Even in the 21st century, infectious diseases are still known to have an impact on the quality of life of the pediatric population. In addition to the specific or symptomatic treatment of the disease, nutrition plays a crucial role in the faster resolution of the disease and in improving the immune status of the child. A vicious cycle exists between infections and nutrition. Infection determines malnutrition while undernutrition drives an increased risk of infection by reducing gut barrier function, modifying the intestinal microbiota, altering the regulation of inflammatory adipocytokines, and limiting the uptake of key micro- and macronutrients. Carbohydrates, lipids and proteins are part of the macronutrient category because they have energy value and are needed by the organism on a daily basis, while micronutrients like vitamins and minerals are needed in a small amount. The water intake is the most important to mention during the illness, the fluid intake being calculated for each child per kilogram of body weight. The lack of hydration or the refusal of oral nutrition can lead to extreme manifestations of dehydration and malnutrition that can endanger the patient’s life. It is important to note that infectious diseases, although preventable by vaccination, continue to cause public health problems worldwide, mentioning that there are vaccines that can prevent these contagious diseases and reduce mortality and morbidity among the pediatric population.
Nutrition as a key factor in pediatric infectious disease
Nutriţia – factorul-cheie în bolile infectocontagioase pediatrice
First published: 12 aprilie 2022
Editorial Group: MEDICHUB MEDIA
DOI: 10.26416/Pedi.65.1.2022.6283
Abstract
Rezumat
Chiar şi în secolul XXI, bolile infectocontagioase sunt încă recunoscute pentru impactul asupra calităţii vieţii la populaţia pediatrică. Este bine cunoscut faptul că, pe lângă tratamentul specific sau simptomatic al bolii, nutriţia are un rol crucial în rezoluţia mai rapidă a simptomatologiei şi în îmbunătăţirea statusului imunitar al copilului. Între infecţii şi nutriţie există un cerc vicios. Infecţia determină malnutriţie, în timp ce subnutriţia conduce la un risc crescut de infecţii, prin reducerea funcţiei barierei intestinale, modificarea microbiotei intestinale, modificarea reglării adipocitokinelor inflamatorii şi limitarea absorbţiei de micro- şi macronutrienţi-cheie. Carbohidraţii, lipidele şi proteinele fac parte din categoria macronutrienţilor, deoarece au valoare energetică şi sunt necesare organismului zilnic, în timp ce micronutrienţii precum vitaminele şi mineralele sunt necesari într-o cantitate mică. Aportul de apă este cel mai important de menţionat în timpul bolii. Lipsa hidratării sau refuzul nutriţiei orale pot duce la manifestări extreme de deshidratare şi malnutriţie care pot pune în pericol viaţa pacientului. Extrem de important de menţionat sunt existenţa vaccinurilor, care pot preveni aceste boli infectocontagioase, precum şi importanţa lor în scăderea mortalităţii şi mobidităţii în rândul populaţiei pediatrice.
Introduction
There is a huge burden of pediatric infectious disease all over the world, taking into account that nearly 5.6 million children under 5 years old lose their lives die every year, and as high as 80% of these deaths occur in areas with an important rate of pediatric malnutrition, maternal and child undernutrition and overweight in low-income and middle-income countries(1). The infectious diseases known to continue to have an impact on the quality of life in the pediatric population are chickenpox, rubella, measles and mumps. Although they can be prevented by vaccination, new cases are reported annually in our country. An inadequate dietary intake leads to weight loss, lowered immunity, and impaired growth and development in children. Cause-effect studies revealed that malnourished children, as well as suboptimal nutrition intake during illness are important factors for morbidity and mortality(2). There is a complex interaction between nutrition and infectious disease in children and this relationship can be addressed according to the following criteria:
a) the influence of nutrition upon human immune system development;
b) infectious diseases in malnourished patients;
c) food-related infectious diseases;
d) nutrition in patients with immunodeficiency;
e) organism overreaction and infection (Figure 1).

