Anatomy based on imagistic findings is the key point on which the understanding of normal and pathological structures is based. Nowadays, the conventional radiology has been replaced by CT imaging, the new gold standard for paranasal sinus pathology. Functional endoscopic sinus surgery is now the most popular technique used in sinonasal pathology and it cannot be performed without knowing the anatomic landmarks. A good understanding of sinonasal anatomy and of anatomic variants provides a better surgical approach. The aim of this article is to focus on the landmarks found on CT scan in order to avoid the complications of ethmoid sinus surgery. In this article, we present the imagistic appearance on CT of ethmoid landmarks beginning from anterior ethmoid (agger nasi, uncinated process, ethmoidal bulla, middle turbinate) to posterior ethmoid (ethmoidal cells, superior turbinate). We also focused on the areas in which complications may occur (lamina papyracea, anterior and posterior ethmoid artery, cribriform plate). The reduction of complications incidence begins with prevention by having a good preoperative medical assessment. The surgeon needs to study the CT imaging for each patient several times before the procedure.
Aspecte particulare ale anatomiei etmoidale pe imagini CT
Particular CT scan aspects in ethmoid anatomy
First published: 26 septembrie 2019
Editorial Group: MEDICHUB MEDIA
DOI: 10.26416/Orl.44.3.2019.2554
Abstract
Rezumat
Anatomia ilustrată pe descoperirile imagistice reprezintă baza înţelegerii structurilor normale şi patologice rinosinuzale. Actualmente, radiologia convenţională a fost înlocuită de imagistica CT, noul standard de aur în patologia sinusurilor paranazale. Chirurgia endoscopică sinuzală este în prezent cel mai frecvent procedeu utilizat, putând fi efectuată doar cunoscând reperele anatomice. O bună înţelegere a anatomiei rinosinuzale şi a variantelor anatomice asigură realizarea unei intervenţii chirurgicale cu un grad scăzut de risc al complicaţiilor. Scopul acestui articol este să evidenţieze reperele anatomice prezente pe imaginile CT. Aceste repere ajută la evitarea complicaţiilor în timpul intervenţiilor chirurgicale de tip endoscopic asupra etmoidului. În articol se evidenţiază aspectul imagistic al reperelor anatomice etmoidale, începând cu etmoidul anterior (celula agger nasi, procesul uncinat, bula etmoidală, cornetul nazal mijlociu) spre cel posterior (celulele etmodiale, cornetul nazal superior). De asemenea, se pune accent şi pe zonele la nivelul cărora sunt frecvent descrise complicaţii intraoperatorii (lamina papiraceea, arterele etmoidale anterioară şi posterioară, lama cribriformă). Reducerea incidenţei complicaţiilor are la bază o bună evaluare preoperatorie a pacientului. Chirurgul are responsabilitatea de a studia imaginile CT pentru fiecare pacient, de mai multe ori, înaintea procedurii chirurgicale.
Introduction
The CT scan represents the imaging investigation of choice in case of sinonasal pathology, at the same time the CT images revealing the anatomical variants of this region.
The clinical picture according to the anatomical variants, from the level of the ethmoid, is represented by rhinogenic headache, facial pressure, inefficient drainage, or it can be asymptomatic, being discovered accidentally after an imagistic investigation.
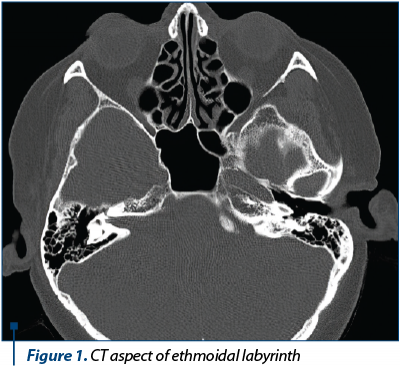
The ethmoid is a bone with a complex configuration, which participates in forming the walls of the nasal cavity, orbit and the floor of anterior cranial fossa. It is located at the level of the ethmoidal incision of the frontal bone and articulates with the sphenoid, maxillary, vomer, lacrimal, nasal, palatine, and quadrilateral cartilage. From an anatomic point of view, the ethmoid consists of the perpendicular blade, the horizontal blade and the two lateral masses (the ethmoidal labyrinth) – Figure 1.
