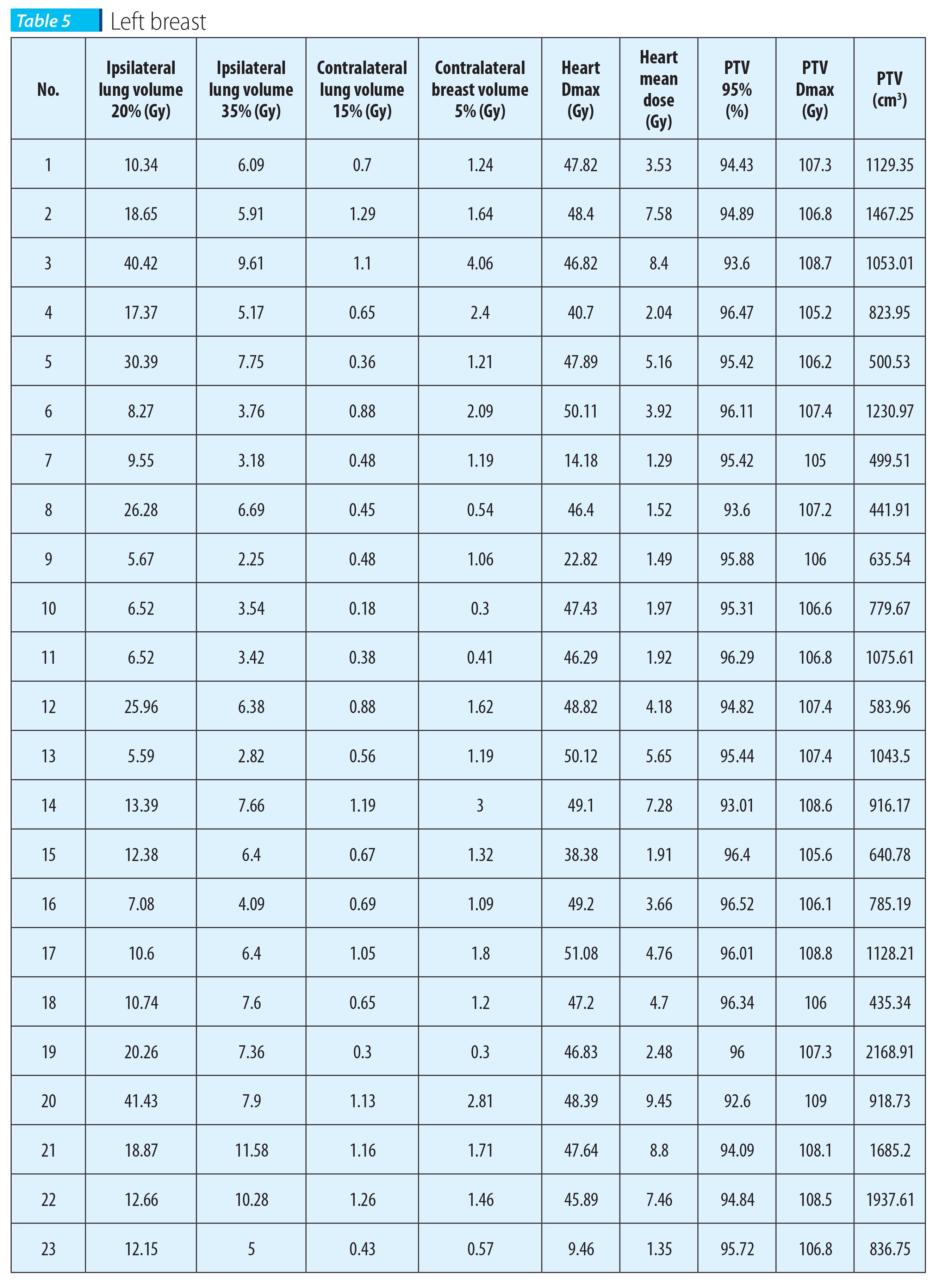
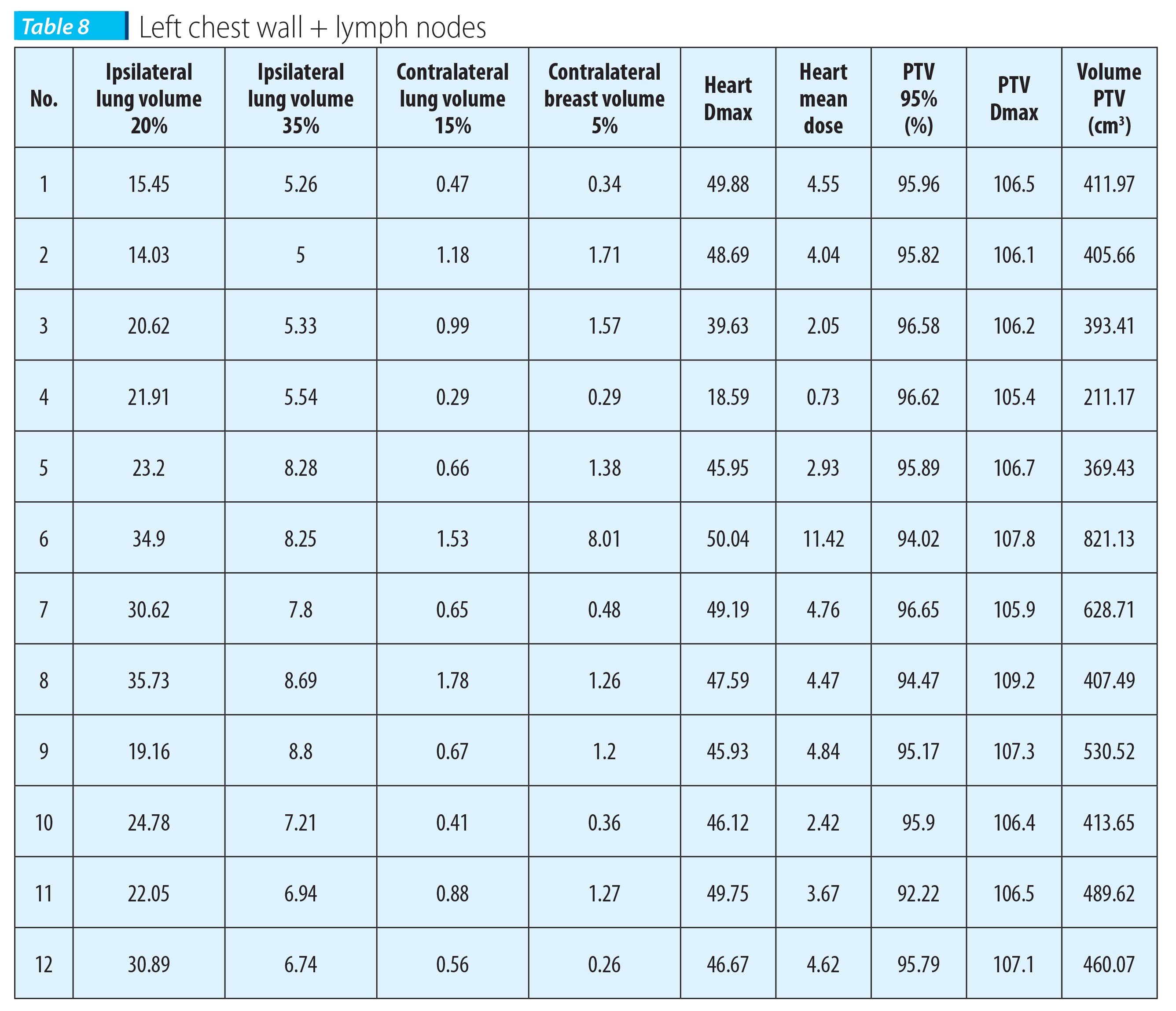
For cases analyzed in the case of left side irradiation, we may detect the same pattern both regarding the 20% and the 35% volume of the ipsilateral lung as in previously analyzed cases for the right side (Tables 5, 6, 7, and 8).