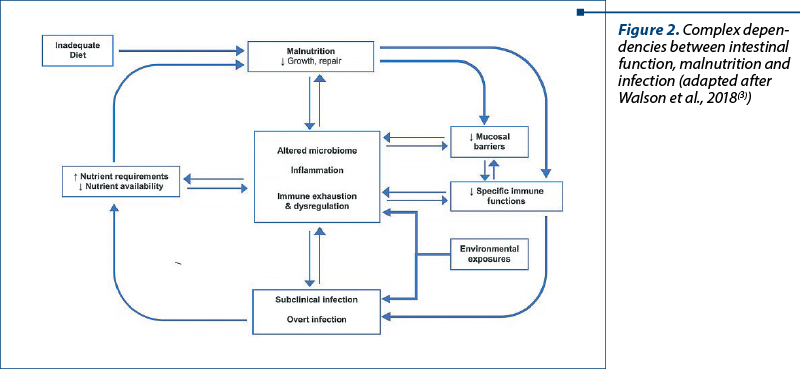
The integrity of the entire ecosystem is mandatory for a safe defense capacity. Any alteration of the gut colonization, respiratory biofilms, and other mucosal surfaces should be regarded as a precursor to invasive infection. Malnutrition is typically associated with important changes in the normal intestinal bacterial populations (dysbiosis) and this will lead to alteration in barrier functions. The surface of the gut mucosae is a huge organ implicated in nutrient absorption in order to maintain growth, healing and recovery; at the same time, it is the interface between microbiota and the predominant lymphoid tissue in the body. Intestinal barrier function functions as a site for pathogen recognition, translocation, at the same time when absorption and secretion should take place. Biochemical signals are sent to the subendothelial layer, modulating hormonal secretions and other immune cell responses.
Preliminary data upon dependencies between nutrition and infections are set up since 1968, when Scrimshaw monography explained that malnourished organisms experience recurrent infections, and the infections induce malnutrition through food refusal, malabsorption, and high nutrient demands(3). Nowadays, the mechanisms are considered to be more complex, as we know more and more about microbiota implication on infections, the immunological implications of intestinal mucosa and the chronic intestinal inflammation consequences on nutrition. Walson et al. proposed such a complex framework, in terms of immunity, between infections and nutrition(4).
Varicella
Chickenpox – known also as varicella – is an infectious, self-limiting, contagious disease, clinically characterized by a blistering rash that occurs in several eruptive waves, accompanied by fever and chills. The etiological agent is represented by the varicella-zoster virus which gives lifelong humoral immunity, with exceptional reinfection in immunocompromised individuals.
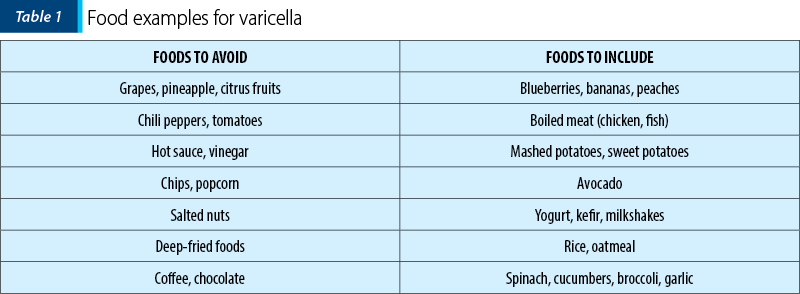
During the febrile period, a nutritious diet is recommended to maintain the nutritional needs of the child and a home-cooked meal is essential. Processed or junk food must be avoided. Hydration is extremely important and patients need to know how to estimate their child’s water needs. It should be noted that fever increases water needs by about 10 ml/kgc/1*C/24 hours. In the age category 1-5 years old, depending on body weight, the water requirement is 1300-1500 ml/day, which corresponds to an amount of about 100-120 ml/kg/day.