The elements of the anterior ethmoid with anatomical variability must necessarily be followed and most often found on CT images. The anatomical variants of the ethmoidal structures can cause changes in the normal sinus physiology, which impose an appropriate therapeutic behavior. We followed on the CT images different anatomical structures of the anterior and posterior ethmoid.
1. Agger nasi cell
The agger nasi cell represents the anterosuperior cell of the anterior ethmoid and is part of the uncinate cellular system. When it exists, it represents an ethmoidal pneumatization, located at the level of the lacrimal bone, and it is an important landmark in the approach of the frontal sinus recess. On the CT image, it is identified superior by the insertion of the middle turbinate and anterolateral and inferior by the frontal sinus recess. A pneumatized agger nasi cell can block the frontal sinus drainage (Figure 2).

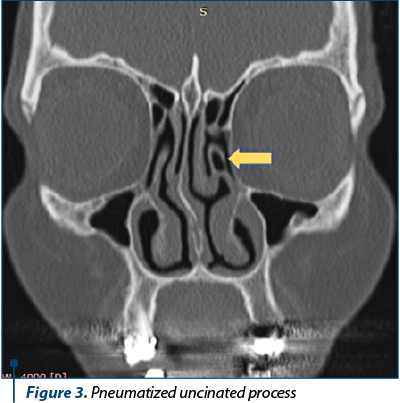
2. Pneumatized uncinate process
The uncinate process (first lamella) is a thin ethmoidal bone lamella, sagittal oriented, from anterior and superior to posterior and inferior; it forms the anterior limit of the semilunar hiatus. When the uncinate process is hypertrophied and in contact with the mucosa of the ethmoidal bulla or the middle turbinate, it blocks the normal sinus drainage through the ethmoidal infundibulum and may cause obstruction of osteomeatal complex (OMC), resulting in altered ventilation of the anterior sinuses of the face (Figure 3).
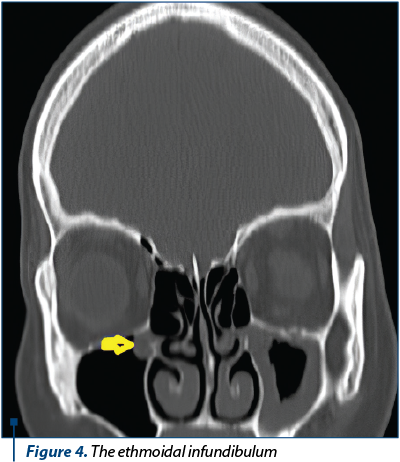
3. The ethmoidal infundibulum
The ethmoidal infundibulum represents the three-dimensional space where we can find the ostium of the maxillary sinus (most commonly). When the uncinate process is inserted on the ethmoidal roof or middle turbinate, the frontal sinus drains into the ethmoidal infundibulum. The clinical picture of the obstruction of the infundibulum is represented by the facial pressure sensation and the lack of sinus ventilation (Figure 4).
4. Ethmoidal bulla
The ethmoidal bulla is a bony protrusion of the nasal lateral wall, known in the Anglo-Saxon literature as “second lamella”. It represents an important landmark in endoscopic sinus surgery, being the most consistently pneumatized anterior ethmoidal cell. The lateral wall of the ethmoidal bulla is always represented by lamina papyracea. On the coronal section it is visualized superior by the ethmoidal infundibulum and posteriorly by the hiatus semilunaris (Figure 5).
