Aim. The paper aims at presenting the terminology and pathogenesis of dental eruption and at identifying the local causes of delayed eruption by clinical and radiological analysis of the permanent dentition. Materials and method. The study was performed on a group of 115 patients diagnosed with eruption delayed by local cause. The clinical data were collected by two examiners who performed both clinical analysis, orthopantomographies interpretation and the calculation of Demirjian index. Results and discussion. The distribution of the study group did not indicate significant differences between sexes and an average age of 12.58 years old. The average values of the Demirjian index of 7.43 for the inferior canine were calculated, 7.35 for the first mandibular premolar, 6.88 for the second mandibular premolar, and 6.9 for the mandibular permanent molar. The inferior canine erupts at 9.98 years of age differently from existing national standards, but similar to current American Academy of Pediatric Dentistry (AAPD) and European Academy of Pediatric Dentistry (EAPD) after the first premolar and sometimes even after the second premolar. Conclusions. The importance of delayed eruption as a clinical problem is reflected by numerous scientific publications that reflect many controversies over the terminology used, the pathogenesis of this unique developmental process in the body, and the reporting of standards derived from population studies. In current dental practice, significant deviations from accepted norms are observed; most frequently occurring is the delayed eruption which may be the first or the only manifestation of local or systemic pathology and may affect the accuracy of diagnosis, the planning of prophylactic or pedodontic treatment or the timing of orthodontic treatment, with a significant impact on the general health status of the child.
Erupţia dentiţiei permanente întârziată de cauze locale – patogeneză, terminologie, diagnostic
Eruption of permanent dentition delayed by local causes – pathogenesis, terminology, diagnosis
First published: 23 mai 2019
Editorial Group: MEDICHUB MEDIA
DOI: 10.26416/Orl.43.2.2019.2405
Abstract
Rezumat
Scop. Lucrarea îşi propune prezentarea terminologiei şi patogenezei erupţiei dentare şi identificarea cauzelor locale de erupţie întârziată prin analiza clinică şi radiologică în dentiţia permanentă. Materiale şi metodă. Studiul a fost efectuat pe un lot de 115 pacienţi diagnosticaţi cu erupţie întârziată de cauză locală. Datele clinice au fost colectate de doi examinatori, care au efectuat simultan analiza clinică, interpretarea ortopantomografiilor şi calculul indicelui Demirjian. Rezultate şi discuţii. Repartiţia lotului de studiu nu indică diferenţe semnificative între sexe şi o vârstă medie de 12,58 ani. Au fost calculate valori medii ale indicelui Demirjian de 7,43 pentru caninul inferior, 7,35 pentru primul premolar mandibular, 6,88 pentru premolarul 2 mandibular şi 6,9 pentru molarul 2 permanent mandibular. Caninul inferior erupe la 9,98 ani, moment diferit de standardele naţionale existente, dar similar standardelor actuale ale AAPD (American Academy of Pediatric Dentistry) şi EAPD (European Academy of Paediatric Dentistry), după primul premolar şi uneori chiar după premolarul 2. Concluzii. Importanţa erupţiei întârziate ca problemă clinică este reflectată de diversele publicaţii ştiinţifice care relevă numeroase controverse privind terminologia folosită, patogeneza acestui proces de dezvoltare unic în organism şi raportarea la standardele derivate din studii populaţionale. În practica stomatologică de zi cu zi se observă deviaţii semnificative de la normele acceptate, cel mai frecvent fiind întâlnită erupţia întârziată, care poate fi prima sau unica manifestare a unei patologii locale sau sistemice şi care poate afecta acurateţea diagnosticului, planificarea tratamentului profilactic sau pedodonţic sau timingul tratamentului ortodontic, cu impact semnificativ asupra stării generale de sănătate a copilului.