Eating fruits rich in vitamin C and A helps relieve infection and regenerate the epidermis, like blueberries. Also, coconut oil taken orally or in cooking is beneficial due to its antibacterial, antifungal and antiviral properties.
Below we present a table with which food to include and which to avoid.
Rubella
Rubella is an endemic infectious disease characterized by maculopapular rash, occipital and retroauricular polyadenopathies, along with catarrhal respiratory manifestations. The etiological agent of rubella is the rubella virus, which belongs to the genus Rubivirus, the Togaviridae family.
The hygienic-dietary treatment is based on a resting diet during the febrile and eruptive period, offering your child a hydrolactosaccharate diet to maintain the right nutrition. Soft foods full of macro- and micronutrients are the perfect candidates for a child’s diet. First of all, hydration remains essential, water and fresh fruit juices being easily accepted by the children.
The citrus fruits (lemon, oranges, grapefruit) provide a consistent intake of vitamin C and fibers which, on one hand, improve appetite and, on the other hand, support the immune system and help maintain it. Also, it’s important not to offer children high-fat foods, fried foods, spicy and processed foods, commercial carbonated sweets drinks and commercial sweets.
Measles
Measles is an extremely contagious disease, clinically characterized by fever, enanthema and a characteristic rash, being a major cause of morbidity and mortality in infants and unvaccinated children. It belongs to the genus Morbillivirus, Paramyxoviridae family. The rash is represented by an erythematous maculopapular with descending character, velvety on palpation, that can appear in eruptive plaques on the chest or abdomen, the rash fading in about 5-6 days, followed by furfuraceous desquamation on the face and chest. Note the pathognomonic sign that appears about two days before the eruption and persists for another two days after its disappearance, the Koplik sign. The respiratory catarrh is of particular interest to the larynx, being expressed by a dry cough associated with dysphonia, and in more severe cases there may occur dyspnea, polypnea, respiratory function syndrome and sometimes even asphyxia.
This is why the children’s nutrition is very useful in improving health. As in other contagious diseases, hydration plays an essential role, being a hydrolactosaccharate diet in the febrile period, followed by a balanced diet.
Vitamin A deficiency and measles, which are estimated to kill 2 million children per year, are closely linked. Measles in a child is more likely to exacerbate any existing nutritional deficiency, and children who are already deficient in vitamin A are at a much greater risk of dying from measles. Postmeasles diarrhea is particularly difficult to treat and has a very high mortality(4). Vitamin A deficiency increases the risk of developing respiratory disease and chronic ear infections. Vitamin A supplementation sustains gut integrity, lowers the incidence of respiratory tract infections, reduces mortality from diarrhea and enhances immunity. Measles also depletes the body’s supply of vitamin A. Thus, vaccination against measles often includes a high dose of vitamin A(4).
An interesting article about maternal beliefs and practices regarding the diet and use of herbal medicines during measles showed that 208 mothers from Jaipur District in Rajasthan, India, preferred foods during measles such as kishmish/munakka (38.5%), khichri/rabbi of bajra (35.6%), daliya (25%), and cow’s milk (23.1%)(5). The restricted foods included roti (62.5%), all dals except moong dal (59.1%), and vegetables (42.8%). The leading herbal medicines used to treat measles were a mixture of nutmeg, mace, clove, tulsi leaves and kishmish (26.9%) and a mixture of nutmeg, mace, clove, tulsi leaves and brahmi (25.5%). The mothers believed that herbal medicines saved their children’s lives(5).
Mumps
Mumps is an acute, contagious infectious disease caused by the urlian virus which is manifested by inflammation of the salivary glands (parotid, submaxillary, sublingual) and other organs with glandular structure (pancreas, ovaries, testicles). The swelling of the salivary glands, especially the parotid glands, is very painful, often accompanied by trismus, the facies acquiring a characteristic pear-like appearance. The enanthema in the disease is manifested by hyperemia and edema of jugal mucosa with hyperemia and hypertrophy of the Stenon canal.