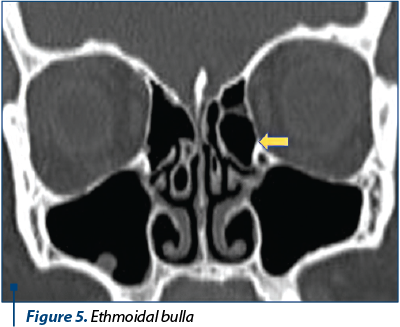
The degree of pneumatization may vary: it extends superiorly (ethmoidal roof), posteriorly (lamina basalis) or laterally (lamina papyracea). In the case of a large bulla, it will occupy the entire middle meatus, being in contact and exerting pressure at the root of the middle nasal turbinate (at the posterior opening of the ethmoidal bulla it reaches directly into the posterior ethmoid) and the uncinate process (anterior) and frontal recess (superior) with the disruption of drainage of the anterior sinuses of the face.
5. Concha bullosa
Concha bullosa represents the pneumatization of the middle turbinate, sometimes causing changes to the sinus physiology by obstructing the middle meatus and implicitly the drainage pathways of the anterior paranasal sinuses.
The classification by Bolger highlights three types of pneumatization: bulbous, lamellar, and extensive (Figure 6).
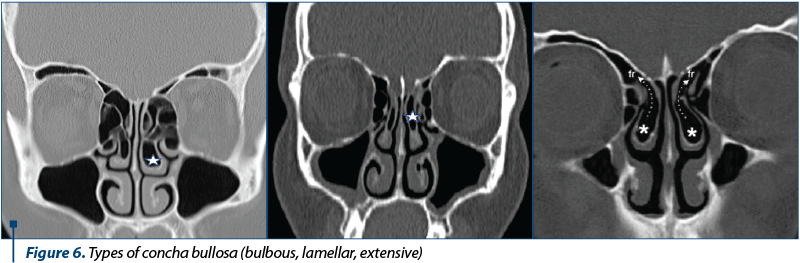
The clinical picture is dominated by persistent frontal headache, facial pressure, chronic nasal obstruction and hyposmia, symptomatology that directs patients to have an imaging investigation.
6. Paradoxical middle turbinate
Typically, the middle turbinate is inserted superior on the lateral nasal wall or ethmoid roof, having a descending direction with the concavity located sideways. The paradoxical middle turbinate is an anatomical entity in which its concavity is oriented in direction of the nasal septum, and the convex face blocks the drainage at the level of the hiatus semilunaris. It is usually found bilateral (Figure 7).

The treatment in this type of anatomical variant is surgical and consists in the resection of the concave part of the middle turbinate with the positioning of the middle turbinate in the normal variant, allowing the drainage and ventilation of the anterior sinuses.
7. Haller cell
The maxillo-ethmoidal cell – orbito-ethmoidal cell or Haller cell – develops by pneumatization from the level of the anterior ethmoid towards the maxillary sinus and always presents a common wall with the orbit.
It is located in the medial region of the maxillary sinus ceiling and the lowest portion of the lamina papyracea, under the ethmoidal bulla, laterally by the uncinate process. The Haller cell contributes to the narrowing of the ethmoidal infundibulum and can compromise the normal physiology of the maxillary sinus (Figure 8).
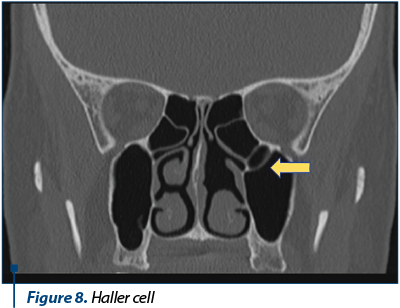
The diagnosis of Haller cell is established by CT imaging, most of the time being a random breakthrough following a regular sinonasal imaging investigation.
