The aim of this study is to determine the success rate of clinically and radiologically endodontic treatment in one session - a retrospective study (6 months - 2 years). Material and methods. Our research is based on a retrospective study performed in The Endodontics Department of the „Carol Davila” Faculty of Dentistry and in a private practice limited to Endodontics in Bucharest. Between the years of 2014-2015, taking out patients were initiated and completed nonsurgical root canal treatment in a single session. Clinically and radiographically analyzed cases (45) and on a reexamination - reconsideration time (6 months, 2 years) after that was decided the success or failure for each case. Results. The study was conducted on a total of 45 patients, out of which women (12%) had a higher failure rate comparable to men (6%); these differences are not statistically significant because female patients were presented at reevaluation in higher rate than men did. Conclusions. Most of selected asymptomatic cases with or without periapical pathology have been successful after a single visit endodontic treatment.
One session endodontic treatment
Tratamentul endodontic într-o singură şedinţă
First published: 15 noiembrie 2015
Editorial Group: MEDICHUB MEDIA
Abstract
Rezumat
Scopul acestui studiu este de a determina clinic şi radiologic rata de succes a tratamentului endodontic într-o singură şedinţă de lucru - este un studiu retrospectiv pe o perioadă de 6 luni - 2 ani. Material şi metodă. Cercetarea de faţă se bazează pe un studiu retrospectiv efectuat în Departamentul de Endodonţie al Facultăţii de Stomatologie „Carol Davila”, precum şi în cadrul unui cabinet privat cu practică limitată la endodonţie, în Bucureşti. În perioada 2014-2015, pacienţilor incluşi în studiu le-a fost efectuat şi finalizat tratamentul nechirurgical al canalelor radiculare într-o singură şedinţă. Cazurile (45) au fost analizate clinic şi radiologic în cursul unei perioade de timp de reexaminare-reevaluare (6 luni, 2 ani), la finalul acestui interval rezultatul tratamentului endodontic fiind evaluat ca succes sau eşec. Rezultate. Studiul a fost realizat pe un număr total de 45 de pacienţi, dintre care femeile (12%) au avut o rată de eşec mai mare comparativ cu bărbaţii (6%); aceste diferenţe nu sunt însă semnificative statistic, pentru că pacienţii de sex feminin s-au prezentat la reevaluarea periodică într-o proporţie mai mare decât bărbaţii incluşi în studiu. Concluzii. Cele mai multe dintre cazurile asimptomatice selectate, cu sau fără patologie periapicală, au reprezentat succes al tratamentului endodontic într-o singură şedinţă.
Introduction
Regarding studies on periapical status and survival rate of tooth undergoing orthograde endodontic treatment, it has been demonstrated that periapical healing is dependent on various factors: preoperative, intra and postoperative (Ng et al., 2007)(1) on adequate coronary restoration and in the absence of complications or other iatrogenic events.
The role of microrganisms in apical periodontitis persistence and development is well known, and appropriate biomechanical treatment contributes to reducing substantially the number of germs, but without eradicating them completely.
Currently endodontic treatment completed in a single session is defined as a modality of non-surgical conservative endodontic treatment for the tooth with pathology, consisting in biomechanical preparation and obturation of the endodontic system in the same session.
Indications for this type of treatment are vital teeth with uncomplicated pulp status, coronary fractures, patients unable to return to treatment that requires antibiotic prophylaxis or sedation; contraindications of one session endodontic treatment are: teeth with acute apical periodontitis, with severe anatomic abnormalities, teeth with necrotic pulp or radiolucent periapical process and endodontic retreatment.
Treating canalar complex anatomy and multiple canals in one session depends on the skills of the practitioner. Whatever the diagnosis or effectiveness of the debridement, instrumentation and disinfection process, an endodontic treated tooth may experience mild to severe postoperative pain. However, these emergency following one session endodontic treatment have been reported less frequently than endodontic treatment after multiple sessions.
Regarding the treatment of uninfected teeth, if final obturation of the canal is possible in the first session, it is not necessary to interpose a medical dressing session with disinfection purposes(2).
Material and method
In this study it was performed one session endodontic treatment on a number of 45 asymptomatic teeth with and without periapical pathology. Thus, the endodontic treatment completed in a single session proved to be effective on a number of 43 cases, clinically and radiologically studied (periapical X- Ray and cone beam computed tomography; CBCT).
Our research is based on a retrospective study performed in The Endodontics Department of the “Carol Davila” Faculty of Dentistry and in a private practice limited to Endodontics in Bucharest. Between the years of 2014-2015, there were evaluated retrospectively to the agenda, following endodontic treatment and taking out patients who were initiated and completed nonsurgical root canal treatment in a single session. Based on clinically and radiographically analyzed cases (45) and on a reexamination-reconsideration time (6 months, 2 years) it was decided the success or failure for each case. Two clinicians reviewed both the treatment and the reappraisal, as such being included in the study both vital and devital teeth, as well those which presented periapaical pathology. If the canal could not be completely dry, the root canal obturation obviously could not be completed in the same session, therefore the tooth was excluded from the study group. Crown-down instrumentation technique was accomplished, or rotary technique, or using a combination of the two of them, endodontic hand instrumentary was used along with canal irrigation with 3.5% sodium hypochlorite (NaOCl) and 17% ethylenediaminetetraacetic acid (EDTA), the working length being initially determined by apex locator and then radiologically confirmed (in case of necessity). Root canal was sealed using cold lateral condensation technique of guttapercha; if the tooth on 6 months - 1 year revaluation was symptomatic, without evidence of any radiological healing trend, requiring endodontic treatament resumption or surgical treatment, the case was therefore considered as failure.
Results
The study was conducted on a total of 45 patients, out of which women (12%) had a higher failure rate comparable to men (6%). However, these differences are not statistically significant because there were only 34 women and 11 men in the study, this being explained by the fact that female patients were presented at reevaluation in higher rate than men did.
There were selected 6 cases that are presented as follows:
Case I - GC patient, aged 29, presents 37 asymptomatic tooth with deep caries. The patient accuses shorter episodes of moderate pain history.
Endodotic treatment is decided and completed in same treatment session.
Figure 1 - 37 tooth after endodontic treatment completed in one session.
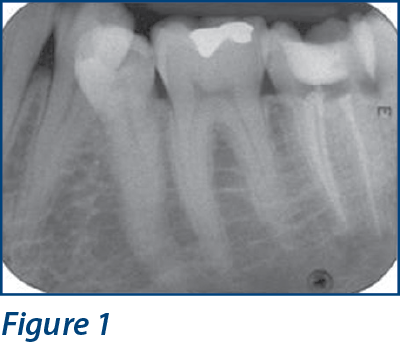
Figure 2 - X-ray control on 37 tooth after 1 year - there is a tendency of periapical healing.
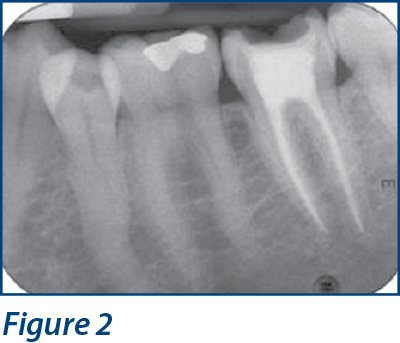
The control radiography performed after 12 months (Figure 2) found decreased periapical radiolucent.
Case II - VG patient, aged 47, presenting for coronary fracture of tooth 22 with chronic apical fibrousperiodontitis (Figure 3). It was decided one session endodontic treatment.