The major difference between the analysis of the left side and the right side breast irradiation in the case of 3D conformal technique lies in the maximum dose collected by the heart, especially in the coronary artery. Literature states that 1 Gy supplied on the coronary artery increases the risk of cardiac morbidity by 2%(6). It is vital to protect the heart in cancer irradiation, especially in the case of patients with heart disease background.
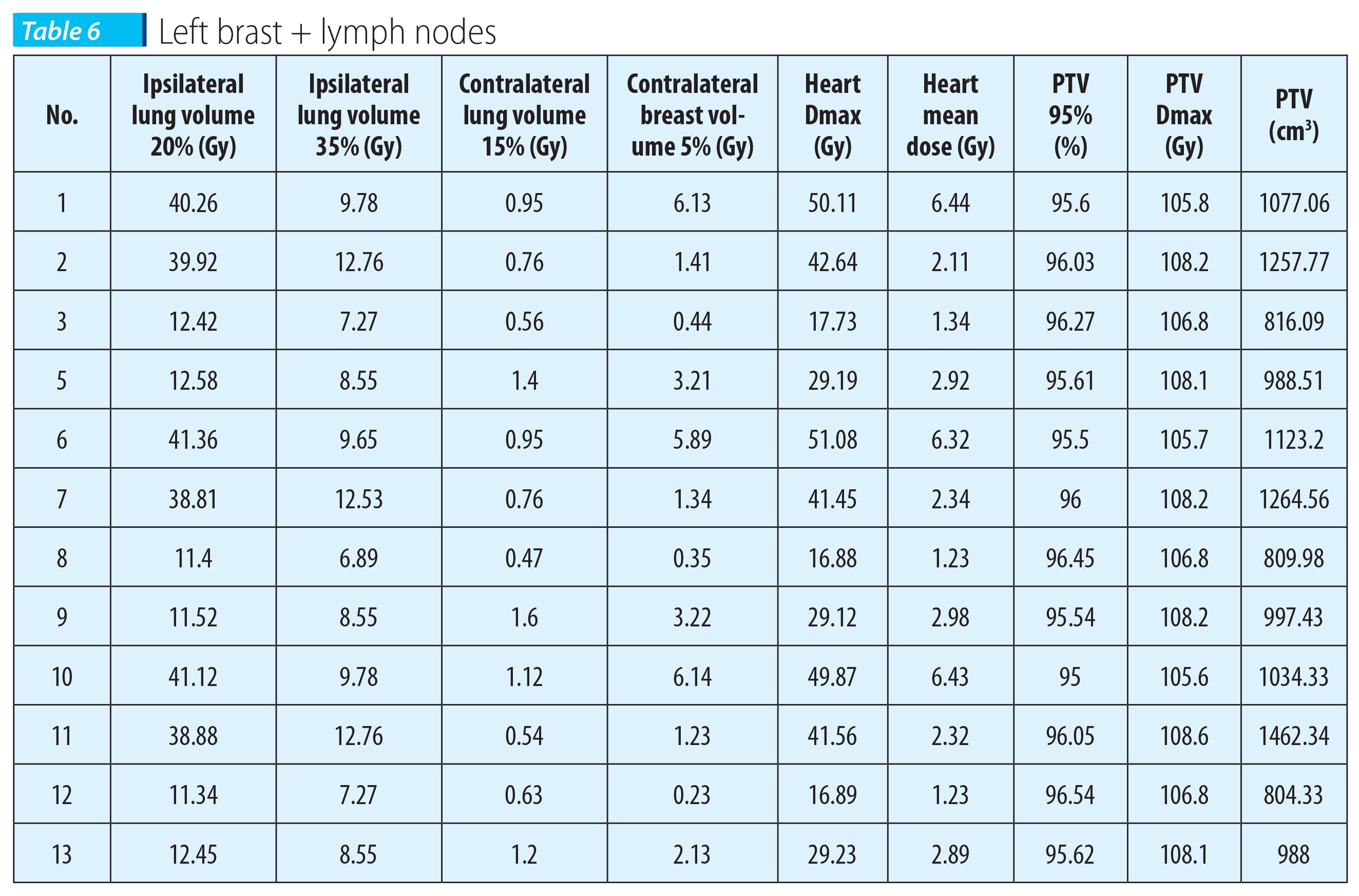
We may notice (Table 6) that the average maximum dose collected by the heart for clinical cases analyzed for the left breast with lymph nodes included in the PTV is below 35 Gy, at least 10 Gy lower than the average of the other three cases analyzed in the study of left side breast irradiation.
