Haemangiomas are vascular tumours rarely found in the otorhinolaryngological practice, especially in adults. We present the case of a 31-year-old female patient, accusing oral haemorrhage and mild dysphagia. Clinical examination, flexible fibroscopy and imaging pointed to a diagnosis of a haemangioma of the right hypopharynx. A microscopic laryngoscopy procedure was carried out, with intratumoral monopolar electrocauterization which led to a complete retraction of the tumour. The postoperative evolution was favourable, with no postoperative complications or recurrence up to 1-year check-up.
FARINGOLOGIE
Hemangiomul faringian – caz clinic
Pharyngeal haemangioma – case report
M. Chițac,
Celesta Drăgulescu,
B. Petrescu,
Alexandru Ciucă,
M. Vasilca,
A. Weisman,
Cătălina Sandu,
Ioana Dumitrescu,
Floriana Stăncescu,
Romeo Călărașu
First published: 23 mai 2018
Editorial Group: MEDICHUB MEDIA
DOI: 10.26416/Orl.39.2.2018.1722
Abstract
Rezumat
Autorii prezintă cazul unei paciente în vârstă de 31 de ani care se internează în clinica noastră pentru sângerare exteriorizată oral şi disfagie uşoară. Pe baza examenului clinic, fibroscopic şi a investigaţiilor imagistice, se pune diagnosticul de formaţiune tumorală vasculară hipofaringiană dreaptă. Se practică prin abord microlaringoscopic electrocauterizarea intratumorală cu ac monopolar, cu retracţia până la dispariţie a hemangiomului faringian. Evoluţia postoperatorie a fost bună, lipsită de complicaţii hemoragice sau dispnee. Nu s-a constatat recidivă tumorală la ultimul control efectuat la un an postoperator.
Case report
Haemangiomas are benign tumours originating in the vascular endothelium. They represent a type of tumour rarely encountered in clinical practice, especially in the pharynx, with a small number of cases cited in literature. The treatment represents a challenge, as there is no agreed-upon standard, due to the rarity of the disease, the variable clinical aspect, and the location of the tumour.
A 31-year-old woman consulted our clinic, accusing two episodes of oral haemorrhage, in moderate quantity, which ceased spontaneously, and mild dysphagia, all occurring in the last month. She had no record of other significant illness of herself or her family. She is a smoker and works as a clinical nurse.
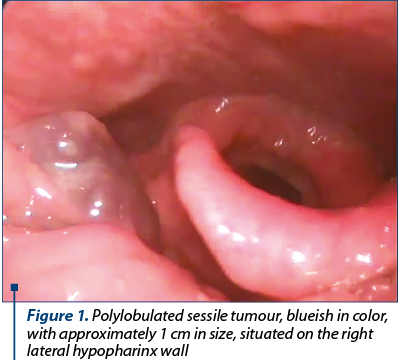
The physical examination and naso-pharyngeal-laryngeal fibroscopic examination revealed a polylobate sessile blueish tumour, approximately 1 cm in size, located in the right lateral hypopharyngeal wall, extending from the lower edge of the tonsil to the aryepiglottic fold (Figure 1). No abnormalities were found in the larynx.