Introduction
Dental eruption is a physiological process in which temporary or permanent teeth move by axial movement from the nonfunctional formation and developmental position from the alveolar bone through the oral mucosa in functional occlusion on the dento-alveolar arch. The mechanism and source of eruptive forces have not yet been elucidated or fully understood(1). The normal eruption of temporary and permanent teeth occurs over an extended period of age, growth and development, and can be influenced by racial, ethnic, sexual and individual factors, considered determinant in the standardization of normal eruption.
In current dental practice, significant deviations from accepted norms are observed; most frequently occurring is the delayed eruption which may be the first or the only manifestation of local or systemic pathology and may affect the accuracy of diagnosis, the planning of prophylactic or pedodontic treatment or the timing of orthodontic treatment, with a significant impact on the general health status of the child(1).
Dental development standards are important in the bio-medical and anthropological field. The first studies on the standards of eruption in Romanian children were conducted 30 years ago(2-4) and they considered that teeth generally erupt earlier in girls than in boys, and that the interim period of mixed teeth is shorter in girls, with an individual 12-month variation from the eruption of permanent teeth that are considered to be within normal limits. In addition to the changes in the eruption sequence, in recent decades we can see the early eruption of permanent teeth, a process directly linked to the acceleration of general development, the early onset of puberty and the increase in living standards(5). Specialty literature suggests that temporary dentition may present fewer asymmetries and deviations from normal chronology due to the controlled intrauterine environment in which it is formed and the shorter calcification and development period of the fetus.
The importance of the delayed eruption as a clinical problem is reflected by numerous scientific publications that reflect many controversies over the terminology used, the pathogenesis of this development process (unique in the body), and the reporting to standards derived from population studies.
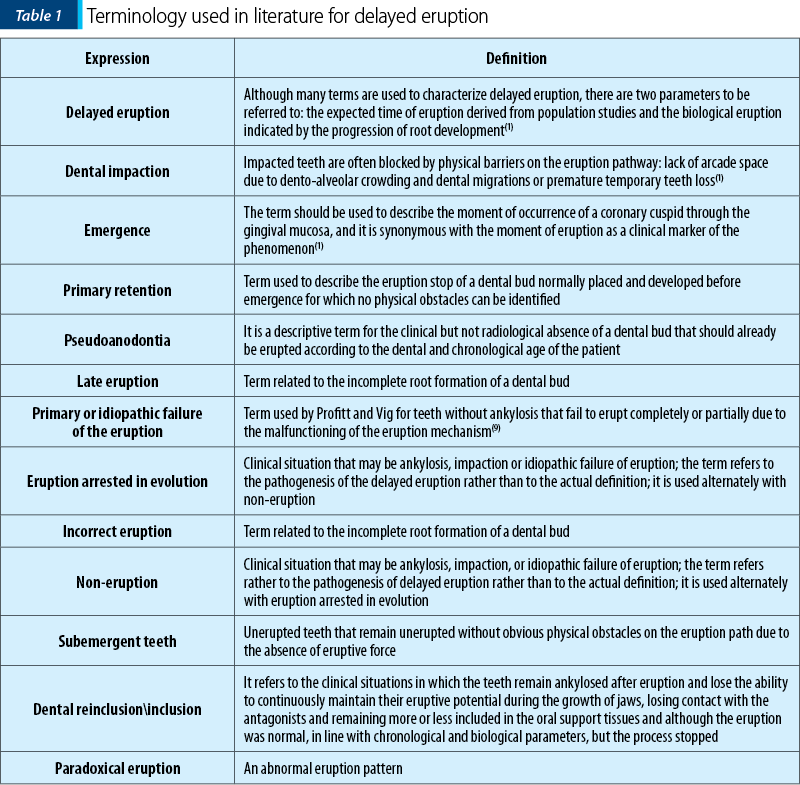
Definition and terminology
Eruption is the developmental process responsible for tooth movement from the intraosseous alveolar cryptus to the oral cavity and in occlusion position with an antagonist. It is a dynamic process that includes completing root development, organizing periodontics and maintaining functional occlusion. Controversies that exist in literature about the use of delayed, late, retarded and incorrect expressions are presented in Table 1, and are related to root formation. In 1962, Gron(6) showed that, in normal circumstances, dental eruption begins when the tooth root is formed at a rate of 75%. Becker(7) suggests that only root development is not enough, and Rasmussen and Katsaki(8) have calculated the mean age of eruption, indicating that when the eruption is made by more than two standard deviations from the established rules, they should be considered as a delayed eruption. On careful analysis, it seems that late eruption according to Rasmussen coincides with late eruption according to Beck and Gron.