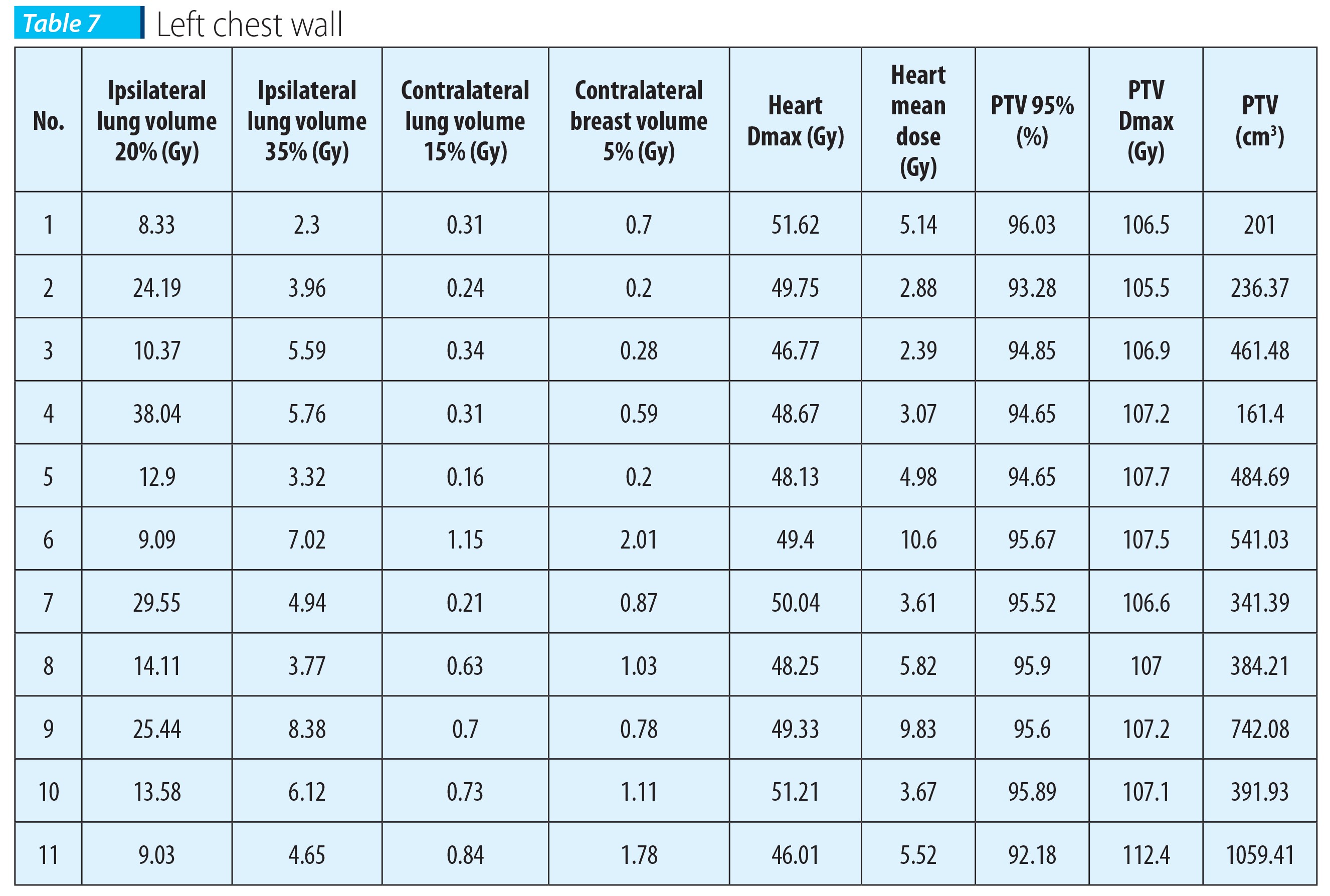
For both plain chest wall irradiation (Table 7) and irradiation of the chest wall with related lymph nodes (Table 8), we may notice that the decrease pattern of the ipsilateral lung irradiation is maintained, as in the cases analyzed for the right side, with the remark that the maximum average obtained for the heart is the highest (among all 8 situations analyzed in this study) in the case of left side chest wall irradiation.