For this reason, it is recommended that meat, vegetables and fruits be cooked or steamed, so as not to require chew that can make the discomfort and pain worse. As in other cases, hydration is important, water and tea being encouraged to consume and, in case of inability to ingest, there can be used for rehydration parenteral infusions with electrolytes. Cream soups, oatmeal, potatoes, sweet potatoes, carrots, broccoli sauteed or puree with boiled fish or chicken are recommended. Also, from the category of fruits, there can be added to the diet, depending on the season, melon, blueberries, apricots, cherries, and especially fruit compotes and jam.
From the diet, they must be avoided fatty red meat, fried foods, spicy sauces, sugar, commercial sweets, as well as citrus fruits and carbonated juices that can stimulate saliva production and intensify the pain.
The role of nutrition
A malnourished baby who does not receive enough protein and vitamins is prone to infectious diseases and does not respond well to vaccines(7). Therefore, nutrition is critical to provide high immunity in humans against environmental pathogens(7). For example, the concentration of vitamin C is reduced in patients’ blood with infections, and this situation is even seen in people who have received measles and smallpox vaccine.
Other minerals and vitamins that are decreased during the infections are: vitamin B2, vitamin A, iron, zinc and copper.
The benefits of enteral nutrition include: reduction of gut atrophy, improvement of gut motility, reduction in infections, enhanced gut immune function and avoidance of translocation, cost effectiveness and the fact that it is less likely to overfeed the patient. However, sometimes we have to resort to parenteral nutrition only when we are unable to meet the nutritional requirements via the gastrointestinal tract or there exists a bowel dysfunction resulting in an inability to tolerate the enteral nutrition for 4-5 days in children and adolescents(8). The parenteral nutrition will be indicated and performed only in the hospital by the specialists.
The importance of the immune system
The immune system is responsible for providing good defense against pathogenic organisms and to provide tolerance to non-threatening organisms, to food components, and to the self. Babies are born with an immature immune system that fully develops in the first few years of life, and malnutrition in childhood might have long-term effects on health. Undernutrition decreases immune defenses, making an individual more susceptible to infection(9). Undernutrition leading to impairment of immune function can be due to insufficient intake of energy and macronutrients and/or due to deficiencies in specific micronutrients. Nutrients that have been demonstrated to be required for the immune system to function correctly include essential amino acids, the essential fatty acid linoleic acid, vitamin A, folic acid, vitamin B6, vitamin B12, vitamins C, D, E, Zn, Cu, Fe and Se(10).
Antioxidant vitamins and trace elements (vitamins C, E, selenium, copper and zinc) counteract the potential damage caused by reactive oxygen species to cellular tissues and modulate immune cell function through regulation of redox-sensitive transcription factors and affect the production of cytokines and prostaglandins. An adequate intake of vitamins B(6), folate, B12, C, E, and of selenium, zinc, copper and iron supports a Th1 cytokine-mediated immune response with sufficient production of proinflammatory cytokines, which maintains an effective immune response and avoids a shift to an antiinflammatory Th2 cell-mediated immune response and an increased risk of extracellular infections(11). The supplementation with these micronutrients reverses the Th2 cell-mediated immune response to a proinflammatory Th1 cytokine-regulated response with enhanced innate immunity(11).
It is known that the effect of vitamin A supplementation on preventing death from childhood disease is one of reducing the severity of infectious illnesses, while zinc can reduce the risk of infection and reinfection.
Also, vitamin A deficiencies induce the loss of mucus-producing cells. This loss of the protective mucus blanket increases the susceptibility to infection by pathogens that would ordinarily be trapped in the mucus and swept away by the cleansing flow of mucus out of the body. Barrier defects of mucous membranes are critical in the pathogenesis of respiratory and gastrointestinal tract infections(18).
Moreover, an inadequate intake of these vitamins and minerals may lead to suppressed immunity, which predisposes to infections and aggravates malnutrition.