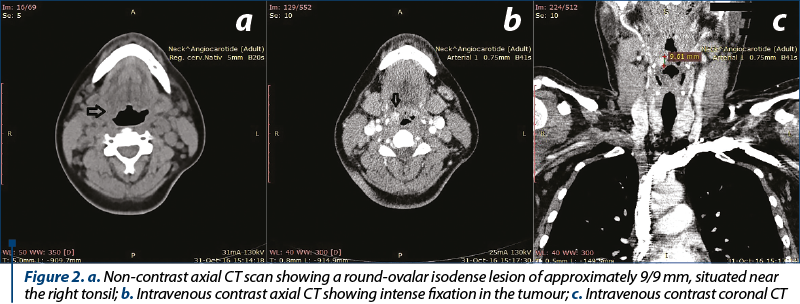
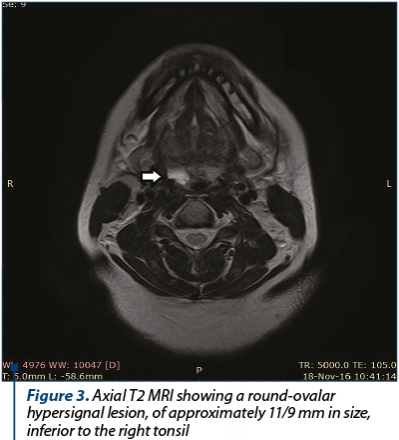
Laboratory tests revealed no signs of anaemia or other pathological findings. Computerized tomography (CT) of the cervical region described a round-ovular isodense lesion on native sequences, with approximately 9/9 mm in size, adjacent to the right tonsil, with a subsequent reduction of the ipsilateral piriform sinus. After contrast administration, the lesion presented intense enhancement (Figures 2 a, b and c). For a better description of the tumour, a magnetic resonance imaging (MRI) was performed, which showed a round-ovalar lesion, 11/9 cm in size, below the level of the right tonsil, with a T2 hyperintense signal and intense contrast enhancement on arterial phase (Figure 3). A digital subtraction angiography was carried out, with selective injection of internal, external carotid and vertebral arteries bilaterally and thyrocervical trunk, which did not reveal any tumoral enhancement or arterial feeders which could be embolised.
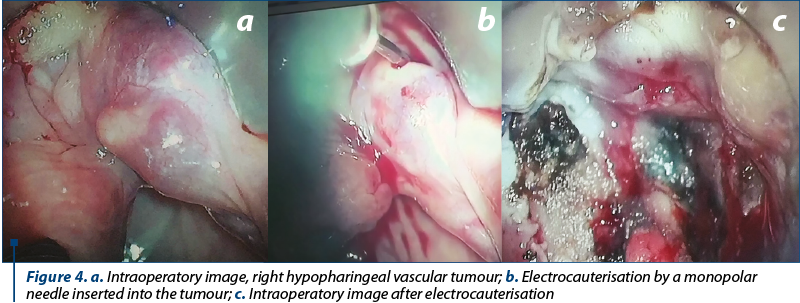
Based on this evidence, we made the diagnosis of haemangioma of the right hypopharynx. A surgical approach under general anaesthesia was decided upon. Through microscope-aided direct laryngoscopy, electrocauterization is applied via a monopolar needle inserted into the tumour, until complete retraction of the tumour is achieved (Figures 4 a, b and c). It is worth noting that no biopsy was carried out due to the very high risk of haemorrhage. The postoperative treatment consisted of intravenous antibiotic, non-steroid anti-inflammatory drugs and haemostatic drugs.
In the postoperative period, there weren’t noted any complications, such as bleeding, dyspnoea or dysphagia.
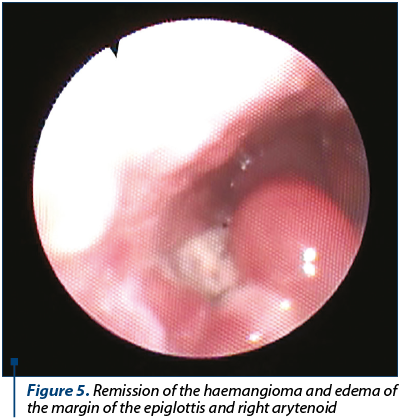
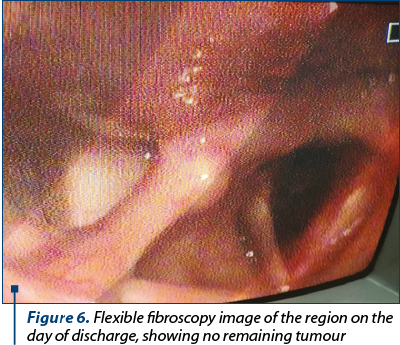
Next-day fibroscopic examination showed the complete remission of the vascular tumour and the presence of oedema of the right margin of the epiglottis and the right arytenoid, which diminished in the following days (Figure 5). The patient was discharged 9 days after the procedure. Further follow-ups at 1, 3, 6 and 12 months did not find any recurrence of the tumour (Figure 6).