Figure 3 - tooth 22 with chronic apical periodontitis, radiological image obtained after completion of long term lasting obturation.
Figure 4 - tooth 22 with the radiolucent periapical with diminished tendency.

On the performed X- Ray after 10 months (Figure 4) a favorable evolution is observed, with decreased periapical and side radiolucent
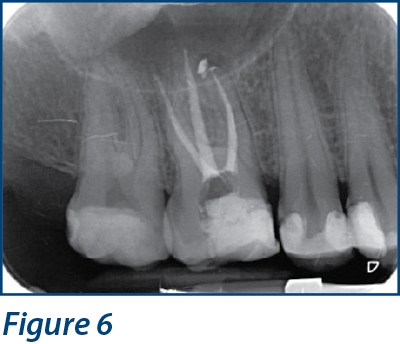
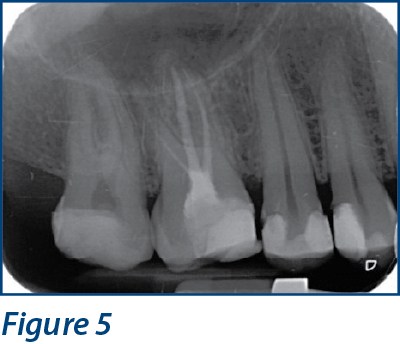
Case III
Endodontic retreatment is performed on tooth 16 (Figure 5) without interleaving a dressing with Ca (OH) 2, the patient is asymptomatic
Figure 5 and Figure 6 - tooth 16 before and after endodontic retreatment completed in a single session.
Case IV
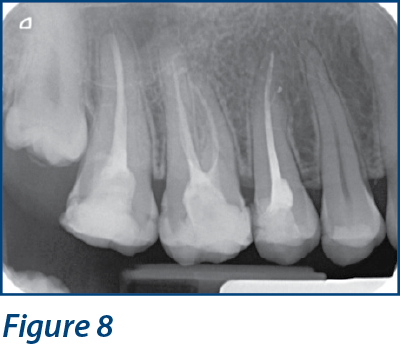
Patient with 15 tooth with acute irreversible pulpitis symptoms, deciding vital extirpation with root canal obturation during cold lateral condensation technique of guttapercha and sealer AH26 (Dentsply).
Figure 7 - 15 tooth before endodontic treatment

