Depression is one of the causes of a decline in the socioprofessional functioning and for decreased quality of life. Depression is often accompanied by other medical conditions. It is not known to what extent these medical conditions precede or lead to depression. The present study proposes to identify somatic comorbities in a group of patients with major depressive disorder. The results show that many of the comorbidities identified may be metabolic risk factors for the development of other diseases or may even predispose to depression, as suggested by other studies in the literature. Patients with multiple comorbidities have a much higher risk of depression, which requires the implementation of a depression screening program and monitoring of patients at risk. Early and effective treatment leads to a lower mortality rate.
Comorbidităţile asociate depresiei
Comorbidities associated with depression
First published: 18 aprilie 2022
Editorial Group: MEDICHUB MEDIA
DOI: 10.26416/Psih.68.1.2022.6308
Abstract
Rezumat
Depresia este una dintre cauzele care duc la declin în funcţionarea socioprofesională şi la scăderea calităţii vieţii. De multe ori, depresia este însoţită de alte condiţii medicale. Nu se cunoaşte în ce măsură aceste condiţii medicale preced sau duc la apariţia depresiei. Acest studiu îşi propune să identifice comorbidităţile somatice într-un lot de pacienţi cu tulburare depresivă majoră. Rezultatele arată că multe dintre comorbidităţile identificate pot fi factori de risc metabolic pentru dezvoltarea altor boli sau pot chiar să predispună la apariţia depresiei, aşa cum sugerează alte studii din literatura de specialitate. Pacienţii cu multiple comorbidităţi au un risc mult mai mare de apariţie a depresiei, ceea ce impune implementarea unui program de screening al depresiei şi de monitorizare a pacienţilor la risc. Un tratament precoce şi eficient duce la o rată mai scăzută de mortalitate.
Introduction
Depression is a major public health problem that leads to a decline in patients’ quality of life. Depression is one of the major causes of disability and recent data suggest that less than half of patients (even below 10% in some countries) receive effective treatment(1). According to epidemiological studies, the lifetime prevalence of depression is between 10% and 15%(2), affecting over 350 million people worldwide(3). Patients with depression and associated somatic disorders have a lower quality of life than the depressed patients who do not have somatic pathologies(4).
Multimorbidity is a term used to define the presence of two or more chronic diseases(5). Multimorbidity is more and more common in medical practice as a result of an aging population. The relationship between somatic disease and depression can be explained by the model of psychological and biological pathways, proposed by Schulberg and his collaborators. It is assumed that physical illness can lead to a decreased ability to use coping strategies, and together with neurochemical and neuroanatomical changes caused by the disease can lead to depressive symptoms(6). The risk of depression increases with each acquired chronic condition, regardless of gender, age or type of illness(7).
Depression and cardiovascular diseases are two-way conditions, which means the risks are reciprocal and often coexist. The prevalence rate of depression is 50% among patients with chronic diseases(8). Depression directly produces pathophysiological changes in various organ systems, altering the values of blood pressure, heart rate, vasomotor tone, vascular resistance, plasma volume and blood viscosity. Other potential mechanisms for the development of cardiovascular pathologies in patients with depression are represented by dysfunction of the hypothalamic-pituitary-adrenal axis, increased proinflammatory and prothrombotic factor activity, reduction of omega-3 fatty acids, smoking and physical inactivity(9). Depression is a common disorder among patients with cardiovascular disease, with a reported prevalence of 20% to 45%, which is much higher than in the general population(8).
The comorbidity between depression and type 2 diabetes seems to have an additive impact on an individual’s health. Thus, patients have an increased risk of mortality, have more disabilities and have a higher risk of job loss due to disabilities. Depression increases the risk of developing diabetes and, conversely, diabetes increases the risk of developing depression(10).
The link between thyroid dysfunction, affective disorders and cognitive disorders has long been studied(11,12). Hypothyroidism is a major cause of depression and can lead to the worsening of cognitive impairment in dementia(11). Associating thyroid hormones with antidepressant treatment is beneficial in comorbid depression with hypothyroidism(13).
Hematological disorders are also common in depression. The prevalence of anemia is higher among patients with mental disorders, including depression, compared to the general population(14). Iron deficiency anemia affects the quality of sleep and the symptoms of anxiety and depression(15). In addition, iron deficiency was associated with depressive symptoms in a study of 1875 elderly patients(16).
