Infantile hemangiomas (IH) are the most frequent tumors of vascular origin. The differential diagnosis with other vascular anomalies is difficult to establish and an appropriate therapeutic management is usually delayed by the underestimation of the importance of the lesion. Problematic types of hemangiomas due to location, size and fast proliferation can determine important functional and esthetic sequelae. Based on the data collected by serial clinical observation and imaging, processed by a computer-assisted diagnosis system (CAD), we studied the evolution of different types of vascular tumors, divided into three groups, according to the treatment method implemented. The database consists of 94 patients. The results show the importance of serial clinical evaluation over a long period and of the early implementation of the treatment for the dangerous hemangiomas. A multidisciplinary medical team is essential for the best outcome of the vascular tumor pathology.
Tumorile vasculare: când supraveghem, tratăm sau trimitem către chirurg?
Vascular tumors: when to observe, treat or send to the surgeon
First published: 16 martie 2021
Editorial Group: MEDICHUB MEDIA
DOI: 10.26416/Pedi.61.1.2021.4703
Abstract
Rezumat
Hemangioamele infantile (HI) sunt cele mai frecvente formaţiuni tumorale de origine vasculară. Diagnosticul diferenţial cu alte anomalii vasculare este dificil de efectuat, managementul terapeutic fiind întârziat de subestimarea importanţei multor leziuni. Din cauza localizării, dimensiunilor sau a proliferării lor rapide, hemangiomele problematice pot determina sechele funcţionale şi estetice importante. Studiul nostru a colectat informaţii seriate bazate pe supravegherea clinică şi imagistică, procesate cu ajutorul unui sistem de diagnostic computerizat (CAD), cu ajutorul căruia am evaluat evoluţia a diverse tipuri de tumori vasculare, împărţite în trei grupuri, separate în funcţie de metoda de tratament implementată. Baza de date este formată din 94 de pacienţi. Rezultatele relevă importanţa evaluărilor clinice seriate pe o perioadă lungă şi importanţa implementării precoce a unui tratament în cazul hemangioamelor periculoase. Formarea unei echipe multidisciplinare medicale este esenţială pentru a avea cele mai bune rezultate în tratarea patologiei tumorale vasculare.
Introduction
Infantile hemangiomas (IH) are the most common tumors of infancy and their management still remains a subject of considerable controversy among specialists of different areas. The true incidence of these vascular masses is difficult to quantify, because they may be present at birth (1.1%), but most of them develop in the first few weeks after birth (12.7% between the ages of 1 to 6 months old), and demonstrate a pattern of rapid disproportionately postnatal growth till the age of 1 year old, followed by a very slow involution phase that can last until adolescence. IH are more frequent in girls, in infants born preterm or with a low birth weight, in twins and in neonates with fair skin(1,2). The most affected areas are those of the head and neck regions, and the variable growth of these tumors may result in grotesque deformities and important esthetic and functional sequelae after the end of the proliferation phase. It is extremely important for the medical team who treat these patients to comprehend the biological behavior of these lesions and to make the right decision on when to intervene and treat the patients with IH. The beginning of any type of treatment has to be justified by the clinical evolution and the possible complications and endorsed by the written consent of the parents, who must be informed on the possibility of spontaneous regression of these lesions after the age of 1 years old(3). Due to their complexity, a multidisciplinary approach is frequently necessary in managing these lesions and includes a team of specialists in pediatric dermatology, surgery, orthopedics, a pediatrician and sometimes a psychologist(4,5).
Matherials and method
In this study, we included a total of 94 patients who were treated for IH between January 2015 and December 2020 in the departments of pediatric surgery from the “Maria Sklodowska Curie” Clinical Emergency Hospital for Children and the “Dr. Victor Gomoiu” Clinical Hospital for Children, both from Bucharest. This is a retrospective analytic study.