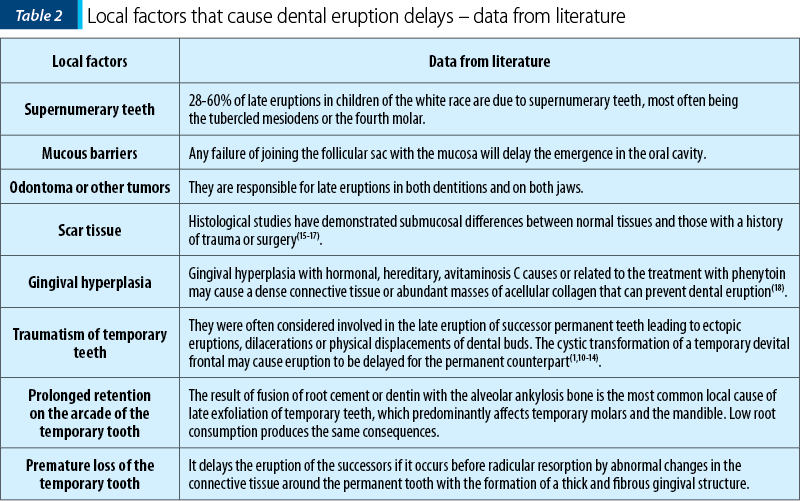
Local factors that cause dental eruption delays
These can be generated by: the presence of obstructions on the eruptive route, the persistence of temporary teeth over the normal exfoliation limit, the organization of an osteofibros cap over the successive tooth following the loss of the corresponding temporary tooth, more than 2-3 years prior to the normal exfoliation moment, abnormal positions of the germs of permanent teeth according to Table 2.
Smitt and Rapp conducted a cephalometric study and demonstrated that there was a bone-gap of up to 3 mm between the temporary and permanent upper central incisors, which was maintained during development(19).
Delayed eruption is often reported in patients with nutritional deficiency, as the major metabolic demand for growing tissues also influences the eruptive process. Endocrine gland disruptions (hypothyroidism, hypopituitarism, true or false hypoparathyroidism) have profound effects on the entire body including dentition. Permanent teeth have significant delays of approximately three months in dental maturation and eruption in children with birth weight below 1500 grams or with periods of gestation under 30 weeks(23,24). There are over 70 genetic syndromes that delay dental eruption(1).
Clinical implications
The correct diagnosis of the eruption delay is an important and complicated process. If the permanent tooth does not erupt with standard deviations after the expected age, careful assessment is needed to establish the diagnosis and the formulation of a treatment plan. The patient’s medical history is of utmost importance because there are numerous systemic or hereditary disorders associated with delayed eruption and abnormal intrafamilial eruption patterns must be carefully identified(1,26). Although syndromes are relatively easy to detect, clinical examination should be methodical and concentric.
The clinician should identify, by inspection and palpation, the pathology of soft tissues, scarring, swelling, fibrous and dense insertions of the frenula. The clinical examination and palpation of the vestibular and oral dento-alveolar ridges show characteristic deformities, pain, crepitation in the temporal teeth area that stagnate over the normal exfoliation time and mean age in the tables (Schour and Massler, Nolla, Moorees)(20-23).
Orthopanthomography is ideal for assessing the presence of teeth and developmental stages by estimating the moment of emergence of the permanent tooth in the oral cavity. Double radiographs using the Clark Parallax method are useful in identifying tumors, supernumeraries, and ectopias. Computed tomography can identify local pathology, bone density and bone quality at a higher cost and higher irradiation. Sometimes obstructions responsible for eruption delays are not visible on radiographs such as soft tissue barriers, but supernumeraries, tumors, cysts and bone seizures can be easily identified radiologically.
