Urgenţe dermatologice în neonatologie şi practica pediatrică
Dermatological emergencies in neonatology and pediatric practice
Abstract
The problem of dermatological emergencies arises mainly in the management of patients with serious dermatological problems in hospital or more frequently as outpatients. Emergencies in neonatologic and pediatric dermatology may occur at birth or later in other stages of childhood. The early identification of emergencies in pediatric dermatology is of great importance, because these afflictions affect not only the skin, but the entire body, putting the patient’s life in jeopardy. The early identification leads to early treatment, which may be an extra chance for the patient. Due to the young age of patients, there is a greater risk of associated complications and they are more difficult to treat.Keywords
neonatologypediatricdermatologyemergenciesRezumat
Problema urgenţelor dermatologice apare, în general, în gestionarea pacienţilor cu probleme dermatologice grave în spital sau, mai frecvent, în ambulatoriu. Urgenţele în dermatologia neonatologică şi pediatrică pot apărea la naştere sau mai târziu, în alte stadii ale copilăriei. Identificarea precoce a situaţiilor de urgenţă în dermatologia pediatrică are o importanţă deosebită, deoarece aceste afecţiuni afectează nu numai pielea, ci întregul organism, punând viaţa pacientului în pericol. Identificarea precoce duce la tratamentul precoce, care poate fi o şansă suplimentară pentru pacient. Dată fiind vârsta mică a pacienţilor, există un risc mai mare de complicaţii asociate şi sunt mai dificil de tratat.Cuvinte Cheie
neonatologiepediatriedermatologieurgenţeIntroduction
Several studies have focused on dermatological diseases in children, but too few on dermatological emergencies, these being a challenge for both the physician and the patient.
The dermatological problems in children represent 30% of the visits to the doctor(1).
In a Swiss pediatric emergency department a wide range of dermatological diseases was identified for patients, most of which being inflammatory/allergic (42.9%) or infectious (31.8%)(2).
The study from New Delhi found the prevalence of neonatal dermatological emergencies in the studied group as follows: epidermolysis bullosa (50%), collodian baby (33.3%), dermatological reactions associated with the intensive neonatal unit (18.7%), harlequin’s fetus (16.7%), infantile seborrheic dermatitis (12.5%); while the prevalence of post-neonatal dermatological emergencies was: drug reactions (56.4%), infections (28.2%) and others (15.4%)(3).
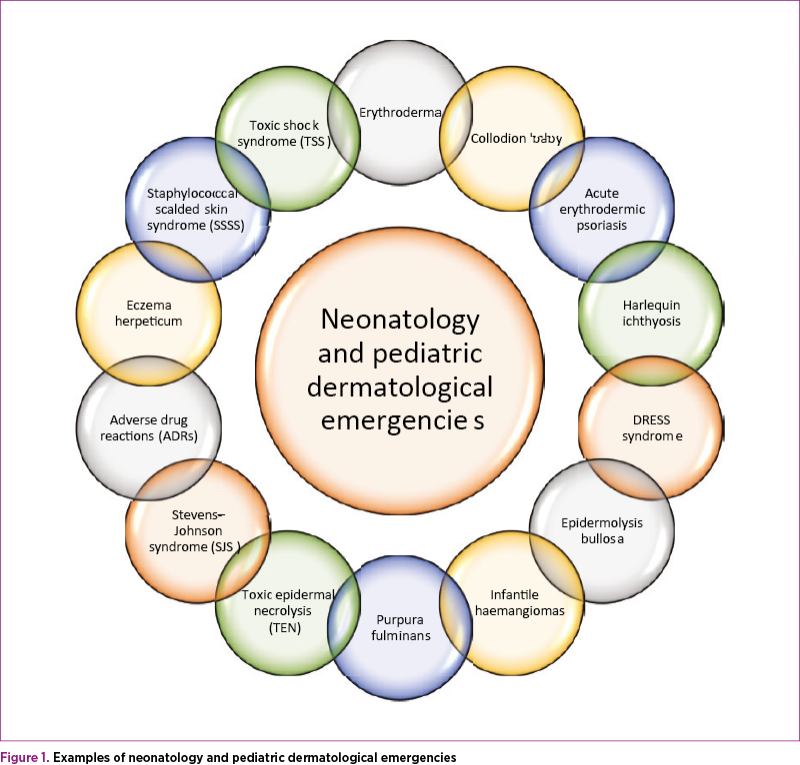
Although it is a long list of dermatological emergencies, we will treat some of these diseases separately.
Erythroderma
Erythroderma (exfoliative dermatitis) is a generalized inflammatory disease with metabolic, hemodynamic and thermal implications. Erythroderma should be mentioned because it puts lives at risk; however, it occurs in less than 1% of cases of pediatric dermatology(4).