Undernutrition
Undernutrition still contributes to almost 50% of all annual deaths in children under 5 years old. Commonly termed “malnutrition,” undernutrition can have an acute, chronic or acute-on-chronic presentation and refers to children who are underweight for their age or length, too short for their age or deficient in key macro- or micronutrients. Undernourished children are more vulnerable to infectious pathogens and more likely to die from infectious diseases(12).
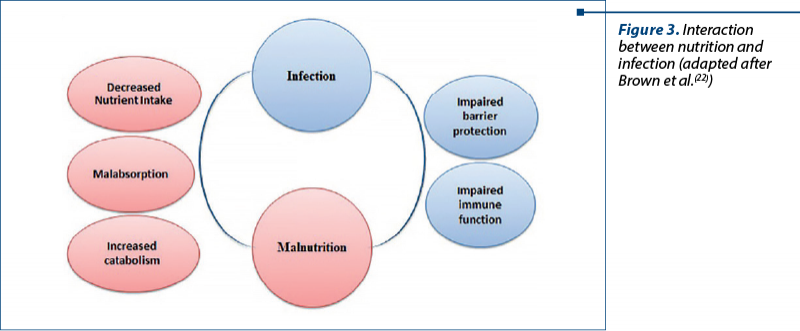
A vicious cycle exists between nutritional status and infection. On one hand, infection results in undernutrition due to nutrient loss, reduced uptake and increased energy requirements. On the other hand, undernutrition increases the risk of infection by reducing the gut barrier function, modifying the intestinal microbiota, altering regulation of inflammatory adipocytokines and limiting the uptake of key micro- and macronutrients(12).
Leptin is an important adipocytokine and it serves as a critical mediator of glucose and lipid metabolism, angiogenesis, hematopoiesis and innate and adaptive immune function. Therefore, undernutrition has a profound impact on vulnerability and outcomes from a variety of childhood infectious diseases(21).
The relationships among malnutrition, immune suppression and infection are complicated by the severe effects that a number of infections exert on nutrition. Examples of how infections can contribute to malnutrition include(16):
1) gastrointestinal infection that leads to diarrhea;
2) chronic infections that cause cachexia and anemia;
3) intestinal parasites that cause anemia and nutrient deprivation.
In 2008, a descriptive and prospective study was conducted on 335 children under 6 years of age who were admitted to a hospital in Colombia for severe acute malnutrition (83%) or moderate acute malnutrition associated with illness (17%). The most common complication upon admission was diarrhea (68.4%) and the most common complication during hospitalization was sepsis (9%). Children with moderate acute malnutrition had similar complications and mortality when compared to children with severe acute malnutrition(17).
Vaccination: the key
Vaccination is the only way to prevent infection or mitigate potentially life-threatening forms of these viruses.
For countries where varicella is a health burden, World Health Organization (WHO) recommends that if sufficient resources exist to reach and sustain a vaccine coverage level of ≥80%, the introduction of varicella vaccination in the routine childhood immunization program should be considered(19). In countries with a high proportion of susceptible persons ≥15 years of age, World Health Organization recommends the vaccination of adolescents and adults without evidence of varicella immunity(19).
For infectious diseases such as rubella, mumps and measles, there is either a monovalent vaccine or a combined MMR/ROR vaccine that can be used for the active prophylaxis of the child. The first vaccine against human herpes virus was the live attenuated VZV vaccine made by Dr. Takahashi in 1974 from the Oka strain, with a seroconversion rate of 95%, with complete protection against the disease between 85% and 95% for a demonstrated period of at least 10 years. It can be given at the same time as the MMR/ROR vaccine. The varicella vaccine may eventually reduce or eliminate herpes zoster, which is a serious problem for elderly and immunocompromised individuals(13).
The European Regional Verification Commission for Measles and Rubella Elimination was established in 2011 to evaluate the status of measles and rubella elimination based on documentation submitted annually by each country’s national verification committee. The WHO European Region has made steady progress towards eliminating measles and rubella and over half of the countries interrupted the endemic transmission of both diseases by 2015(14).