Aim of the study
-
Review of terminology and pathogenesis of dental eruption.
-
Identifying the causes of delayed eruption by clinical and radiological analysis.
-
Dental age identification using the Demirjian index.
Materials and method
The study was conducted in a private practice office in the urban area (Bucharest) on a group of 115 patients with delayed local eruption. The clinical data were collected by two examiners who examined 115 children wth late eruption, in the same time period (2018, within six months), and they evaluated their orthopantomographies, photographs and their study patterns.
The waistline, weight, date of birth, age in years and months, intrafamily history of dental eruption, dental and general history were recorded.
Using the orthopantomographies of the patients selected for the study, they calculated the Demirjian index for the reference teeth: the lower left canine (33), the first left inferior premolar (34), the second lower left premolar (35) and the second lower left molar (37), their mean age of eruption; root formation, physical obstacles on the eruption pathway, and the position of dental buds were assessed.
Determination of dental age
Knowledge of dental age is important for both the orthodontist for the assessment of the optimal age of treatment, as well as for the pedodont for a tooth during treatment. Dental age is calculated by appreciating the main moments of teeth formation in relation to age when they occur. Various radiographic methods of dental age determination have been reported, depending on the degree of dental mineralization. Of these, the most widespread method has been described by Demirjian et al. in 1973, in French-Canadian children. The Demirjian method is based on the development of seven permanent left mandibular teeth. Eight development stages (A to H) were determined, from the mineralization of the cuspidar tip to the apex closure for each tooth. Its system of dental maturity scores provides a universal application, which is why we have also used it in this study.
The statistical analysis used the T student test and the frequency analysis was performed using the SPSS 13.00 software.
The study group
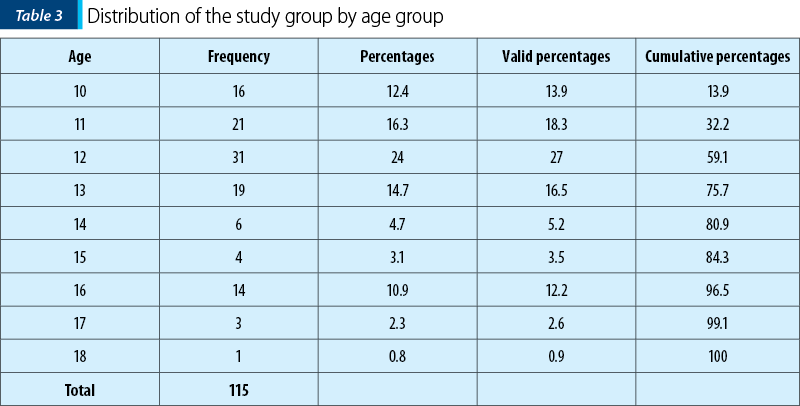
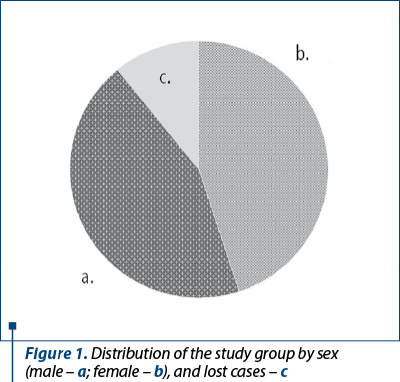
The study group consists of 151 patients (57 boys and 58 girls), aged 10-18 years old, clinically and radiologically monitored for one year. The distribution of the study group does not indicate significant gender differences. The distribution of the study group by age group indicates an average age of 12.58 years old, with a heterogeneous distribution (Figure 1, Table 3).