All the patients had a clinical and imagistic diagnosis of IH, with ages between 3 weeks old and 2 years old, and were separated into three different categories, according to the type of treatment they received: no treatment (watch and wait), medical treatment (propranolol), and surgical excision. We included in the study only the cases that were diagnosed under the age of 10 months old and had frequent monitoring. We collected data from the medical observation sheets (age at the discovery, age at diagnosis, location, clinical aspect, number of IH, frequency of monitoring, age at the beginning of the treatment, number of follow-ups, type of treatment) and we also had a database of photographic, ultrasound images and video recordings as a result of careful examination and surveillance.
The clinical progression of the IH was quantified using the computer-assisted diagnosis (CAD) software that takes into consideration the progression or regression of the area and the redness of the lesion.
We excluded from the study the children who were diagnosed with other types of vascular anomalies and were misinterpreted as IH and those who had less than two follow-ups with the medical team.
The statistic processing of the study results was carried out by standard algorithms of variation statistics, using Excel software and statistical software STATA 16.
Results
The CAD system of analyzing the photographic and ultrasound images of IH allowed us to study the progression or regression of the clinical and ultrasound aspect of the lesions with or without treatment and to try to find an algorithm of treatment for future patients with similar vascular tumors. We provided the software photographic data for each patient, both clinical and by ultrasound, and the system analyzed the evolution of the region of interest. The results of this processing were correlated with the clinical observation (Figure 1).

We included in the study IH from different areas (Figure 2) that were possible to quantify using the CAD system and we collected photographic data for each follow-up of the patients.

The median age of the children included in the study was 7.8 months old, with a prevalence of the female gender (72.2%).
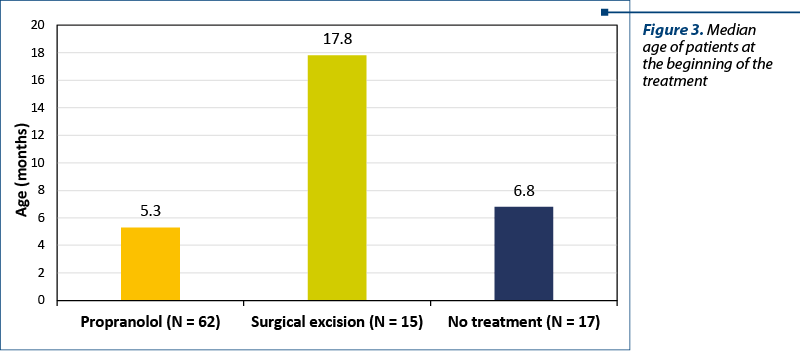
We included the patients in three different categories, according to the management of IH: medical treatment (propranolol), surgical excision, and no treatment (watch and wait). We noticed that the median age of the children who received the propranolol treatment was much lower than that of the surgical excision group and of the no treatment one (Figure 3).
We also studied the number of follow-ups that were necessary for the three management groups. The medical treatment had a median of 8.8 follow-ups, no treatment had a median of 6.8 months, and for the surgically excised IH, the median was only 3.4 months. The median period of time that the cases were followed-up was 8.7 months for the propranolol group, 6.3 months for the no treatment group, and only 1.2 months for the surgical one. We had nine cases of IH which, due to no response to the treatment (five patients) or complications during the natural evolution (four cases), needed to be surgically excised. The six more cases that needed surgical correction of the IH were older patients who had unesthetic sequalae lesions.
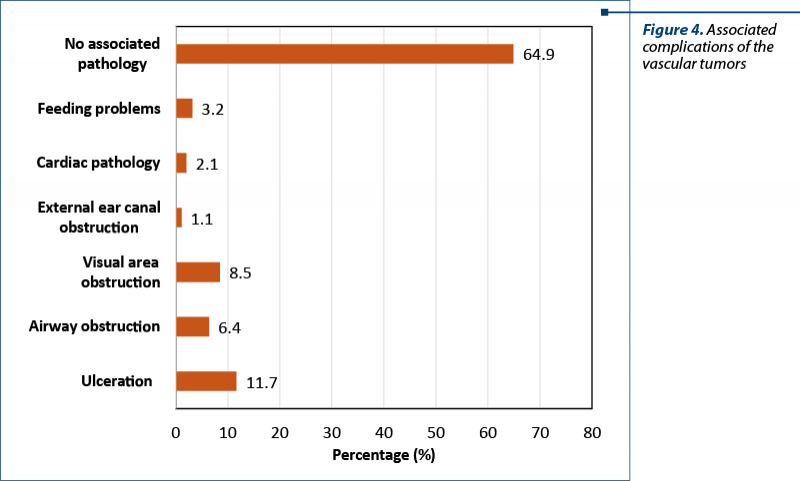
We also noticed that all the cases that presented with associated possible complications were included in the propranolol group (Figure 4).