In Romania, in 2016, a large measles outbreak started and a current study aimed to clarify who was affected by the outbreak and why they’ve chosen not to vaccinate their children. A survey was administered via telephone to 704 caregivers of measles cases (520 respondents) to explore the capability, opportunity and motivation barriers to vaccination(15). Most cases were unvaccinated and lived in low coverage areas. Ethnic minorities were disproportionally affected. Most caregivers felt welcome at health facilities. Some were less satisfied with the waiting time and had found the vaccine out of stock(15). Not everybody knew that vaccines were free of charge. Less than half knew the child’s next vaccination date, some had not been informed and did not know where to seek this piece of information. Some said their peers did not vaccinate. Beliefs were generally supportive of vaccination, but many were concerned about vaccine safety and found they had not received good information about this. The conclusions varied greatly between minorities and less educated groups, compared with people with higher education levels(15).
Parents must be informed about what these contagious diseases entail, the severity of their complications, the existence of these vaccines that are part of the child’s vaccination schedule, to explain their need and, of course, the risks and benefits of the vaccination.
Conclusions
The key to success is a balanced, healthy diet based on home-cooked food, fruits and vegetables rich in vitamins and minerals that enhance immunity and, of course, first of all, the optimal hydration to prevent the loss of water and electrolytes.
Increasing intakes of some nutrients and vitamins with the recommended levels can enhance some aspects of immune function and make it work properly. Otherwise, an inadequate intake and status of these vitamins and minerals may lead to suppressed immunity, which predisposes to infections and aggravates malnutrition. The causes of malnutrition are multiple and complex, and infections are a common precipitating factor.
It is easier to prevent than to treat, and that’s why it is so important to encourage, whenever we have the opportunity, the need to vaccinate the children against MMR and varicella, primarily to increase the quality of life and to reduce the rate of morbidity and mortality among the pediatric population.
Conflict of interests: The authors declare no conflict of interests.
Bibliografie
-
Black RE, Victora CG, Walker SP, Bhutta ZA, Christian P, de Onis M, Ezzati M, Grantham-McGregor S, Katz J, Martorell R, Uauy R, Maternal and Child Nutrition Study Group. Lancet. 2013 Aug 3;382(9890):427-451.
-
Scrimshaw NS. Historical concepts of interactions, synergism and antagonism between nutrition and infection. J Nutr. 2003;133:316S–321S.
-
Walson JL, Berkley JA. The impact of malnutrition on childhood infections. Curr Opin Infect Dis. 2018;31(3):231-236.
-
Katona P, Katona-Apte J. The interaction between nutrition and infection. Clin Infect Dis. 2008 May 15;46(10):1582-8. https://doi.org/10.1086/587658.
-
Singh MB. Maternal beliefs and practices regarding the diet and use of herbal medicines during measles and diarrhea in rural areas. Indian Pediatr. 1994 Mar;31(3):340-3. PMID: 7896375.
-
Kowalzik F, Faber J, Knuf M. MMR and MMRV vaccines. Vaccine. 2018 Aug 28;36(36):5402-5407. doi: 10.1016/j.vaccine.2017.07.051.
-
Farhadi S, Ovchinnikov RS. The relationship between nutrition and infectious diseases: A review. Biomed Biotechnol Res J. 2018;2:168-72.
-
Braunschweig CL, et al. Enteral compared with parenteral nutrition: a meta-analysis. Amer J Clin Nutr. 2001;74(4):534-42.
-
Calder PC. Feeding the immune system. Proc Nutr Soc. 2013 Aug;72(3):299-309. doi: 10.1017/S0029665113001286.
-
Calder PC, Kew S. The immune system: a target for functional foods? Br J Nutr. 2002 Nov;88 Suppl 2:S165-77.