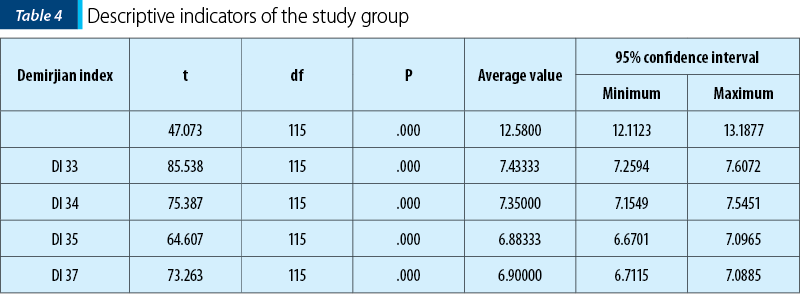
The statistical descriptors of the study group indicate an average age of 12.58 years old, mean Demirjian indices of 7.43 for the lower canine (33), 7.35 for the first mandibular premolar (34), 6.88 for the second mandibular premolar (35), and 6.9 for the second permanent mandibular molar (37) – Table 4.
Clinical cases
From our study, we present some clinical cases in which the diagnosis of delayed local eruption was formulated, by the malposition of the permanent tooth, the presence of supernumeraries, blockage on the eruption path of a permanent molar, or by the insufficient root development of dental buds.
Case 1
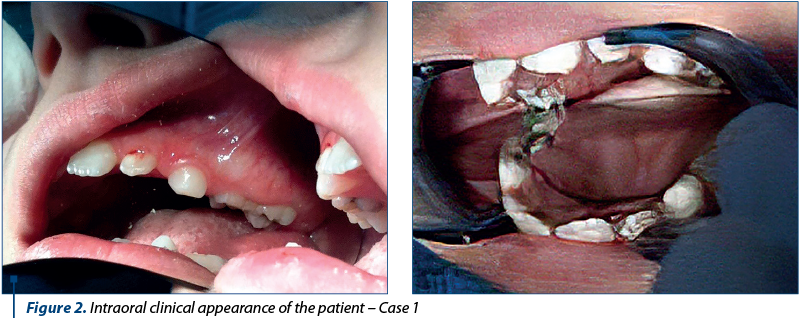
In the case of the first 8-year-old patient, with the absence of the first upper right molar (16) from the arcade, a bone conjugation is clinically observed in the lateral area of quadrant 1, the swollen area showing pain at vestibular palpation and being palatal depressed (Figure 2a and 2b).
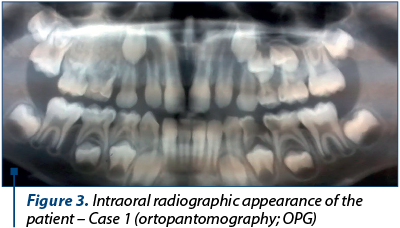
Radiologically (Figure 3), the normal position of 16 and the mass of dense bone which extends into the jaw sinus, accompanied by the anodontia of the first (14) and the second upper premolar (15) are observed.
Case 2
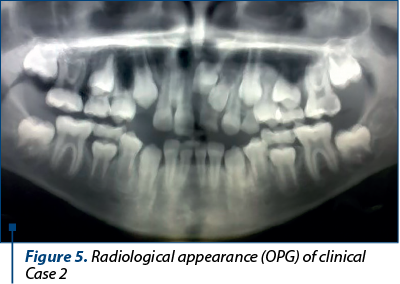
The second patient, aged 9 years and 3 months old, was diagnosed with late eruption in the left upper central incisor (21), with the presence on the eruptive route of a supernumerary tooth that was radiologically exposed.
Clinically, there was an arcade presence of the bigeminal temporary upper left central incisor (61) (Figure 4a and 4b).