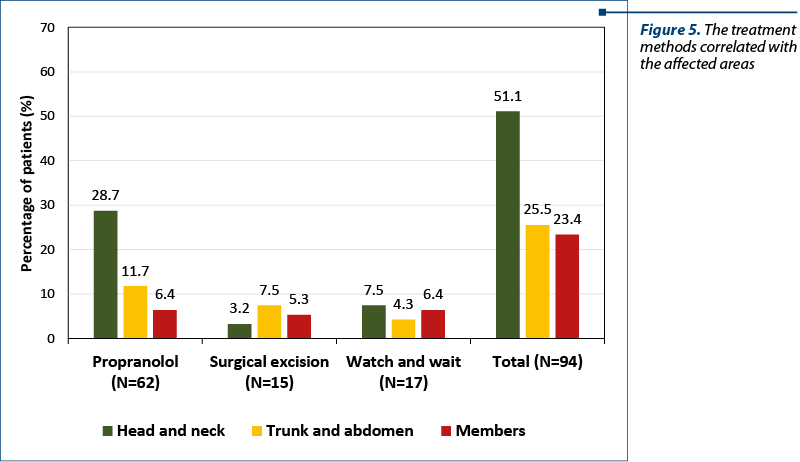
We divided the body areas affected by IH in head/neck, trunk/abdomen and members, and we noticed the differences of management (Figure 5). The treatment with propranolol was more frequently used for head and neck, and the surgical excision was more frequently used for the other areas.
The CAD system analyzed similar hemangiomas for different patients, with the same age, who were included in different study groups, and noticed a progression of the redness and area of the IH for the “no treatment” patients in 43% of the cases. These patients were registered and after that excluded from the study to receive appropriate treatment with propranolol or surgical excision.
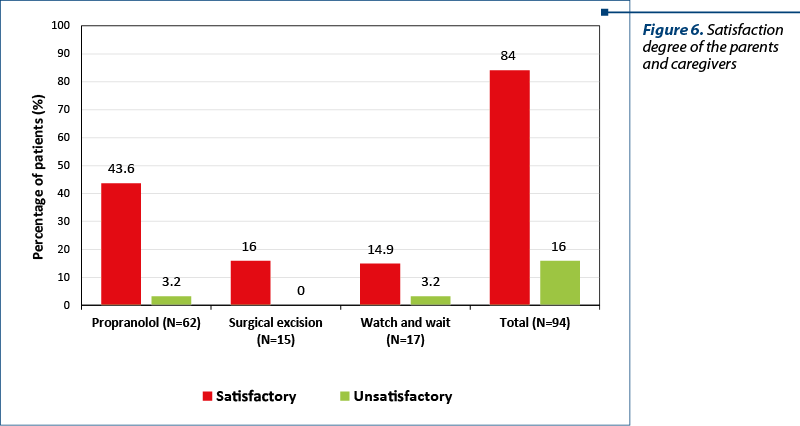
At the end of the study, we gathered data from the parents and caregivers of the patients whom we treated, concerning the efficiency of the chosen treatment method and the satisfaction degree (Figure 6).
Discussion
Vascular tumors appear in as many as 12% of infants, making them the most common benign tumor of the infancy. Many of them are small and self-resolving and require no treatment, but some of them, due to their size, location and progression, are potentially problematic. In this moment, a standardized protocol of treatment and follow-up for these lesions does not exist. Many other vascular anomalies are misdiagnosed and treated as IH, leading to confusion regarding the efficiency of the medical and surgical treatment(5).