Discussions
All breast cases of the clinical practice of the radiotherapy department in 2016 have been presented, which comply with the 50 Gy in 25 fractions dose prescription criterion.As a result of reviewing the treatment plan, for medical reasons some of the patients presented in this study have underwent another treatment plan, using the IMRT technique.
The purpose of this study is to be able to predict the appropriate treatment technique for a 50 Gy in 25 fractions dose prescription in breast cancer irradiation, depending on the position, sizes and localization of the PTV, in order to obtain the best treatment plan for each particular case, in compliance with physician’s requirements depending on the medical history of each patient.
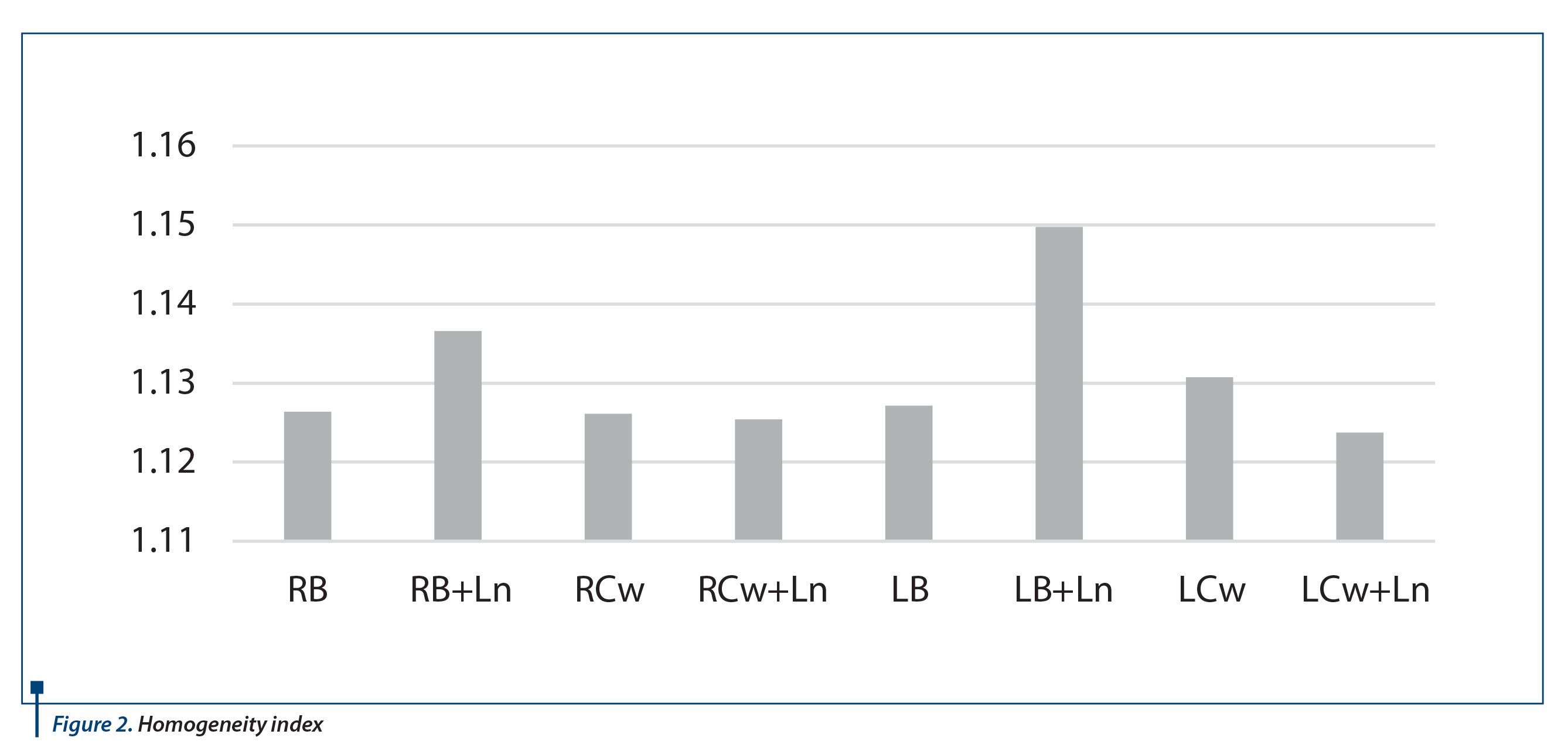
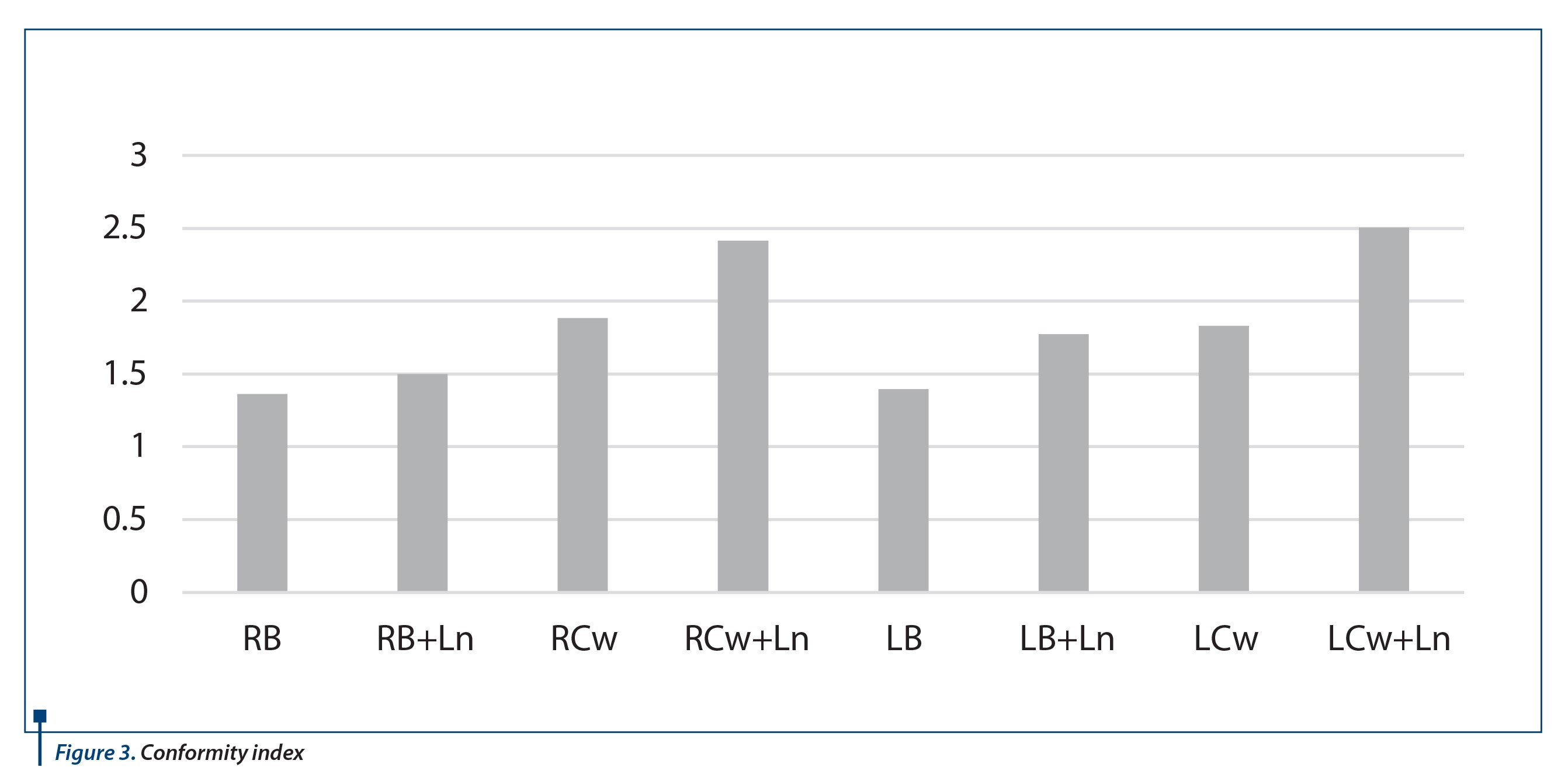
In order to demonstrate the quality of treatment plans subject to analysis regarding PTV coverage with minimum 95% of the prescribed dose and compliant with the maximum dose, conformity and homogeneity indexes have been calculated (Figure 2 and Figure 3)(7).
Why would this study be useful in clinical practice?
- 3D conformal is still a standard in breast irradiation and IMRT is used only when the advantage of using it is bigger than the risk caused by patient’s movement when breathing.