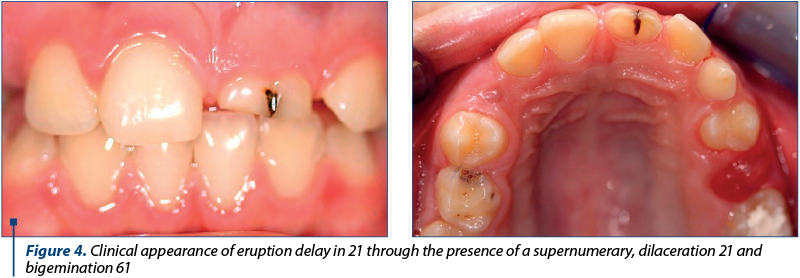
Radiologically, there is another factor that will slow or even prevent eruption, namely cervical dilaceration of the upper left central incisor (21) – Figure 5.
Case 3
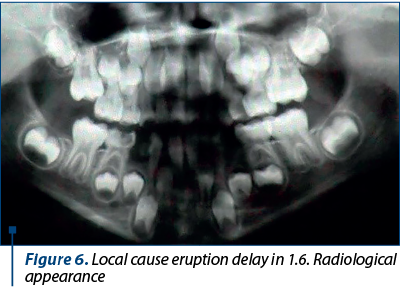
In a 7-year-and-6-month-old patient diagnosed with eruption delay in the first upper right molar (16), there were observed mesial-version and blocking of the eruption under the cervical convexity of the second upper right temporary molar (55), on an arcade with mixed teeth with less available space than required in the lateral area (Figure 6).
Case 4
In the case of an 11-year-old patient, the absence of the first right lower premolar (44) and of the second right lower premolar (45) from the arch was clinically observed. Radiologically, the development difference between 44 and 34 was observed, 44 being hypodeveloped compared to 34 after the early loss of the corresponding temporary tooth and the formation of an overlying osteofibrosis cap (Figure 5).
Eruption variations are more common in permanent teeth, where the literature records the lowest eruption delay (+/- 0.5 years) at the lower front teeth and the highest eruption delay in canines, premolars and the permanent second molars (+/- 1.5 years).
Our study and the clinical cases presented support the data published by the working group of the Pediatric Dentistry Association(25). There is no absolute therapeutic treatment in eruption delays.
In order to remove physical obstacles along the eruption path of permanent teeth, surgical approach by gingivectomy, apical flap surgery and orthodontic tractions are recommended – it takes an average of 18 months for the tooth to erupt(1,15,16,26). Sometimes getting the space required by orthodontic treatment is sufficient to resume eruption(1,26).
Results and discussion
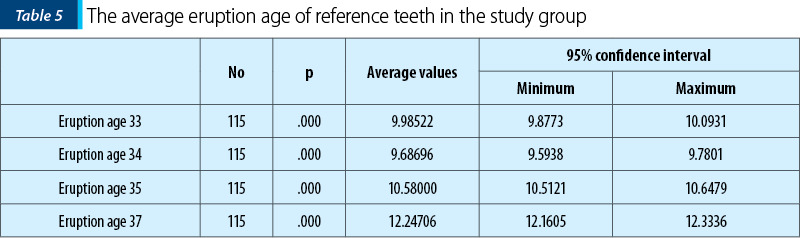
There was no significant difference in gender distribution. In general, specialized literature reports that dental eruption is earlier in girls, delayed in boys, and the intermediate period between consecutive eruptions is higher in boys. As in Ogodescu’s study(2-4), the lower canine (33) erupts at 9.98 years of age, a different moment from the existing national standards, but similar to the current standards of AAPD and EAPD, after the first premolar (34) and sometimes even after the second premolar (35) – as it can be seen from the values calculated by us (Table 5)(1,25).
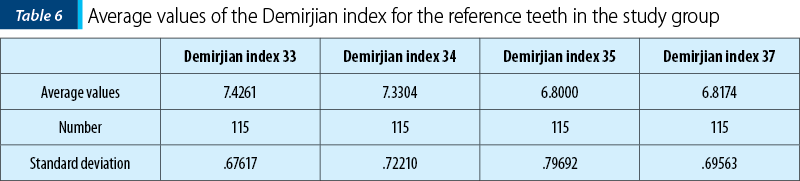
The mean values of the Demirjian index calculated for reference teeth 33, 34, 35 and 37 are presented in Table 5. For the inferior canine, the mean value of the Demirjian index is 7.43, with a standard deviation of 0.67. The Demirjian index has a mean of 7.33 for the first premolar, lower than the mean value of the canine, but very close to what indicates the possibility that the first premolar erupts before the canine, as in Ogodescu’s study(2-4).