Discussion
Haemangiomas are a class of benign tumours of vascular origin. They mostly develop in infants, with an incidence of 2.5% in the first year. Despite this, they are rarely present at the moment of birth. They are found more often in people of Caucasian descent, with a 3-5:1 ratio of females to males. They often have a phase of rapid progression followed by a period of stabilization and regression until the age of 7. Haemangiomas are found much less often in adult life and they have a different evolution, with progressive growth and no spontaneous involution. 60% of cases are situated on the skin and subcutaneous tissue of the head and neck. Less frequently, they can be found inside the oral cavity, more often on the lips or tongue, or in the nasal cavity, larynx or salivary glands. Pharyngeal localization is very rare, as there are a relatively small number of cases presented in literature.
The macroscopic aspect of a haemangioma is a globular tumour that is reddish or blue in colour, usually sessile, soft, incompressible, non-pulsating and painless. Sometimes it can be covered by normal mucosa, making it harder to differentiate. Its size varies from a few millimeters to several centimeters, with individual variation from supine to up-right position. Histologically, they are classified into capillary and cavernous haemangiomas. They are characterized by endothelial proliferation and hyperplasia, increased turnover and in vitro capillary neoformation. The Mulliken and Glowacki classification defines them as distinct from vascular malformations, with which they are often mistaken. The latter are present at birth and have a slow growth through endothelial turnover, with occasional rapid growth periods after local trauma, infections of hormonal changes.
The clinical presentation is very variable, as it depends on the tumour’s size and location. Haemangiomas of the head and neck can be clinically silent and found during routine investigations or they may cause symptoms ranging from foreign body sensation in the oral cavity or throat, nasal obstruction, hearing impairment, dysphagia, dysphonia, up to severe dyspnoea, congestive heart failure or coagulopathy (Kasabach-Merrit syndrome). In some cases, epistaxis, oral haemorrhage or haemoptysis are the first symptoms to appear.
Imaging procedures are crucial for the diagnosis of haemangiomas. A fibroscopic examination offers important information about the location and aspect of the tumour, but it cannot be used to estimate its extension. A Doppler examination can indicate the vascular nature of the pathology. Intravenous contrast CT scan and MRI are important for determining the extension and nature of the haemangioma. MRI typically describes a lobulated, heterogeneous lesion, with well-defined margins, with an intermediary signal in T1 and moderately-strong signal in T2, with intense signal enhancement after the administration of intravenous contrast agents. Digital subtraction angiography can be particularly useful, as it can determine the presence of vascular pedicles, and may be used for embolization as a stand-alone treatment or before surgery. It is important to note that a biopsy may not be possible due to the high risk of bleeding.
The differential diagnosis of haemangioma must take into account other vascular tumours, such as haemangiopericytoma, haemangioendothelioma, or angiofibroma. Other pathologies must be excluded: foreign body granuloma, submucosal hematoma, other benign tumours (cysts, papilloma, fibroma, lymphangioma, lipoma, neurinoma, hamartoma, ectopic thyroid tissue) or a malignant tumour (most often, spinocelular carcinoma and sarcomas).
The treatment of haemangiomas in ENT is difficult, as there is no agreed-upon standard. The decision depends on the patient’s age, the size and location of the tumour, and the symptoms it causes. Most haemangiomas do not require treatment and are simply monitored. The pharmaceutical treatment is possible in juvenile cases where corticosteroids can be administered or, more recently, beta-receptor blockers. Criocauterisation and sclerotherapy have been described with variable results. Embolization may be attempted if there is a suitable vascular pedicle.
Surgical treatment methods include electrocauterization or resection via CO2, Nd:YAG, or Argon laser. Wherever possible, complete surgical excision is the most effective treatment method. Choosing any method must take into account the risks during and after surgery that derive from the vascular nature of the tumour. Possible complications include tissue necrosis, infection, oedema or hematoma of the surrounding regions, which can lead to acute respiratory distress, early and late post operatory bleeding, with possible flooding of the airways. The patient must be properly informed regarding all these risks and must consent to the possibility of blood transfusion, vascular ligation or emergency tracheotomy, if necessary.
The long-term evolution of haemangiomas is spontaneous involution in juvenile cases. In adults who have suffered surgery, recurrence is possible after 3 to 6 months.
The particular findings in the case presented:
-
Very rare location of the tumour in an adult, at the pharyngeal level.
-
Oral haemorrhage was the reason for consultation and discovery of the pathology.
