Internal root resorption is a rare pulp disease characterized by loss of dentine due to the action of multiclastic cells stimulated by pulpal inflammation. Internal resorption can be detected earlier by chance when it is located within the pulp space, or later, when the invasion of the cementum has begun. In earlier stages, root canal treatment remains the treatment of choice, removing the granulation tissue and filling the root using warm gutta-percha by thermoplastic technique. When perforation of the root occurs, other methods, such as surgery techniques or even removing the tooth, are recommended.
INTERDISCIPLINARY
Managementul resorbţiei radiculare interne – prezentare de caz
Management of internal root resorption – clinical case report
Sânziana Scărlătescu,
Irina-Maria Gheorghiu,
Loredana Mitran,
Cristian Mitran,
Ioana Suciu,
George Nicola,
Paula Perlea,
Dr. Alexandru Iliescu
First published: 27 mai 2022
Editorial Group: MEDICHUB MEDIA
DOI: 10.26416/ORL.55.2.2022.6499
Abstract
Rezumat
Resorbţia radiculară internă este o afecţiune pulpară rară, caracterizată prin pierderea de dentină din cauza acţiunii celulelor multinucleate, stimulate de inflamaţia pulpară. Resorbţia internă poate fi detectată în fazele precoce din întâmplare, când este localizată în interiorul spaţiului pulpar, sau în fazele tardive, atunci când invazia cementului a început. În fazele iniţiale, tratamentul de elecţie este cel endodontic, cu îndepărtarea ţesutului de granulaţie şi obturaţie de canal, folosind gutapercă încălzită şi tehnici termoplastice. Când perforaţia rădăcinii a avut loc, alte metode, precum tehnicile chirurgicale sau chiar extracţia dintelui, sunt recomandate.
Introduction
The pulp canal is a soft tissue containing a pool of cells, most of which are fibroblasts, blood vessels and nerfs. The pulp is totally surrounded by a hard tissue (dentin) and therefore having a low ability to tolerate edema. Also, its poor collateral circulation limits the ability to cope with bacteria and inflammation. In spite of these circumstances, pulp tissue has some capacity to recover, but the degree is uncertain. So, the pulp cells can differentiate into hard-tissue-secreting cells in an attempt to form dentin and irritation dentin to protect from injuries(1).
In certain inflammatory conditions, the opposite response to formation of dentin may occur. This response is due to the presence of infected necrotic tissue in conjunction with injury to the periodontal ligament. It occurs with luxation injuries and replanted teeth as well(2,3). The phenomenon is called inflammatory resorption and is characterized by loss of tooth structure and sometimes adjacent alveolar bone.
This process is insidious, usually asymptomatic and identifiable only on radiographs until the lesion has progressed to the canal wall and perforated it. Sometimes it is impossible to say if the resorption is internal or originally external of the root canal.
External resorption begins in the periodontium space and affects the external surface of the tooth. It may or may not invade the dental pulp space(4). Internal resorption is a process that begins within the pulp space and affects the dentine and sometimes invades the cementum(4).
Internal resorption may begin in the root canal (Figure 1) or in the pulp chamber (Figure 2).


Internal resorption frequently occurs in inflamed pulps. The precise etiology is unknown, but it is related to a history of trauma, maybe a blow or restorative procedures that can lead to pulpitis due to the presence of bacteria(5).
Internal resorption appears when multinucleated giant cells named dentinoclasts resorb dentin and that loss is replaced by chronic inflammatory tissue or occasionally by apposition of hard, bone-like tissue. Clinical, a pink area through the enamel can be seen, that means an irreversible pulpitis occurred and root canal treatment is therefore recommended until the perforation of the canal wall may happen. The lesion can be seen on radiographs as a radiotransparent and uniform area, that enlarges the coronal or radicular part of the tooth. Also, the use of CBCT is highly recommended for a more accurate diagnosis of internal root resorption(6).
Internal resorption is considered to be rare in permanent tooth. It seems that external resorption is much more common and is often misdiagnosed as internal resorption(7). In active internal resorption, the coronal portion of the pulp is often necrotic, whereas the apical part remains vital.
Endodontic treatment
The treatment must remove the blood supply to the dentinoclastic cells of the inflammatory tissue. After anesthesia, the root canal is inspected and the working length short of the radiographic apex is established. The root canal instrumentation will cut off the blood supply to the tissue resorbing and the canal can be flushed with irrigants and then dried with paper point. A calcium hydroxide inter-appointment paste is mandatory to facilitate the removal of the tissue in the defect. At the second visit, the root canal tooth and the resorption are filled using a soft filling technique(7). With this technique, gutta-percha is warmed and injected in the canal, providing an adequate seal. This technique is very useful in such special conditions as internal root resorption, in contrast to other techniques (cold lateral condensation)(8).
Clinical case number 1
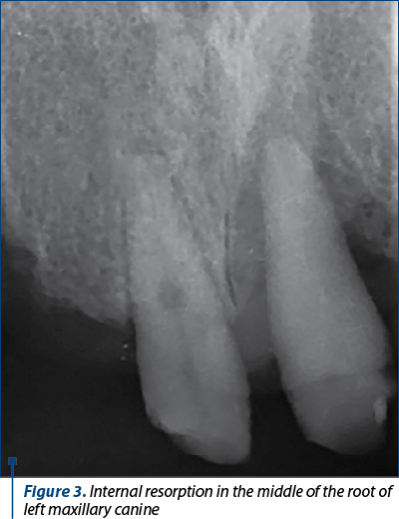
A healthy 65-year-old female presented to the dental office with a pain history of left maxillary canine. She had a total maxillary bridge, very old and incorrectly adapted. After cutting this bridge, a radiograph revealed a loss of internal tooth structure in the middle of the root, without any perforation (Figure 3). Actually, she was not in pain and no fistula was noted. Vertical and transversal percution on tooth 13 was negative.
