Larynx cancer in young pregnant women is very uncommon. The treatment modalities traditionally used for larynx cancer management may present high risk either for the mother or the fetus. A rational therapeutic approach (flexible endoscopic laser surgery), that allows avoiding the risk of radiation therapy and general anesthesia, is presented.
LARYNGOLOGY
Managementul endoscopic flexibil al unui carcinom glotic în stadiu iniţial la o gravidă tânără
Flexible endoscopic management of early glottic carcinoma in a young pregnant woman
First published: 09 aprilie 2021
Editorial Group: MEDICHUB MEDIA
DOI: 10.26416/ORL.51.2.2021.4942
Abstract
Rezumat
Cancerul laringian la femeile tinere însărcinate este foarte neobişnuit. Modalităţile de tratament utilizate în mod tradiţional pentru managementul cancerului laringian pot avea un risc mare, fie pentru mamă, fie pentru făt. Este prezentată o abordare terapeutică raţională (chirurgie laser cu endoscop flexibil), care permite evitarea riscurilor determinate de radioterapie şi anestezia generală.
Introduction
Larynx cancer in young women is uncommon. Larynx cancer in young pregnant women is even more uncommon. In the accessible English literature, we found only a few references covering therapeutic approaches in such cases(1-4). Radiotherapy is the most popular treatment modality for early glottic cancer, but it is an aggressive treatment for a pregnant woman, that results in the interruption of pregnancy, which is too traumatic for a woman, especially when performed at late term.
Conservation open surgery or endoscopic laser surgery that can serve as an alternative to radiotherapy with comparable local control rates are related to using general anesthesia which, in its turn, can be considered a negative factor for the evolution of pregnancy.
A rational therapeutic approach that allows avoiding the risk of radiation therapy and general anesthesia is presented.
Case report
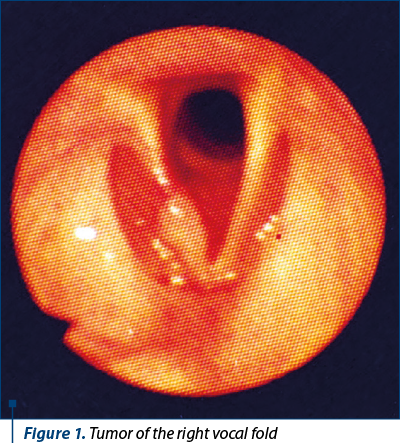
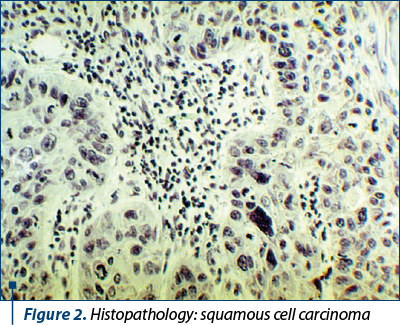
A 27-year-old pregnant woman (20 weeks) came to the “Timofei Moşneaga” Republican Clinical Hospital, from Chişinău, Republic of Moldova, on April 30, 1996, due to a twelve-month history of moderate progressive hoarseness. The patient was a nonsmoker. Fiberlaryngoscopy demonstrated an exophytic tuberous tumor with rose-colored surface affecting the anterior two thirds of the right vocal fold (Figure 1). The biopsy of the tumor was performed. The histologic exam revealed squamous cell carcinoma (Figure 2). No evidence of cervical lymphadenopathy was found either by palpation or by ultrasound. Taking into consideration the pregnancy and the limited tumor extension (T1aN0M0), the endoscopic management of the tumor was proposed as the method of choice. The informed consent was obtained from the patient.
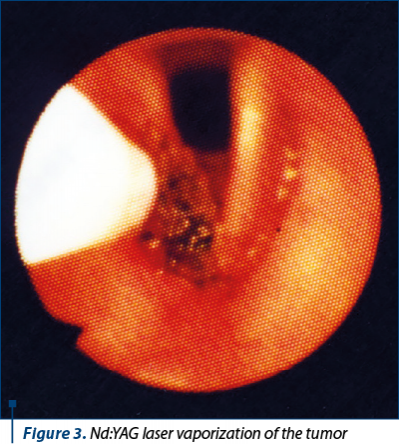
The photovaporization of the tumor was performed with Nd:YAG laser (40 W) under local anesthesia with 2% lidocaine hydrochloride in sitting position, the laser guide being introduced through the working channel of fiberbronchoscope (Olympus, BF1T10) inserted transnasally in order to obtain a good exposure of the lesion (Figure 3). Intramuscular premedication with diazepam (10 mg) and atropine (0.3 mg) was additionally used.
