The continuously growing number of diagnosed skin cancers, of which a great percent is located on the face, has determined plastic surgeons to find better answers and solutions to the challenging questions regarding reconstruction following tumor excision. The only thing complex post-excisional face defects have in common is that they widely vary from a patient to another. The nasal vestibule is the most anterior part of the nasal cavity, enclosed by cartilages and lined by skin anteriorly and respiratory epithelium in its posterior part. The nasal vestibule is a specialized organ with unique characteristics that need to be considered when reconstruction is planned. We present a complex defect of nasal vestibule and ala, following radical excision of basal cell carcinoma.
Reconstrucţia de vestibul nazal şi aripă nazală cu cartilaj auricular şi lambou cutanat latero-nazal după excizia unui carcinom bazocelular
Reconstruction of the nasal vestibule and ala using ear cartilage and folded lateral nasal flap after large basal cell carcinoma excision
First published: 01 martie 2019
Editorial Group: MEDICHUB MEDIA
DOI: 10.26416/Orl.42.1.2019.2207
Abstract
Rezumat
Numărul în continuă creştere al cancerelor cutanate diagnosticate, dintre care un procent important localizat la nivelul feţei, a determinat chirurgii plasticieni să încerce să găsească răspunsuri şi soluţii din ce în ce mai bune la provocările reconstrucţiei defectelor post-excizionale. Îndrăznim să susţinem că singurul lucru pe care defectele de la nivelul feţei îl au în comun este tocmai larga varietate de la un pacient la altul. Vestibulul nazal este partea cea mai anterioară a cavităţii nazale, încadrat de cartilajul nazal şi căptuşit cu piele în partea anterioară şi epiteliu respirator în partea posterioară. Prezentăm în acest articol un defect complex ce include vestibulul nazal şi aripa nazală, după excizie largă de carcinom bazocelular ulcerat.
A 62-year-old female patient, without any significant medical history, presented to our Plastic and Reconstructive Department for an ulcerated tumor in the nasal vestibule, including the inner lining of the nasal cavity, along with ipsilateral nasal ala retraction (Figure 1), but with no difficulties in breathing. The lesion was moderately painful, with a progressive evolution for the last 18 months.
After a thorough assessment of the tumor’s size, shape, location and extension, we decided to perform the surgery under general anaesthesia. The aim of the reconstruction was to follow the basic principles of plastic surgery by ensuring reliable structures with adequate blood supply and skin coverage with similar color and texture. After wide tumor excision, the complex defect included full thickness nasal ala along with the underlying lining, the inferior wall of the vestibule and partially the philtrum (Figure 2).
Discussion
The reconstructive options for this defect were as follows:
1. Paramedian forehead flap and cartilage graft (a two-stage procedure).
2. Lateronasal cutaneous flap and cartilage graft (a one-stage procedure).

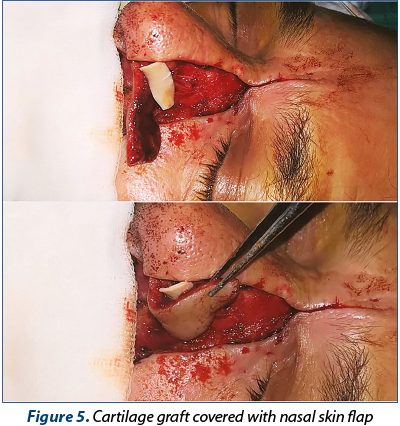

Our final choice was the one-stage procedure, as it also offered superior functional and esthetic outcome to the paramedian forehead flap. A lateral nasal skin flap is carefully elevated and dissected just above the upper border of the defect (Figure 3) in order to preserve the blood supply from the nasal muscle – the external nasal artery and angular artery. Cartilage graft was harvested from the left concha and trimmed similar to the contralateral cartilage regarding angulation and size (Figure 4) and covered by a folded nasal skin flap (Figure 5). We assessed the final nostril dimension and estimated that there will be no airflow obstruction (Figure 6). The rest of the defect was covered with a local transposition flap (Figure 7) sutured in double layers (Figure 8).



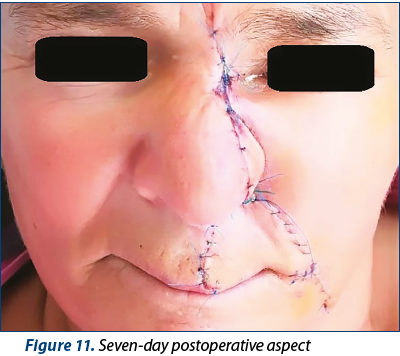
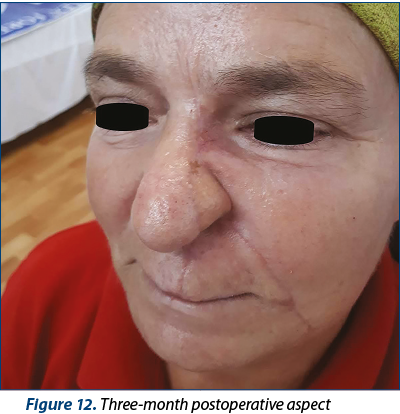
The immediate postoperative aspect was satisfactory for both the surgeons and the patient (Figure 9), with good results three days (Figure 10) and seven days (Figure 11) after the surgery. We removed the skin sutures in the seventh day after surgery and did not register any complications. Unfortunately, the patient lived 380 km from Bucharest and could not comply with the follow-up protocol. Three months after the surgery we had a telephonic conversation with the patient, and we received a picture (Figure 12) from the local dermatologist – the patient had no functional complaints and declared herself satisfied with her final appearance.
Conclusions
As the most central part of the face, the nose is extremely important in keeping harmonious proportion to one’s face. Full-thickness defects of the nasal ala require cartilage graft in order to prevent alar collapse during inhaling. Cartilage grafts require strong vascular support offered only by flaps. Therefore, when reconstructing post-excisional defects of the nose, the surgeon is challenged with both functional and esthetic targets.
Conflict of interests: The authors declare no conflict of interests.
Articole din ediţiile anterioare
Carcinomul de vestibul nazal – comentarii pe baza unui caz clinic
Întâlnit la mai puţin de 1% din totalitatea neoplasmelor capului şi gâtului, carcinomul cu localizare la nivelul vestibulului nazal este o patol...
Excizia unui papilom scuamos de vestibul nazal cu electrochirurgie de înaltă frecvenţă
Tumorile nazale benigne reprezintă o patologie neobişnuită, cu diferite tipuri histologice. Papilomul scuamos al vestibului nazal, denumit şi verru...
Reconstrucţia unui defect extensiv la nivelul nasului cu lambou frontal paramedian după excizii seriate pentru recidivă locală de carcinom bazocelular
Cancerele de piele sunt cele mai frecvente tipuri de cancer, cu o creştere semnificativă a incidenţei şi prevalenţei în ultimele decenii. S-a încer...
Urmărirea pacienţilor cu carcinom bazocelular
Tegumentul poate fi afectat de tumori maligne, cu preponderenţă carcinomul bazocelular, urmat de cel spinocelular şi melanomul malign. Patol...