As resulted from the study we conducted, we noticed that the first and most important step in deciding what management to apply in a vascular anomaly is to have a clear diagnosis(4). At the beginning of each evaluation, we have collected all the important anamnestic data from the parents and caregivers concerning the moment they first noticed the lesion and its natural evolution in a defined period of time. It is important to collect photographic data both clinical and using imaging, for most of the follow-ups, in order to have a clear image of the progression or regression of the image. All these corroborated data will allow the medical team to make the right decision for the management plan of the patient.
We noticed that for most hemangiomas the optimal period of time for treatment is not at the end of the proliferation period, but during the first few weeks of it, in order to stop the lesion from growing and from affecting a larger are. There is a small window of opportunity to manage those IH that are potentially high risk due to the association with life-threatening complications (air ways obstruction), functional impairment, potential for disfigurement or ulceration(1,3). It is important that the first consult take place early, during the proliferation period, for this type of IH, around 1 month of age, in order to start the treatment as soon as possible.
Oral propranolol is the treatment of choice for problematic IH and the beginning of the therapy must be carefully monitored by the medical team. We recommend at least 24 hours of admittance to the hospital for the beginning of the treatment for monitoring the arterial blood pressure of the patient before and after the propranolol, along with the glycemic level. Also, we must perform lab tests and cardiac consults before we decide what dosage of treatment we should begin with. The usual scheme of treatment for propranolol begins with 1 mg/kg/day and is quickly increased to 2 mg/kg/day, divided in three or two doses. For complicated cases, we can go as far as 3 mg/kg/day, with appropriate monitoring(1).
There are certain clear indications for the surgical excision and are limited to a small number of IH: large sized vascular tumors that affect areas that are not important from an esthetic point of view, hemangiomas that are pediculate and have a small implantation area, failure of the medical treatment for problematic lesions, treatment of complications like ulcerations and hemorrhage, excision of sequelae lesions after the end of the proliferation period, and also as a choice of the parents if the medical team approves(5).
Laser therapy is more commonly used for the treatment of IH after the period of proliferation is over. Sedation is usually required, therefore the procedure is limited to treating older patients and other types of vascular anomalies.
We must also take into consideration the psychosocial consequences of an untreated vascular tumor on the affected patient and his family if we underestimate and decide not to treat the lesion. This is especially true with facial and neck hemangiomas that cannot be hidden from view by clothing. Attempts should be made to normalize the appearance of the child before entering the social environment of kindergarten(4,5).
Conclusions
IH affect an important number of infants and the correct diagnosis is imperative for the appropriate treatment. At present, there are no modalities to predict the evolution of an infantile hemangioma, making the follow-up period very important in order to avoid underestimating the esthetic and functional sequelae. The treatment of problematic vascular tumors can be complex and often involves a large medical team, with pediatrician, cardiologist, surgeon and dermatologist.
Conflict of interests: The authors declare no conflict of interests.
Bibliografie
- Popescu M, Secheli I, Draghici I. Proposal for future diagnosis and management of vascular tumors by using automatic software for image processing and statistic prediction. Journal of Medicine and Life. 2015;8:44-48.
- Enjolras O. Classification and management of the various superficial vascular anomalies: hemangiomas and vascular malformations. J Dermatol. 1997;24:701-710.
- Hoeger PH, Harper JI, Baselga E, et al. Treatment of infantile haemangiomas: recommendations of a European expert group. Eur J Pediatr. 2015;174(7):855–865.
- Darrow DH, Greene AK, Mancini AJ, Nopper AJ; Section on Dermatology; Section on Otolaryngology – Head and Neck Surgery; Section on Plastic Surgery. Diagnosis and management of infantile hemangioma. Pediatrics. 2015 Oct;136(4):e1060-104.
- Bauland CG, Lüning TH, Smit JM, Zeebregts CJ, Spauwen PH. Untreated hemangiomas: growth pattern and residual lesions. Plast Reconstr Surg. 2011;127(4):1643–1648.
Articole din ediţiile anterioare
Hemangiomul infantil − posibilităţi de abordare terapeutică
tumori vasculare, malformaţii vasculare, hemangiom, propranolol, scleroterapie