The etiology disease in a child may be hereditary or acquired. Hereditary: keratom malign, Sjöngren-Larsson syndrome, Rud syndrome, Netherthon syndrome, congenital bullous erythroderma, rubella pilaris congenital pitiriasis. Acquired: Ritter von Rittersheim erythrodermia, Leiner Moussous erythroderma, toxic erythroderma, erythroderma of the Letterer-Siwe disease, erythroderma due to preexisting dermatoses such as psoriasis, mastocytosis, atopic dermatitis, lichen(5,6). However, there are situations where the etiology remains unknown.
Erythroderma covers over 90% of the skin surface and the patient may have pruritus, cold sensation, fever over 390C, increased basal metabolism, red to violet skin, edema can lead to vesicles, scaling occurs in 4-5 days or at 10-15 days, the skin is fattened, the patient may have chelation, stomatitis or conjunctivitis, hyperkeratosis of palms and soles and cracks. Most often, lymphadenopathy or splenomegaly occur(5,7).
Among complications we include: hydroelectrolytic disorders, respiratory failure, heart failure, cachexia, renal failure, predisposition to infection. The presence of complications can cause a poor prognosis for the patient(8).
Treatment is done with corticotherapy, but not when erythroderma is caused by psoriasis. Thermal comfort, hydroelectrolytic rebalancing, antibiotherapy, antipruriasis must be ensured(9).
Collodion baby
Collodion baby (congenital ichthyosis) is a condition that occurs at birth, especially preterm. It is inherited by autosomal recessive genes and affects both sexes. The baby is wrapped in a glowing membrane that begins to crack in 48 hours and within a few days there is a generalized squamous erythema.
Collodion babies require intensive care; they need to stay in an incubator to regulate water and heat loss. The treatment consists of frequent application of moisturizers and mouth care, because the lips can become painful, but also the eyes that can dry out(10,11).
Most patients evolve into various types of congenital ichthyosis, such as transglutaminase-1 deficient lamellar ichthyosis, trichotiodistrophy, Sjögren-Larsson’s syndrome or Gaucher disease(12).
Even though mortality occurs in 10% of cases(10), most cases spontaneously heal in the first few weeks of life.
Acute erythrodermic psoriasis
Acute erythrodermic psoriasis is a serious form of psoriasis with high risk of mortality and difficult to treat. It may be a new psoriasis or a complication of a preexisting psoriasis(13,14).
Skin manifestations can be: erythema, edema, generalized pruritus, intense desquamation, nail and hair damage(15). Systemic manifestations: obviously altered general condition, fever, chills, heart failure(16).
Although more than 25% of cases are due to psoriasis, it is important to make a differential diagnosis with other causes of erythroderma(17); if necessary, skin biopsy can be performed.
Regarding the treatment of erythrodermic psoriasis, the most commonly used methods are systemic retinoid, methotrexate, and cyclosporine(18). The decision to implement the treatment and the monitoring should be done in a multidisciplinary team from which the dermatologist should not miss.
Toxic shock syndrome (TSS)
The toxic shock syndrome is determined by an immune reaction caused by the deficiency of antibodies against the streptococcal or staphylococcal toxin.
At birth, S. aureus can be transmitted from an intrauterine or acquired infection during delivery. The most common risk factor of toxic shock syndrome in pediatrics is varicella, that can lead to group A streptococcal skin infection, favoring the onset of toxic shock syndrome(4).
Symptoms of toxic shock may be: faster influenza flu symptoms, skin reaction mimicking sunburn, erythroderma, skin necrosis, desquamation (during healing, days 7-14), fever, vomiting, diarrhea, syncope, hypotension, sepsis. It can cause complications of the lungs, liver and kidneys. Possible major complications: acute respiratory distress syndrome, disseminated intravascular coagulation, renal failure(19).
The diagnosis is clinical, usually the serum levels of transaminases, bilirubin and creatinine being increased. Differential diagnosis is done with Gram-negative septic shock, staphylococcal toxic shock syndrome, severe dengue.
Because toxic shock syndrome has a rapid evolution, therapy should be initiated as soon as possible. Intravenous fluids, oxygen therapy and intravenous antibiotics are given.
Mortality occurs in 30-70% of cases, sometimes even in cases where treatment has been established correctly(20).
DRESS syndrome
DRESS syndrome (Drug Reaction with Eosinophilia and Systemic Symptoms) is also known as hypersensitivity reaction. It is a condition endangering the patient’s life, with organ dysfunctions.
Dress syndrome is due to drug reactions, most often found as a delayed reaction to antiepileptic drugs(21).
The patient has a diffuse cutaneous eruption that can progress to erythroderma, lymphadenopathy, fever, visceral involvement, eosinophilia, and possibly atypical lymphocytes(21,22).