Figure 8 - 15 tooth after endodontic treatment completed in one session
Case V
Tooth 33, 34 with advanced coronary destructions. Endodontic treatment is decided upon in one session (Figure 9). Figure 10 - immediately after root canal obturation and radiographic control of the assessment after six months reveals a tendency to narrow the periapical radiolucenton 33.
Figure 9 and Figure10 - radiological images before and after endodontic treatment completed in one session.

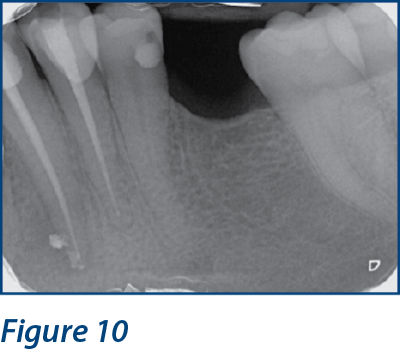
Figure 11- radiography control after 6 months - the tendency to reduce the radiolucent.

Case VI
Tooth 45 diagnosed with chronic apical periodontitis (Figure 12), incomplete root canal obturation, long term lasting obturation is decided to accomplish upon during the same session (Figure 13).
Figure 12 - incomplete root canal obturation on tooth 45.

Figure 13 - 45 tooth after root canal obturation.

The success rate of treatment in a single session is not age-dependent, but of course, on the elderly patient, the endodontic approach can sometimes be hampered by hipermineralization, dentin apposition and should be considered a trend of slow healing. Two clinicians followed the treatment steps and estimations were accomplished regarding the success level, since there were no significant differences between the two evaluators success rate versus the cases selected for one session endodontic treatment, the course required changes in the therapeutic case management, these being correlated with anatomical complexity, depending on the type of tooth and its position.
Endodontic treatment failures completed in one session (on 2 cases) may be assigned to the diversity of endodontic biofilm, residual infection and probably due to the inefficiency of chemical decontamination methods of the endododntic system.
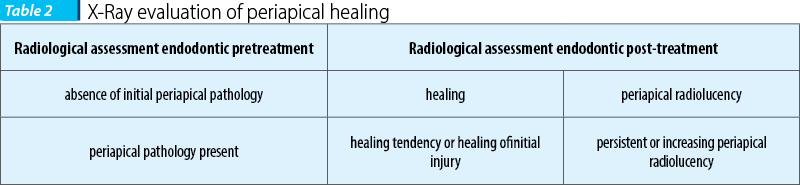
Studies on postoperative (Table 1) pain as healing rate (Table 2) showed that the results are somewhat similar, whether made in one or more sessions.