The Demirjian index calculated for the second lower premolar has an average value of 6.8, with a standard deviation of 0.79. For the second mandibular molar, the calculated Demirjian index has the smallest mean value of the batch of 6.81, close to the values calculated for the second premolar, indicating an almost synchronous development and a concomitant eruption (Table 6).
Conclusions
1. The importance of delayed eruption as a clinical problem is present in numerous scientific publications that reflect many controversies over the terminology used, the pathogenesis of this unique developmental process in the body, and the reporting to standards derived from population studies.
2. In practice, however, dentists and pediatricians observe significant deviations from accepted norms; most commonly occurring is the delayed eruption – which may be the first or the only manifestation of a local or systemic pathology and which can affect the accuracy of diagnosis, the planning of prophylactic or pedodontic treatment, as well as the timing of the orthodontic treatment, with significant impact on the general health status of the child.
3. The variations in the normal eruption of the permanent teeth are a clinical issue commonly encountered in dental practices.
4. Significant deviations from established population norms alert clinicians and compel them to further investigate the health status and patient development.
5. The advantage of using chronological eruption rules is related to their ease of use.
6. Delayed eruption may be an alarm for a systemic illness or an indicator for an altered physiology of the craniofacial complex.
7. A clinical indication of local cause delayed eruptions is to overcome the average age of eruption by two standard deviations.
8. The radiological examination confirms and determines the cause of the eruption delay of these permanent teeth.
9. The necessity of periodic clinical and radiological checks to detect these cases and solve them so that they do not eventually lead to more severe dento-maxillary development disorders, with severe repercussions on dental occlusion, is underlined.
10. Orthodontists, dento-alveolar surgeons and pediatricians will be consulted in case of delayed eruptions for an early and comprehensive assessment of craniofacial structures.
11. Consideration of new (updated) standards for children in Romania is important for prophylactic, pedodontic and orthodontic treatment.
Compliance with ethics requirements:
The authors declare no conflict of interests regarding this article. The authors declare that all the procedures and experiments of this study respect the ethical standards of the Helsinki Declaration from 1975, as revised in 2008, as well as the national law. The informed consent was obtained from the patients included in the study. No funding for this study.
Bibliografie
- Suri L, Gagari E, Vastardis H. Delayed tooth eruption: Pathogenesis, diagnosis, and treatment. A literature review. American Journal of Orthodontics and Dentofacial Orthopedics. 2004; Volume 126, Number 4.
- Ogodescu AE, Tudor A, Szabo K, Daescu C, Bratu E, Ogodescu A. Up-to-date standards of permanent tooth eruption in Romanian children. Jurnalul pediatrului. 2011 Jan-Jun, vol. XIV, nr. 53-54.
- Bratu E, Ovidiu G, Voinea C. Erupţia dentară normală şi patologică. Editura Helicon Timişoara. 1996; 146.
- Ogodescu AE, Bratu E, Ogodescu AS. Importanţa actualizării standardelor de creştere şi dezvoltare a sistemului stomatognat. Timişoara Medical Journal. 2009; 59(1):111.
- Nichifor M, Scutariu M, Mocanu C, Crauciuc E, Ungureanu E, Toma O, Scutariu M. Study regarding the sequence of eruption of permanent teeth in a group of children from Buzău. Sci Ann of “Al. I. Cuza” Univ. Iaşi, Series Mol Genet Biol. 2011. 12: 85-94.
- Gron AM. Prediction of tooth emergence. J Dent Res. 1962; 41:573-85.
- Becker A. The orthodontic treatment of impacted teeth. London: Martin Dunitz; 1998.