Methodology
The aim of this study was to identify somatic comorbidities associated with depression. This is a descriptive, retrospective study.
Using the AtlasMed database of the Psychiatry III Ward of the Cluj County Emergency Clinical Hospital, we analyzed the hospitalizations of patients with the main diagnosis of major depressive disorder, with single episode and major depressive disorder, recurrent (according to ICD-10 criteria), from the 1st of January 2018 to the 1st of April 2021. In the case of patients with multiple hospitalizations, the primary diagnosis at the first hospitalization was considered, and the secondary diagnoses were summed.
Sociodemographic data (age, sex, environment) and the main and secondary diagnoses were analyzed.
For the analysis of statistical data, the Statistical Analysis Tool of Microsoft Office Excel 2016 was used. The study protocol respects the confidentiality and is in accordance with the research rules, being approved by the local Ethics Commission.
Results
Between the 1st of January 2018 and the 20th of April 2021, there were reported 2395 hospitalizations. A total of 334 patients with the main diagnosis of major depressive disorder, single episode or major depressive disorder, recurrent, were hospitalized 475 times, totaling 5601 days of hospitalization.
The mean age was 51.06 years old, with the minimum age being 18 years old and the maximum being 82 years old. Regarding gender distribution, 61.38% of patients were females and 38.62% were males. Most patients came from urban areas (68.3%).
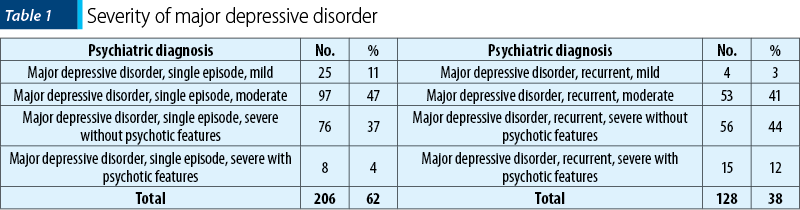
Regarding prognosis, 62% of patients had as primary diagnosis major depressive disorder, single episode, and 38% had as primary diagnosis recurrent depressive disorder. The prevalence of each episode of major depressive disorder is presented in Table 1.
Cardiovascular comorbidities have the highest prevalence (30%) among somatic comorbidities associated with depression, followed by nutritional and metabolic diseases (24%). Together, they account for more than half of the co-occurring disorders (Figure 1).
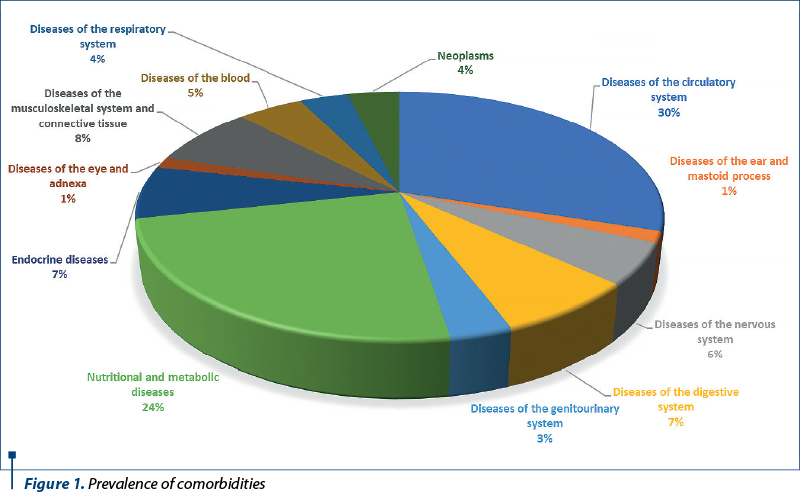
The third place is occupied by diseases of the musculoskeletal system and connective tissue (8%), followed by endocrine diseases and diseases of the digestive system, with an equal prevalence (7%). Neurological comorbidities have a prevalence of 6% and hematological comorbidities have a prevalence of 5%.
Neoplasms and diseases of the respiratory system have an equal prevalence of 4%, followed by diseases of the genitourinary system, with a prevalence of 3%. On the last place, there are the diseases of the eye and adnexa and diseases of the ear, with an equal prevalence of 1%.