-
Wintergerst ES, Maggini S, Hornig DH. Contribution of selected vitamins and trace elements to immune function. Ann Nutr Metab. 2007;51(4):301-23. doi: 10.1159/000107673.
-
Gwela A, Mupere E, Berkley JA, Lancioni C. Undernutrition, Host Immunity and Vulnerability to Infection Among Young Children. Pediatr Infect Dis J. 2019 Aug;38(8):e175-e177. doi: 10.1097/INF.0000000000002363
-
Arvin AM, Gershon AA. Live attenuated varicella vaccine. Annu Rev Microbiol. 1996;50:59-100. doi: 10.1146/annurev.micro.50.1.59.
-
Datta SS, O’Connor PM, Jankovic D, Muscat M, Ben Mamou MC, Singh S, Kaloumenos T, Reef S, Papania M, Butler R. Progress and challenges in measles and rubella elimination in the WHO European Region. Vaccine. 2018 Aug 28;36(36):5408-5415. doi: 10.1016/j.vaccine.2017.06.042.
-
Habersaat KB, Pistol A, Stănescu A, Hewitt C, Grbic M, Butu C, Jackson C. Measles outbreak in Romania: understanding factors related to suboptimal vaccination uptake. Eur J Public Health. 2020 Oct 1;30(5):986-992. doi: 10.1093/eurpub/ckaa079.
-
Schaible UE, Kaufmann SH. Malnutrition and infection: complex mechanisms and global impacts. PLoS Med. 2007 May;4(5):e115. doi: 10.1371/journal.pmed.0040115.
-
Bernal C, Velásquez C, Alcaraz G, Botero J. Treatment of severe malnutrition in children: experience in implementing the World Health Organization guidelines in Turbo, Colombia. J Pediatr Gastroenterol Nutr. 2008 Mar;46(3):322-8. doi: 10.1097/MPG.0b013e318156c2c3.
-
Cunningham-Rundles S, McNeeley DF, Moon A. Mechanisms of nutrient modulation of the immune response. J Allergy Clin Immunol. 2005 Jun;115(6):1119-28; quiz 1129. doi: 10.1016/j.jaci.2005.04.036.
-
Spoulou V, Alain S, Gabutti G, Giaquinto C, Liese J, Martinon-Torres F, Vesikari T. Implementing Universal Varicella Vaccination in Europe: The Path Forward. Pediatr Infect Dis J. 2019 Feb;38(2):181-188. doi: 10.1097/INF.0000000000002233.
-
Varicella and herpes zoster vaccines: WHO position paper, June 2014. Wkly Epidemiol Rec. 2014 Jun 20;89(25):265-87.
-
Alwarawrah Y, Kiernan K, MacIver NJ. Changes in Nutritional Status Impact Immune Cell Metabolism and Function. Front Immunol. 2018 May 16;9:1055. doi: 10.3389/fimmu.2018.01055.
-
Brown KH. Diarrhea and Malnutrition. The Journal of Nutrition. 2003 Jan;133(1):328S–332S. https://doi.org/10.1093/jn/133.1.328S
Articole din ediţiile anterioare
Otita medie acută la copii
Otita medie acută (OMA) este cea mai frecventă afecțiune a copilăriei, 90% dintre copiii cu vârsta sub 6 ani având cel puțin un episod de otită med...
Educaţia pentru sănătate în şcoli, o şansă pentru o generaţie viitoare sănătoasă
Bolile netransmisibile legate de stilul de viaţă (NCD) reprezintă principala cauză de deces şi morbiditate la nivel mondial. Comportamentele al...
Sindromul de regresie caudală – afecţiune congenitală rară cu implicaţii sistemice multiple
Caudal regression syndrome (CRS) – also known as caudal dysplasia, sacral agenesis or sacral defect with anterior meningocele – is a rare congenita...
Vaccinurile şi vaccinarea. Certitudini şi provocări
Într-o lume în care legile biologice fac să existe o continuă confruntare între organismul uman şi microorganisme, vaccinarea rămâne cea mai raţion...