Systemic damage may include liver, kidneys, lungs and gastrointestinal disorders; later, patients may develop insipid diabetes, thyroiditis and adrenal insufficiency(23).
The differential diagnosis in children is made with infectious diseases, immunological diseases and neoplastic diseases.
Immediate patient hospitalization and stopping therapy that triggered the syndrome are required. It is usually necessary to administer systemic corticosteroids for a short period of time; antipyretics and topical corticosteroids may also be used.
The administration of intravenous immunoglobulins has been shown to be ineffective(24).
Purpura fulminans
Purpura fulminans is a life-threatening condition, being a hematological emergency. It is a very severe infection with a high mortality rate, the most severe and most common form being caused by meningococcus.
The patient presents the destruction of soft tissues and necrotic lesions that may even include the bones. Due to the alteration of endothelial vascular function, thrombotic and hemorrhagic lesions increase(25).
For treatment use: antibiotics, corticoids, vascular filling and catecholamines; depending on the evolution, between 10 days and 3 weeks, the necrotic lesions will be debrided and if an amputation is necessary, the psychological counseling of the child will be mandatory(26).
From the point of view of complications, there is a great possibility of organ failure and the skin will change very rapidly from scattered petechiae to gangrene(27).
Conclusions
Although intensive management and care are the responsibility of the pediatrician, it is necessary to collaborate with the dermatologist for diagnosis confirmation, disease prevention and early treatment of life-threatening conditions.
Conflict of interests: The authors declare no conflict of interests.
Bibliografie
1. Schachner LA, Hansen RG. Preface. In: Pediatric Dermatology, 2nd ed. Eds. Schachner LA, Hansen RC. New York, Churchill Livingstone. 1995; p IX.
2. Landolt B, Staubli G, Lips U, Weibel L. Skin disorders encountered in a Swiss paediatric emergency department. Swiss Med Wkly. 2013; 143:w13731, 1-6.
3. Sarkar R, Basu S, Patwari AK, Sharma RC, Dutta AK, Sardana K. An Appraisal of Pediatric Dermatological Emergencies. Indian Pediatrics. 2000; 37:425-429.
4. Rashid R, Goodyear H. Management of paediatric dermatological emergencies. Paediatrics and Child Health. 2015; Volume 25, Issue 2, 2015, Pages 78-83.
5. Pătraşcu V. Eritrodermia ichtioziformă congenitală non-buloasă. In: Boli dermatologice şi infecţii sexual-transmisibile. Ed Sitech. 2014; ed a-3-a: 379-380.
6. Cesar A, Cruz M, Mota A, Azevedo F. Erythroderma. A clinical and etiological study of 103 patients. Journal of Dermatological Case Reports. 2016; 10(1):1-9.
7. Pal S, Haroon TS. Erythroderma: a clinico-etiologic study of 90 cases. International Journal of Dermatology. 1998; 37:104-107.
8. Rothe MJ, Bialy TL, Grant-Kels JM. Erythroderma. Dermatol Clin. 2000; Jul 18(3):405-15.
9. Dobson JS, Levell NJ. Erythroderma. Medicine. 2017; Volume 45, Issue 7, pages 417-421.
10. Mason L. Challenges and learning points: A Colloidion baby. Journal of Neonatal Nursing. 2013; Volume 19, Issue 3, pages 91-93.
11. Raghunath R, Hennies HC, Ahvazi B, Vogel M, Reis A, Steinert PM, Traupe H. Self-Healing Collodion Baby: a Dynamic Phenotype Explained by a Particular Transglutaminase-1 Mutation. Journal of Investigative Dermatology. 2003; Volume 120, Issue 2, pages 224-228.
12. Lui K, Commens C, Chong R, Jaworski R. Collodion babies with Gaucher disease. Arch Dis Child. 1988; 63, pp. 854-856.
13. Stănescu AMA, Matei A, Grăjdeanu IV, Appiah EA, Giurcăneanu C. Multipli factori de interes în managementul psoriazisului şi comorbidităţilor asociate. Revista Practica Medicală. 2016; 11,1(43): 49-52.
14. Stănescu AMA, Grăjdeanu IV, Appiah EA, Bejan GC. Abordare diferenţiată a psoriazisului în funcţie de vârsta pacientului. Practica Medicală. 2017; Vol. 12, nr.4 (53); 204-207.
15. Stănescu AMA, Grăjdeanu IV, Diaconu C, Iancu MA, Stefani C. Evoluţia psoriazisului prenatal şi postnatal, afectarea fătului, modificări imune şi hormonale, tratament. Practica Medicală. 2018; Vol.13, Nr. 1(54); 36-40.