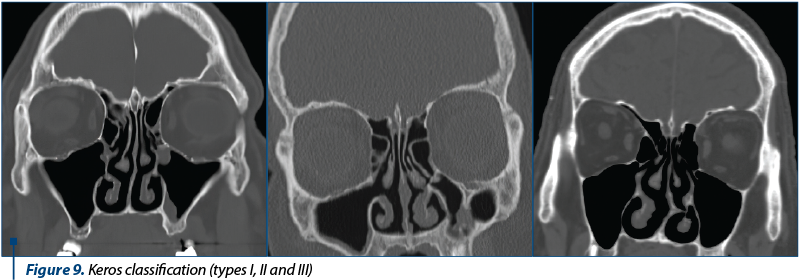
8. Ethmoidal roof
The ethmoidal bony wall of the skull base consists of the cribriform plate and the ethmoidal roof and divides the nasal cavity from the anterior and middle cerebral fossa. The Keros classification is an objective method in measuring the depth of the olfactory fovea. In adults, the recess is represented by a variable depression of the cribriform plate which represents the thinnest structure of the skull base, being roamed by the olfactory nerves and interconnecting arteries (Figure 9).
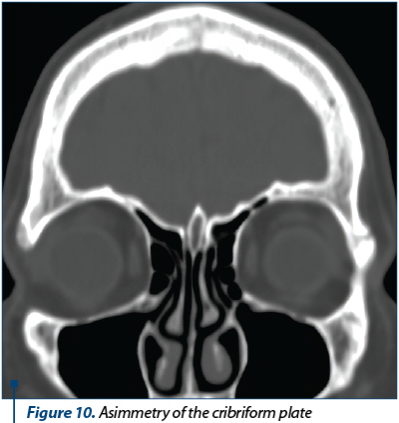
CT scan is a standard method of identifying the height of the ethmoidal roof. The surgeon must identify possible asymmetries of the olfactory fovea and assesses preoperatively the risk of intracranial complications with the possibility of producing a bony or dural injury, with the occurrence of a cerebrospinal fluid leak (Figure 10).
9. Anterior ethmoidal artery
The anterior ethmoidal artery is a branch of the ophthalmic artery and represents an important anatomical landmark in endoscopic sinus surgery. This artery can be found in the posterior segment of the frontal recess and has a path originating from the medial orbital wall to the nasal septum. On CT scan, a small bulge in the lamina papyracea (discontinuous appearance of the lamina) can be observed, which pinpoints the position of the anterior ethmoidal artery (Figure 11).
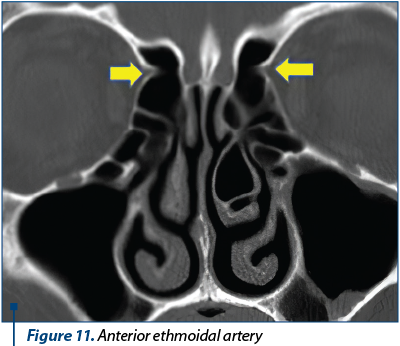
Injury inflicted upon this artery produces significant bleeding and may cause orbital hematoma as a result of the retraction of the sectioned artery in the orbit, requiring emergency orbital decompression.
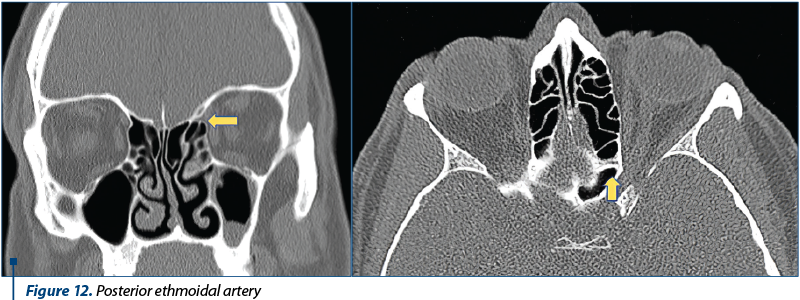
10. Posterior ethmoidal artery
The anatomy of the ethmoidal arteries is important for surgeons, as their injury can cause intraorbital hemorrhage and blindness due to a retrobulbar hematoma through optic nerve compression. Most studies to date focus on the anterior ethmoidal artery, and less on the posterior (or middle) artery. After detaching from the ophthalmic artery, the posterior ethmoidal artery provides vascular supply to the posterior ethmoidal cells, the posterior nasal septum, and an intracranial branch that is distributed to the dura mater.