-
The diagnosis was based on imaging, instead of biopsy, due to the risk of bleeding close to the airways, which is difficult to control. Angiography was an important tool that described the haemangioma’s relation to the large vessels of the neck and the lack of any vascular branch that could be embolised.
-
The surgical treatment is unstandardized and was decided upon after taking into account the risks during and after surgery due to the proximity of large vessels and the airways.
-
Follow-up did not note any recurrence or complications up to the present date.
Conclusion
Haemangiomas are a class of benign vascular tumours, rare in the ENT speciality, especially in adult life, which may remain hidden until severe symptoms appear, such as bleeding, dysphagia or dyspnoea. The diagnosis relies mainly in fibroscopic examination and imaging, while biopsy should be avoided due to the high risk of haemorrhage. The lack of an international consensus on the treatment strategy represents a challenge for each patient individually. Choosing any method must take into account the natural progression of the disease, the risks of treatment and the evolution after treatment.
Conflict of interests: The authors declare no conflict of interests.
Bibliografie
- Sharifi A, Nazemieh M, Moghadaszadeh M. Supraglotic hemangioma as a rare cause of recurrent hemoptysis: A new treatment modality with Argon plasma coagulation. Tanaffos. 2014; 13(2): 50-52.
- Lechien JR et al. Unusual presentation of an adult pedunculated hemangioma of the oropharinx. Clin Case Rep. 2017; 5(4): 491-496.
- Khil EK et al. Nasopharyngeal hemangioma in adult: A case report. J Korean Soc Radiol. 2013; 68(5):391-395.
- Gangavati R et al. A review of hemangiomas of the oral cavity. UJMDS. 2015; 03 (04): 4-6.
- Anniko M, Bernal-Sprekelsen M, Bonkowsky V, Bradley P, Iurato S. Otorinolaringology. Head & Neck Surgery. Springer. 2009.
- Snow JB Jr, Ballenger JJ. Ballenger’s Otorhinolaryngology. Head and Neck Surgery, 16th edition. BC Decker. 2003.
- Hussain K, Makura ZGG. Pyriform sinus haemangioma: an unusual presentation of an unusual condition. JLO. 2011; 125(11):1196-1198.
Articole din ediţiile anterioare
PATOLOGIE CERVICALĂ | Ediţia 3 40 / 2018
Rezolvarea în echipă multidisciplinară a unei malformaţii arteriovenoase mandibulare la un copil de 13 ani – caz clinic
Daniela Vrînceanu, Bogdan Bănică, Matei Dumitru, Bogdan Dorobăț, Cristina Tudor, H. Mureşian
Malformaţia arteriovenoasă (MAV) este o conexiune anormală şi fragilă între artere şi vene, dintre ele lipsind capilarele, cu aspect de ghem vascul...
24 septembrie 2018
PATOLOGIE CERVICALĂ | Ediţia 2 35 / 2017
Hemangiom al venei jugulare interne
Daniel Mirea, Gabriela Popescu, Răducu Stănciulescu, Loredana Mitran, Răzvan Stănciulescu, Ștefăniță Dima, Raluca Ungureanu, Liliana Mirea
Hemangioamele venei jugulare interne sunt extrem de rar întâlnite, foarte puține cazuri fiind publicate în literatură. Autorii prezintă un caz de h...
07 iunie 2017
RHINOLOGY | Ediţia 3 52 / 2021
Particularităţi diagnostice, terapeutice şi anestezice în abordul tumorilor vasculare gigante nazosinuzale
Mihail Tuşaliu, Iulia Tiţă, Diana Tuas, Ruxandra Zarei, Cristian Bucur, Bădeanu Andreea
Tumorile vasculare ale capului şi gâtului constituie un grup heterogen de afecţiuni care ridică numeroase probleme în ceea ce priveşte diagnosticul...
30 septembrie 2021
RHINOLOGY | Ediţia 1 58 / 2023
Hemangiom mixt cavernos-capilar rinoetmoidal – rezecţie endoscopică transnazală. Prezentare de caz
Bogdan Mocanu, Silviu Oprescu, Cristina Bichir, Alexandru Mocanu
Hemangioamele sunt tumori vasculare benigne care îşi au originea în piele, mucoase şi structuri profunde precum oase, muşchi sau glande. Hemangio...
03 martie 2023