16. Stănescu AMA, Diaconu C, Iancu MA, Bejan GC, Stefani C, Grăjdeanu IV. Psoriazisul şi bolile cardiovasculare: Actualităţi în cercetarea medicală. Revista Medicală Română. 2018; vol. LXV, Nr. 1; 41-44.
17. Burton JL, Rook A, Wilkinson DS. Eczema, lichen simplex, erythroderma and prurigo. In: A. Rook, DS Wilkinson, FJG Ebling (Eds.), Textbook of dermatology (4th ed), Blackwell, Boston. 1986; pp. 367-418.
18. Dogra S, Mahajan R. Biologics in pediatric psoriasis – efficacy and safety. Expert Opinion on Drug Safety. 2018; 17:1, pages 9-16.
19. Burnham JP, Kollef MH. Understanding toxic shock syndrome. Intensive Care Med. 2015; 41: 1707-1710.
20. Demers B, Simor AE, Velland H, Schlievert PM, Byrne S, Jamieson F, et al. Severe invasive group A streptococcal infection in Ontario, Canada: 1987–1991. Clin Infect Dis. 1993; 16:792–800, 801–2.
21. Bosdure E, Cano A, Roquelaure B, Reynaud R, Boyer M, Viard L, Sarles J. Oxcarbazepine et syndrome DRESS: un cas pediatrique revele par une hepatite fulminante. Archives de Pediatrie. 2004; Volume 11, Issue 9, pages 1073-1077.
22. Fathallah N, Mlika A, Slim R, Larif S, Zayani H, Boughammoura L, Ben Salem C. Anticonvulsivant-induced dress syndrome in children: two cases. Clinical Therapeutics. 2015; volume 37, Issue 8, Supplement, page e53.
23. Ushigome Y, Kano Y, Ishida T, et al. Short- and long-term outcomes of 34 patients with drug-induced hypersensitivity syndrome in a single institution. J Am Acad Dermatol. 2012; May; 68(5):721-8.
24. Joly P, Janela B, Tetart F, et al. Poor benefit/risk balance of intravenous immunoglobulins in DRESS. Arch Dermatol. 2012; 148, pp. 543-544.
25. Nectoux E, Mezel A, Raux S, et al. Meningococcal purpura fulminans in children: initial orthopedic management. J Child Orthop. 2010; 4: 401-407.
26. Pasquesoone L, Belkhou A, Gottrand L, Guerreschi P, Duquennoy-Martinot V. Prise en charge des lesions des parties molles du purpura fulminans chez l’enfant. Annales de Chirurgie Plastique Esthetique. 2016; Volume 61, Issue 5, pages 605-612.
27. Nectoux E, Mezel A, Raux S, et al. Meningococcal purpura fulminans in children. II: Late orthopedic sequelae management. J Child Orthop. 2010; 4: 409-416.

Postbioticele – introducere, clasificare şi beneficii asupra sănătăţii
Simona Vlădăreanu, Mihai Cristian
Postbioticele sau paraprobioticele sunt produse bacteriene neviabile, metaboliţi care sunt secretaţi de bacteriile vii sau produşi eliberaţi după liza chimică ori mecanică a acestora, cum ar fi enzime, acizi organici sau...
Sarcină gemelară obţinută spontan versus sarcină gemelară obţinută prin FIV/ICSI – review al literaturii
Ana Maria Măreşescu, Simona Vlădăreanu, Silviana Mănăilă, Andreea Radu
Sarcina gemelară reprezintă o provocare pentru echipa medicală, dat fiind riscul crescut de complicaţii materno-fetale, fiind cea mai frecventă formă de sarcină multiplă....
Incontinentia pigmenti
Marilena Lefter, Daniela Sicoie, Carmen Ancăr, Roxana Bratu
Incontinentia pigmenti, cunoscută ca boala Bloch-Sulzberger, reprezintă o afecţiune genetică rară în lume, având o incidenţă de aproximativ 1 la 40000 de nou-născuţi. ...
Incontinentia pigmenti
Marilena Lefter, Daniela Sicoie, Carmen Ancăr, Roxana Bratu
Incontinentia pigmenti, cunoscută ca boala Bloch-Sulzberger, reprezintă o afecţiune genetică rară în lume, având o incidenţă de aproximativ 1 la 40000 de nou-născuţi. ...
O revizuire narativă despre asocierea dintre sindromul Sjögren și sarcină
Bianca Mihaela Danciu, Ana Maria Alexandra Stănescu, Mariana Vieru, Anca A. Simionescu
Sindromul Sjögren (SS) este una dintre cele mai frecvente boli sistemice autoimune care poate influența rezultatul sarcinii, iar sarcina poate influența evoluția acesteia. ...