Cardiac metastases are not as rare as considered, their incidence ranging from 2.3% to 18.3%, most commonly from lung cancer. We report the case of a 57-year-old male with a second primary lung cancer in stage IV, with intracardiac mass, developed after a clear renal cell carcinoma. The particular features of the case are discussed, highlighting the important aspects of diagnosis, with reference to known data.
CASE REPORT
Un al doilea cancer pulmonar primar, cu masă intracardiacă dezvoltată după malignitate renală – prezentare de caz şi review al literaturii
Second primary lung cancer with intracardiac mass developed after renal malignancy – case report and literature review
First published: 16 mai 2018
Editorial Group: MEDICHUB MEDIA
DOI: 10.26416/OnHe.43.2.2018.1694
Abstract
Rezumat
Metastazele cardiace nu sunt pe atât de rare pe cât se consideră, incidenţa lor fiind cuprinsă între 2,3% şi 18,3%, cel mai adesea secundare cancerului pulmonar. Prezentăm cazul unui pacient de 57 de ani, cu un al doilea cancer pulmonar primar în stadiul IV, cu o masă intracardiacă, dezvoltată în urma unui carcinom renal cu celule clare. Sunt discutate particularităţile acestui caz, subliniind aspectele importante privind diagnosticul, referindu-ne şi la datele existente.
Introduction
Although the outcome of patients diagnosed with renal cell carcinoma (RCC) has improved over the past years, there is a lack of information on the risk of developing a second cancer after RCC.
A population-based study conducted in Norway indicated that nearly 47% of patients with RCC develop a subsequently malignancy, and lungs are a common site of occurence(1,2).
Other studies reported an increased risk of subsequent bladder and prostate cancer for papillary RCC(3,4).
On the other hand, metastatic spreads to the heart are not as rare as considered, their incidence ranging from 2.3% to 18.3%, most commonly from lung cancer through a lymphatic or hematogenous pathway. Furthermore, lung adenocarcinoma has a higher rate of heart metastases (21%) compared to lung squamos cell carcinoma (18.2%)(5,6).
Case presentation
A 57-year-old male, non-smoker, with history of clear renal cell carcinoma (T3N1M0), diagnosed in 2009, for which he had undergone radical nephrectomy on his left side, radiotherapy and received treatment with interferon-alpha, presented to our clinic in May 2014 complaining of progressive dyspnea, productive cough, chest pain and important weight loss (14 kg in two months).
The chest X-ray and the CT scan revealed a tumor mass in the right lower lobe of his lung (6.6/4.5 cm), enlarged mediastinal lymph nodes, and low-density masses in the liver.
The biopsy of a mediastinal lymph node by Carlens mediastinoscopy, and the histopathological findings revealed metastatic adenocarcinoma G3.
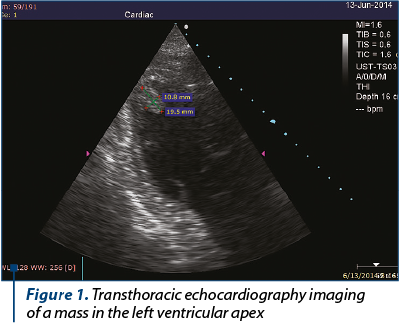
Palliative chemotherapy was initiated, the pacient receiving two cycles of carboplatin with vinorelbine. After that, without any symptomatic change, transthoracic echocardiography detected in his left ventricular apex a high echogenic mass (1.95/1.08 cm), with no pericardial effusion and no detectable valvular abnormality (Figure 1).
The differential diagnosis included thrombus. However, taking into account that no hipokinesia or left ventricular hyperthrophy was detected and he had a normal ejection fraction, we considered the mass as a cardiac metastasis.
The chemotherapy was changed, the patient receiving one cycle of pemetrexed plus cisplatin. Unfortunately, soon after, the family informed us that he passed away, and no autopsy was performed.