Six days later, after multiple control biopsy from the margins and the bottom of the tissue defect following photovaporization, the second session of laser vaporization in the limits of visual intact tissues was performed.
The patient was discharged from the hospital after six days. The histologic exam didn’t reveal tumor elements in control biopsy specimens.
Twenty weeks later, the patient gave birth to a baby (boy, 4 kg weight).
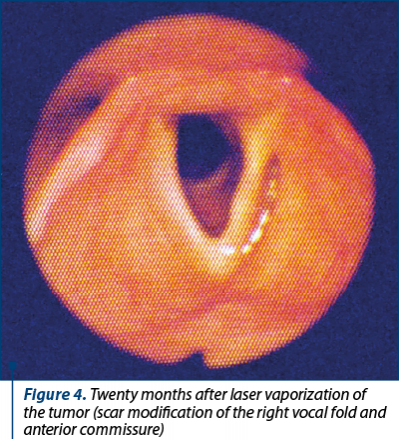
The follow-up exam took place at one year and eight months after operation. The voice had almost restored (only mild hoarseness was persisting). No other complaints were presented. The child was 15 months old. The development of the child was normal. No evidence of cervical lymphadenopathy was found either by palpation or by ultrasound. Fiberlaryngoscopy didn’t reveal any evidence of recurrence of laryngeal tumor (Figure 4).
A telephonic conversation with the patient took place 9 years and 7 months after operation. The patient felt OK. The voice was normal. No additional complaints were presented.
Discussion
The diagnosis of laryngeal carcinoma during pregnancy puts clinicians into a dilemma with respect to choosing the optimal treatment strategy. Some of the therapeutic modalities accepted for the management of early glottic carcinoma cannot be implemented during pregnancy because of the high risk of fetal complications. On the other hand, postponing cancer treatment for the period after delivery would mean exposing mother’s life to a high risk, especially if cancer is diagnosed at an early period of gestation. The decisions about choosing the optimal treatment modality for the mother are very difficult because two lives are involved and any intervention may have direct consequences for the fetus. Different types of laryngectomy are mostly considered as a solution in such cases(2-4).
In the accessible English literature, we have found only one article dedicated to fiberendoscopic laser surgery of early glottic carcinoma(5), and no references concerning the fiberendoscopic approach in the treatment of glottic carcinoma in a pregnant woman.
Flexible endoscopic laser surgery is a method that allows the complete eradication of the tumor, at the same time avoiding the risk for pregnancy related to radiation therapy and general anesthesia. The impossibility of the histologic exam of the margins of resected specimen is a drawback of the technique, that can be compensated, in a way, by multiple biopsies from the margins and the bottom of the tissue defect, following photovaporization and close follow-up at short time intervals that allows the early detection of recurrence.
Conclusions
The results obtained demonstrate that fiberendoscopic laser vaporization under local anesthesia can be recommended as a method of choice in the treatment of early glottic carcinoma in pregnant women in selected cases. The follow-up exams at short-time intervals are critical for the early detection of recurrence.
Bibliografie
-
Bradley PJ, Raghavan U. Cancers presenting in the head and neck during pregnancy. Curr Opin Otolaryngol Head Neck Surg. 2004;12(2):76-81.
-
Pytel J, Gerlinger I, Arany A. Twin pregnancy following in vitro fertilisation coinciding with laryngeal cancer. ORL J Otorhinolaryngol Relat Spec. 1995;57(4):232-4.
-
Ferlito A, Nicolai P. Laryngeal cancer in pregnancy. Acta Otorhinolaryngol Belg. 1980;34(6):706-9.
-
Matschke RG, Graber T, Panagiotopoulos A. A laryngeal cancer in pregnancy. HNO. 1994;42(8):505-8.
-
Lai JP, Tao ZD, Xiao JY, et al. Microinvasive Nd:YAG laser therapy of early glottic carcinoma and its effect on soluble interleukin-2 receptor, interleukin-2, and natural killer cells. Laryngoscope. 2001;111(9):1585-8.