The discovery of the posterior ethmoidal artery can be achieved by following the CT scans where we can find the posterior ethmoidal artery canal or the place where it leaves the olfactory fossa in route to orbit crossing the lamina papyracea (Figure 12).
11. Pneumatized superior turbinate
The superior turbinate is a part of the posterior ethmoid that medially borders the superior meatus. Most of the time, the superior turbinate is inserted on the ethmoidal roof. In case of a pneumatized superior turbinate (superior concha), the sphenoethmoidal recess gets blocked, leading to inefficient sinus drainage (Figure 13).
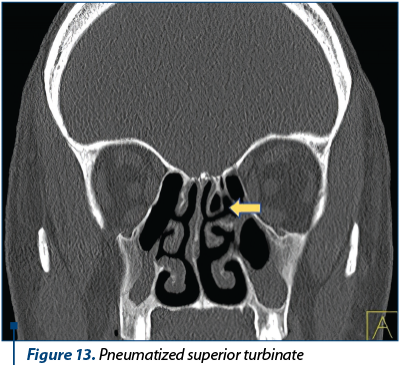
This anatomical-clinical situation requires endoscopic surgery with removal of the pneumatized superior turbinate. Some studies even show a causal relationship between the rhinogenic headache and the presence of pneumatized superior turbinate. Pneumatized superior turbinate is often found bilaterally and can associate, besides headache, anosmia or hyposmia, by blocking the olfactory fovea.
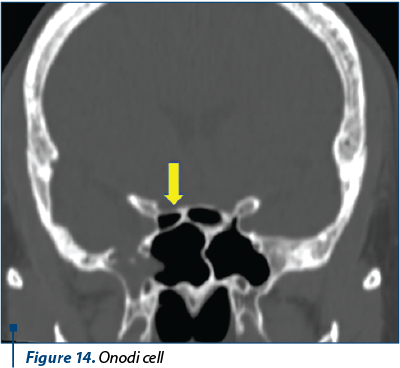
12. Onodi cell
Onodi cell is a sphenoethmoidal air cell where we can identify the optic nerve projection on its wall. It is very important to identify any Onodi cell on a CT scan, before any endoscopic sinus surgery, because this air cell can surpass laterally and superiorly the sphenoid. Once the position of the Onodi cell is found in the CT scan, it is important during endoscopic sinus surgery not to confuse it with the sphenoid sinus, in order to avoid intracranial complications (Figure 14).
Conclusions
Unsystematic headache, sometimes accompanied by facial pressure, causes difficulties in diagnosis and treatment. The endoscopic nasal exam and the computed tomography allow the proper diagnosis and therapeutic management to be established.
The anatomical variants of the ethmoidal structures can cause changes in the drainage and ventilation of the paranasal sinuses, and the treatment usually consists in surgical procedure. In order to perform an endoscopic sinus surgery, it is necessary to study the sinonasal anatomy through the CT investigation.
Conflict of interests: The authors declare no conflict of interests.
Bibliografie
- Dunnebier EA, Beek E, Pameijer F. Imaging for Otolaryngologists. Thieme Publishing Group. 2011.
- Shah G, Wesolowski J, Choi J. Head and Neck Imaging. Thieme Publishing Group. 2016.
- Moedder U, Cohnen M, Anderson K, et al. Head and Neck (Direct Diagnosis in Radiology). Thieme. 2007.
- Bradoo R. Anatomical Principles of Endoscopic Sinus Surgery. Taylor & Francis Group. 2005.
- Mancuso A, Hanafee W. Head and Neck Radiology. Lippincott Williams & Wilkins. 2010.
- Hasso A. Diagnostic Imaging of the Head and Neck. Lippincott Williams & Wilkins. 2012.