Discussions
The advantages of endodontic treatment completed in one session are: reduced number of sessions, decreased risk of microbial recontamination and the opportunity of immediately applying the intraradicular post. It removes the recontamination potential during the delay, a permanent restoration can be applied earlier, ensuring a long-term success(3).
The immediate root canal obturation of those teeth which are not infected is not controversial and basically, probably preferable to the treatment in multiple sessions. If aseptic environment is maintained, then a disinfectant dressing in between sessions is not required anylonger. Data obtained from bacteriological studies and clinical follow-up studies show that current disinfection methods in one session are not as effective and predictable as multiple treatment sessions, especially if infected canals(4,5).
The case must be carefully evaluated prior to initiating therapy; the cases should be selected depending on the degree of difficulty and practitioner’s level of training. Protocols studies that have shown good healing after one treatment session emphasize the following factors in an aseptic treatment approach: using rubber dam, isolation of the area access; apical instrumentation to a size that allows adequate debridement and proper irrigation of the infected apical canal portion; abundant irrigation with sodium hypochlorite and chlorhexidine and ethylenediaminetetraacetic acid (EDTA)(6,7).
If there is enough time, a tooth diagnosed with irreversible pulpitis should be treated in a single session.
In the absence of infection at or near the periapex, there is justification for treatment in one session. According to the latest research, there is no acceptance for necrotic teeth to require one or more weeks of intracanal dressing to ensure proper disinfection and healing of the apical pathology(8). Recent research demonstrates that when debridement and antimicrobial therapy are thorough investigation, complete and accurately accomplished, a comparable healing occurs regardless of whether the treatment was carried out in one or several sessions.
Most practitioners believe that if the treated tooth is not infected, completion of treatment is recommended in a single session(9).
Temporary disinfectant dressing followed by provisional closing is necessary when the root canal treatment can not be completed in one session. This is required for organizational reasons or lack of time due to persistent exudate and hence it is necessary to obtain additional disinfectant action. There is controversial regarding the usefulness and sense of intercalation the disinfectant dressing.
If multiple sessions, the canal is being dressed between sessions with calcium hydroxide, if the tooth is infected and presents associated periapical radiolucent. The dressing is being keept for at least 1 week. These teeth may be contaminated by difficult bacterial flora than in primary infection cases. Studies of clinical reference on patients with asymptomatic apical periodontitis teeth on which were applied antiseptic protocols, isolation with rubber dam, canal disinfection with hypochlorite during and after canal preparation, smearlayer removal with EDTA and final irrigation with chlorhexidine 2% showed similar results in respect to one or multiple sessionsof endodontic treatment.
Each case must be evaluated individually based on the patient’s medical and dental record and current signs and symptoms, to determine the number of sessions required.
A recent in vivo study(10) (Vera et al.) examines the effects of treatment on a single meeting or more on microbiological status of the mesial canal of a mandibular molar with primary apical periodontitis, the protocol for several sessions with calcium hydroxide treatment showed a microbiological status compared to the protocol accomplished in one session. Studies accomplished on single session treatment without intercanalar medication showed that residual bacteria are common and abundant in ramifications, isthmuses and dentinal tubules.
Studies show that treated teeth in a single session with diagnosis of apical periodontitis have a reasonable prognosis for full recovery and that the benefits of accomplishing endodontic treatment in one session outweigh these risks. The patient should be informed on the benefits in terms of risk taking (on an informed consent).
Conclusion
The decision to treat endodontically a tooth in one or several sessions depends on the medical and dental history, the amount of tooth structure remaining, symptomatology, signs of inflammation and the anatomic complexity; however, the final decision to treat the case belongs to the practitioner and should be done in an individualized manner.
One session treatment versus more continues to generate controversial discussion. If vital teeth, treatment is predictable in a single session, but in cases of apical infection, there should be interleaved medication dressing.
Contamination and reinoculation prevention between sessions and timing the long lasting fillings cause some clinicians to elect for performing endodontic treatment in one session.
At the six-month follow-up sesion, significant reduction of the lesion size and density changes was evidenced on the radiography, and healing was observed in the majority of cases.
However, it is necessary to deepen the clinical trial to determine factors associated with successful implementation of treatment in a single session.
Additional studies are needed to obtain pertinent data on large samples of patients who followed reproductible parameters regarding clinical and radiological healing and long-term reevaluation steps.
Bibliografie
-
Y-L. Ng et al. Outcome of primary root canal treatment: sistematic review of the literature Part 1 Effects of study Characteristics on probability of succes, J.E. Journal 40.921 -939 Dec.2007.
-
HA Ray, Trope M. Periapical status of endodonticaly in relation to the teeth Treated technical quality of the root filling and the coronal restauration Endod Int J 1995; 28: 12-18
-
PN Nair, Henry S, V Cano, Vera J. Microbial status of apical root canal system of human mandibular molars with primary apical periodontitis first after “one-visit” endodontic treatment. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2005; -99: 231-252.
-
Trope M, Delano EO Orstavik D. Endodontic treatment of teeth Orstavik apical periodontitis: multivisit vs single treatment. Journal of Endodontics, 1999: 25, 345-50.
-
JWField, JL Gutamann, ESSolomon & H.Rakusin. A retrospective clinical radiographic assessment of the success rate of single-visit root canal treatment, Endodontic Journal International, from 37.70 to 82, 2004.
-
Pisano DM, DiFiore PM, Mc Clanahan SB, Lautenschlager EP, Duncan JL. Gutta-percha Intraorifice sealing of root canals obturated to Prevent coronal microleakage. J Endod October 1998; 24 (10): 659-62.
-
Donald E Arens, Allan H Gluskin, Christine I Ove A Peters Peters. Practical Lessons in Endodontic Treatment Quintesence 2009. 212-220.
-
W Saunders. Latest concepts in root canal treatment, British Dental Journal, April 23-2005, Vol 198 515- 516.
-
Meister F Jr, TJ Lomell, Gerstein H. Diagnosis and Possible causes of vertical root fractures. Oral Surg Oral Med Oral Pathol 1980 March; 49 (3): 243-53.
-
Vera J, JF Siquiera, Ricucci D, et al. One-versus-visit endodontic treatment of two teeth with AIPC periodontitis: a study histobacteriologic. Endod J 2012; 38: 1040-1052.