Discussion
There are two important aspects worth highlighting in our clinical case, namely the development of a second primary lung malignancy after clear RCC, and the appeareance of a solitary cardiac metastasis in the evolution. Clear cell RCC represents the predominant histological subtype of RCC (70-85%), and the development of a second primary cancer after clear cell RCC seems to be more frequent than expected, with lungs as a commun site of occurence(1,2,7).
Therefore, in order to establish an optimal follow-up program for patients with RCC, we should consider the risk of developing other subsequent primary cancer, and promote an effective surveillance for early detection. Regarding cardiac malignancies, most of them are secondary tumors, produced by lung cancer or many other cancers, with a small size, multiple, commonly asymptomatic and indicating widespread metastases. Despite the fact that majority of them are clinically silent, the risk of embolism is high and can lead to death; thus, echocardiography is important in oncologic patients, with or without cardiac symptoms.
To the best of our knowledge, solitary cardiac metastases with intracavitary growth are rare.
Conflict of interests: The authors declare no conflict of interests.
Bibliografie
- Beisland C, Talleraas O, Bakke A, et al. Multiple primary malignancies in patients with renal cell carcinoma: a national population-based cohort study. BJU Int. 2006; 97:698–702.
- Chakraborty S, Tarantolo SR, Batra SK, Hauke RJ. Incidence and prognostic significance of second primary cancers in renal cell carcinoma. Am J Clin Oncol. 2013; Apr, 36(2):132-42.
- Rabbani F, Reuter VE, Katz J, Russo P. Second primary malignancies associated with renal cell carcinoma: influence of histologic type. Urology. 2000; Sep 1; 56(3):399-403.
- Neuzillet Y, Lechevallier E, Coulange C. Renal cancer and second cancer: critical review of the literature. Prog Urol. 2007; Feb, 17(1):35-40.
- Bussani R, De-Giorgio F, Abbate A, Silvestri F. Cardiac metastases. J Clin Pathol. 2007; 60:27–34.10.1136/jcp.2005.035105.
- Klatt EC, Heitz DR. Cardiac metastases. Cancer. 1990; Mar 15; 65(6):1456-9.
- Crumley SM, Divatia M, Truong L, Shen S, Ayala AG, Ro JY. Renal cell carcinoma: Evolving and emerging subtypes. World J Clin Cases. 2013; Dec 16; 1(9): 262–275.
Articole din ediţiile anterioare
THERAPEUTIC GUIDELINE | Ediţia 1 54 / 2021
Breviar terapeutic al cancerului pulmonar fără celule mici, din perspectiva oncologiei medicale
Alexandru Grigorescu, Ciprian Ciobotaru
Acest ghid sumarizează recomandările Societăţii Americane de Oncologie Clinică şi prezintă într-o manieră schematică principalele modalităţi de abo...
24 martie 2021
PALLIATIVE CARE | Ediţia 1 58 / 2022
Symptoms control in patients with advanced lung cancer
Alexandru Grigorescu
Prezentăm un scurt review despre principalele simptome întâlnite în cancerul pulmonar, şi anume dispneea, tusea şi hemoptizia. Un aspect particula...
25 martie 2022
CASE PRESENTATION | Ediţia 4 41 / 2017
Adenocarcinom mucinos pulmonar primitiv la o femeie nefumătoare
Irina Strâmbu, Livia Luculescu, Ciprian Bolca, Diana Leonte, Daniela Dorina Vasile, Alexandru Stanciu
Adenocarcinoamele sunt cele mai frecvente tipuri histologice de cancer pulmonar. Dintre ele, adenocarcinomul mucinos pulmonar primitiv (fostu...
20 decembrie 2017
CASE PRESENTATION | Ediţia 4 53 / 2020
Importanţa rebiopsierii pentru detectarea mutaţiei T790M în cancerul pulmonar fără celule mici – prezentare de caz
Andreea Mihaela Radu, Iulia Tatiana Lupaşcu, Isabela Anda Komporaly, Adelina Silvana Gheorghe, Elena Adriana Mateianu, Conf. dr. Dana Lucia Stănculeanu
Lung cancer, the leading cause of mortality worldwide, is comprised in proportion of 80-85% of non-small cell lung carcinoma (NSCLC).
23 decembrie 2020