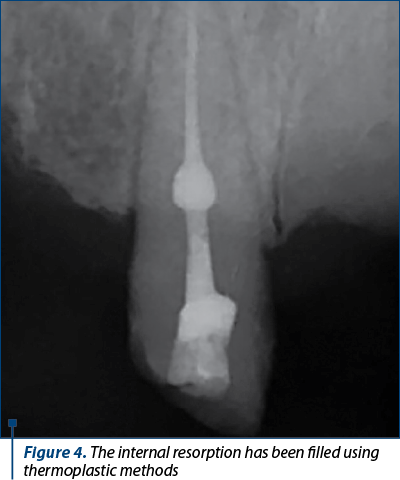
Internal root resorption diagnosis was established. The tooth underwent rotative treatment procedure using ProTaper Universal system till F3 instrument (30/09). After copious irrigation with 5.25% sodium hypochlorite and final ultrasonic irrigation using Irrisafe® (Acteon, Satelec), the tooth was filled in one session by continuous wave of condensation using System B® (SybronEndo). In the down-pack stage a master F3 gutta-percha cone was used till the internal resorption defect, whereas the defect was filled with System B® gun in the back-fill stage (Figure 4).
Finally, the patient is about to receive a new prosthetic restoration.
Clinical case number 2
A healthy 48-year-old female presented to the office with a complaint of a loose front incisor. The radiograph revealed significant loss of internal tooth structure in the middle of the root (Figure 5). The clinical exam revealed tooth perforation, probing depths of 6 mm, class III mobility. No fistula was noted.

The differential diagnosis of internal and external resorption was made. Internal tooth resorption was given based on the fact that the focal point of radiolucency was within the root canal area. Due to the extent of the perforation, it was recommended that the tooth be removed and other surgical and prosthetic restorative options be assessed.
Discussion
Internal root resorption is quite rarely observed in daily practice, in contrast to external resorption. Earlier radiographs could aid in early detection and more accurate and definite diagnosis can be given by the use of technology and CBCT scans(9).
The histologic picture of internal resorption is a granuloma with multinucleated cells. When the perforation does not occur and the lesion is found earlier, the conservative root canal treatment can be performed and the prognosis of the tooth is favorable.
The differential diagnosis between internal and external resorption is mandatory and sometimes they can be found together in the same tooth. It is important to note that, unlike the internal root resorption, the adjacent bone is affected with external root resorption(10).
Today we have a lot of modern techniques which can aid to treat teeth with internal resorption: the use of microscope, ultrasonic irrigation during the root canal instrumentation, thermoplastic filling techniques(11,12). In such conditions, the prognosis of this disease can be good.
Acknowledgements: All the authors have equal contributions for this article.
Conflicts of interests: The authors declare no conflict of interests.
Bibliografie
-
Simon JHS, Walton RE, Pashley DH, Dowden WE, Backland LK. Pulpal pathology. In: Ingle J, Backland L editors. Endodontics, 4th ed. Williams&Wilkins, Malvern PA; 1985: p.419, 430-433.
-
Backland LK, Flores MT. Management of traumatic dental injuries. In: Torabinejad M, Walton RE, editors. Endodontics: Principles and Practice. 4th ed. Sauders Co. St. Louis; 2009: p. 178.
-
de Souza BDM, Dutra KL, Reyes-Carmona J, Bortoluzzi EA, Kuntze MM, Teixeira CS, Porporatti AL, De Luca Canto G. Incidence of root resorption after concussion, subluxation, lateral luxation, intrusion, and extrusion: a systematic review. Clin Oral Investig. 2020 Mar;24(3):1101-1111.
-
American Association of Endodontics. Glossary of endodontic terms, 2014. www.aae.org/glossary.
-
Wedenberg C. Development and morphology of internal resorption of teeth – a study in humans, monkeys and rats. Kongl Carolinska Medico Chirurgiska Institutet, Stockholm, 1987.
-
Nilsson E, Bonte E, Bayet F, Lasfargues JJ. Management of internal root resorption on permanent teeth. Int J Dent. 2013;2013:929486. doi:10.1155/2013/929486.
-
Trope M. Endodontic considerations in dental trauma. In: Rotstein I, Ingle J,editors. Endodontics, vol. 1, 7th ed. Raleigh, North Carolina; p. 386, 387, 2019.
-
Scărlătescu SA, Iliescu A, Didilescu AC, Ştefan DS, Iliescu ALA. A comparative study of the root canal fillings based on warm gutta-percha condensation techniques. Int J of Romanian Dent. 2012;2:102-106.
-
Estrela C, Bueno MR, de Alencar AHG, et al. Method to evaluate inflammatory root resorption by using cone beam computed tomography. J Endod. 2009;35(11):1491–1497.
-
Gabor C, Tam E, Shen Y, Haapasalo M. Prevalence of internal inflammatory root resorption. J Endod. 2012;38(1):24–27.
-
Glickman GN, Walton RE. Obturation. In: Torabinejad M, Walton RE, editors. Endodontics: Principles and Practice. 4th ed. Sauders Co. St. Louis; 2009; p.315-318.
-
Deep A, Thakur S, Singhal P, Chawla D. Management of Root Perforation due to Internal Resorption: A 1-year Follow-up Study. Int J Clin Pediatr Dent. 2021 Jul-Aug;14(4):593-595.