- It is less time consuming and more cost-effective to calculate the most appropriate plan from the beginning, which is very important in clinical practice.
Conclusions
In order to obtain a real correlation between the simulated treatment plan and the patient’s treatment, a real analysis of all the disturbing factors that may occur during the treatment is necessary. When performing the 3D treatment plan these factors have less influence on the efficiency of the treatment than the IMRT plans, where due to the fluence variation of the beam, any positioning error, like breathing, can decrease the efficiency of the treatment, even though in theory the IMRT technique is superior to 3D conformal technique.In breast cancer irradiation it can’t be generalized that one irradiation technique is superior to another, due to the fact that each patient is different. When analyzing the cases, it can be observed that patients who should be treated with the IMRT technique can be chosen depending on the organs at risk that need to be spared according to the PTV shape, as following:
1. When ipsilateral lung should be spared, IMRT technique should be used when the volume to be irradiated has lymph nodes included (large PTV).
2. When the heart needs to be spared, IMRT technique should be used when the volume to be irradiated is on the left side of the patient. n
Acknowledgement
We would like to thank to dr. Ioana Lupșe and medical physicist Bogdan Ile for their contribution in acquisition and data analysis.
Special thanks for guidance and support goes to Head of Radiotherapy Department of OncoHelp Foundation, dr. Anca Croitoru.
Mention: This retrospective analysis is not subject to any conflict of interests.
Bibliografie
2. Thomas Bortfeld. Effects of intra-fraction motion on IMRT dose delivery: statistical analysis and simulation, Physics in Medicine and Biology, vol 47, 2002.
3. Coen W Hurkmans. Reduction of cardiac and lung complication probabilities after breast irradiation using conformal radiotherapy with or without intensity modulation, Radiotherapy and Oncology, vol 62, 2002.
4. Giovanna Galigardi. Radiation Dose-Volume effects in the heart, Int J. Radiation Oncology. Biol. Phys. Vol 76, 2010.
5. Mudasir Ashraf. Dosimetric comparison of 3DCRT versus IMRT in whole breast irradiation of early stage breast cancer, International Journal of Cancer Therapy and Oncology, August 2014.
6. Jacques H Borger. Cardiotoxic effects of tangentioal breast irradiation in early breast cancer patients: The role of irradiated heart volume, International Journal of Radiation Oncology Biol. Phys, vol 69, 2007.
7. Loic Feuvret, Conformity index: a review, Int J Radiation Oncology Biol Phys, vol 64, 2006.