- Rasmussen P, Kotsaki A. Inherited retarded eruption in the permanent dentition. J Clin Pediatr Dent. 1997; 21:205-11.
- Proffit WR, Vig KW. Primary failure of eruption: a possible cause of posterior open-bite. Am J Orthod. 1981; 80:173-90.
- Brin I, Ben-Bassat Y, Zilberman Y, Fuks A. Effect of trauma to the primary incisors on the alignment of their permanent successors in Israelis. Community Dent Oral Epidemiol. 1988; 16:104-8.
- Hawes RR. Traumatized primary teeth. Dent Clin North Am. 1966; 391-404.
- Andreasen JO, Sundstrom B, Ravn JJ. The effect of traumatic injuries to primary teeth on their permanent successors. I. A clinical and histologic study of 117 injured permanent teeth. Scand J Dent Res. 1971; 79:219-83.
- Ravn JJ. Sequelae of acute mechanical traumata in the primary dentition. A clinical study. J Dent Child. 1968; 35:281-9.
- Odersjö ML, Robertson A, Koch G. Incidence of dental traumatic injuries in children 0-4 years of age: a prospective study based on parental reporting, European Archives of Paediatric Dentistry, 10.1007/s40368-018-0334-z, 19, 2, (107-111), (2018).
- Di Biase DD. Mucous membrane and delayed eruption. Dent Pract Dent Rec. 1971; 21:241-50.
- Di Biase DD. Mucous membrane and delayed eruption. Trans Br Soc Study Orthod. 1969; 5:149-58.
- Goho C. Delayed eruption due to overlying fibrous connective tissue. ASDC J Dent Child. 1987; 54:359-60.
- Katz J, Guelmann M, Barak S. Hereditary gingival fibromatosis with distinct dental, skeletal and developmental abnormalities. Pediatr Dent. 2002; 24:253-6.
- Smith RJ, Rapp R. A cephalometric study of the developmental relationship between primary and permanent maxillary central incisor teeth. ASDC J Dent Child. 1980; 47:36-41.
- Schour I, Massler M. The development of the human dentition. J Am Dent Assoc. 1941; 28:1153-60.
- Nolla CM. The development of the human dentition. ASDC J Dent Child. 1960; 27:254-66.
- Moorrees CFA, Fanning EA, Hunt EEJ. Age variation of formation stages for ten permanent teeth. J Dent Res. 1963; 42:1490-502.2
- Seow WK. Effects of preterm birth on oral growth and development. Aust Dent J. 1997; 42:85-91.
- Seow WK. A study of the development of the permanent dentition in very low birthweight children. Pediatr Dent. 1996; 18:379-84.
- Ukpong M. Eruption and eruption disorders. Working group EAPD.
- Taha SEE, El-Yazeed AM, Wael Abou-Zeid AW. Eruption dates of primary and permanent teeth among a group of Egyptian children. Review of Research Journal. 2018; vol 7, no. 9.
Articole din ediţiile anterioare
Consideraţii diagnostice în cazul unui sindrom Guillain-Barré
Autorii prezintă un caz clinic de debut al sindromului Guillain-Barré, mimând perfect simptomatologia unei infecții respiratorii acute, în particul...
Lichenul plan oral. Actualităţi în sfera etiologiei şi patogenezei
Lichenul plan oral are o prevalenţă şi o incidenţă variată. Au fost evidenţiate în literatura de specialitate şase tipuri distincte de lichen plan ...
Defecte congenitale severe la copiii expuşi vertical la infecţia HIV. Serie de cazuri
Tratamentul antiretroviral reprezintă piatra de temelie pentru o mai bună calitate a vieţii şi pentru prevenirea transmiterii infecţiei HIV. Este î...
Consideraţii epidemiologice şi corelaţia cu complicaţiile gripei la copii în sezonul 2016-2017
Pe parcursul epidemiei de gripă din sezonul 2016-2017 mulţi pacienţi pediatrici au necesitat internare pentru complicaţiile gripei, în special cele...