Among diseases of the circulatory system, essential hypertension ranks first, with a prevalence of 51% (n=138), followed by ischemic heart diseases and valvulopathies, with an equal prevalence of 15% (n=40, respectively n=39). Peripheral venous diseases have a prevalence of 5% (n=14). Left ventricular failure and rhythm and conduction disorders have a prevalence of 4% (n=10), followed by congestive heart failure, with a prevalence of 3% (n=8). Hypertensive heart disease has a prevalence of 2% (n=6). Secondary hypertension has the lowest prevalence, only 1% (n=4).
Among the nutritional and metabolic disorders, the most common one is obesity, with a prevalence of 30% (n=66), followed by mixed hyperlipidemia, with a prevalence of 18% (n=39). Diabetes has a prevalence of 21% (n=45); 56% of patients have type 2 diabetes without complications, and 44% have type 2 diabetes with complications (diabetic polyneuropathy, proliferative retinopathy, poor control etc.). Essential hypercholesterolemia has a prevalence of 16% (n=35), followed by essential hyperglyceridemia, with a prevalence of 10% (n=21). On the penultimate place there is hyperuricemia, with a prevalence of 3% (n=7), followed by malnutrition (2%).
Diseases of the musculoskeletal system represent the third most common comorbidities associated with depression. The most common musculoskeletal pathology is spondylosis, with a prevalence of 26% (n=18). The most common location of spondylosis is lumbar (56%), followed by the cervical region (33%) and the thoracic region (11%). On the second place, there are osteoporosis and scoliosis, with a prevalence of 17%, followed by primary hip osteoarthritis (15%) and primary gonarthrosis (7%). Gout, polyarthritis and lumbago with sciatica have an equal prevalence (4%). The last one is sciatica, with a prevalence of 3%.
Gastroenterological comorbidities have a prevalence of 7% among patients with depression. The most common gastroenterological pathology is alcoholic hepatitis, with a prevalence of 26% (n=17). On the second place, there are chronic superficial gastritis, with a prevalence of 14% (n=9), and gastroesophageal reflux disease, with an equal prevalence. On the third place, there are alcoholic fatty liver disease, with a prevalence of 12% (n=8), followed by chronic gastric ulcer, with a prevalence of 11% (n=7). Neurogenic bowel and diverticulosis of the large intestine have an equal prevalence of 9% (n=6). Alcohol-induced chronic pancreatitis has a prevalence of 4%, and on the last place there is gastrojejunal ulcer (1%).
Among the endocrine diseases associated with depression, the most common is hypothyroidism, with a prevalence of 52% (n=32), followed by autoimmune thyroiditis, with a prevalence of 26% (n=16). On the third place, there is the nontoxic multinodular goiter (8%), and on the fourth place there is the nontoxic diffuse goiter (6%). Hypothyroidism due to medicaments and other exogenous substances has a prevalence of 5%. On the last place, there is thyrotoxicosis (3%).
Neurological comorbidities have a prevalence of 6%, the most common one being alcoholic polyneuropathy, with a prevalence of 17% (n=8), followed by generalized idiopathic epilepsy, with a prevalence of 13% (n=6). On the third place there are Parkinson’s disease and radiculopathies, with an equal prevalence (10%). On the fourth place, there are essential tremor, focal idiopathic epilepsy, cerebral cyst and transient cerebral ischemic attack, with a prevalence of 8% (n=4). Vertebro-basilar artery syndrome (with a prevalence of 6%) is followed by migraine without aura, multiple sclerosis and secondary parkinsonism, with an equal prevalence of 4%.
Iron deficiency anemia has the highest prevalence among hematological comorbidities (43%), followed by vitamin B12 deficiency anemia (18%). On the third place, there are folate deficiency anemia and secondary thrombocytopenia, with a prevalence of 14% (n=6). Refractory anemia has a prevalence of 9% (n=4), followed by essential thrombocytopenia (2%).
Among the patients who were diagnosed with a tumor, 59% had a benign tumor (the most common being uterine leiomyoma, with a prevalence of 23%, followed by benign stomach tumor). The remaining 41% of patients were diagnosed with a neoplasm, the most common being a malignant tumor of the prostate, with a prevalence of 17%, followed by a malignant tumor of the ovary, with a prevalence of 9%. On the third place there are malignant tumors of the thyroid and lung, with an equal prevalence (3%). More information about the prevalence of other neoplasms and benign tumors cand be found in Table 2.
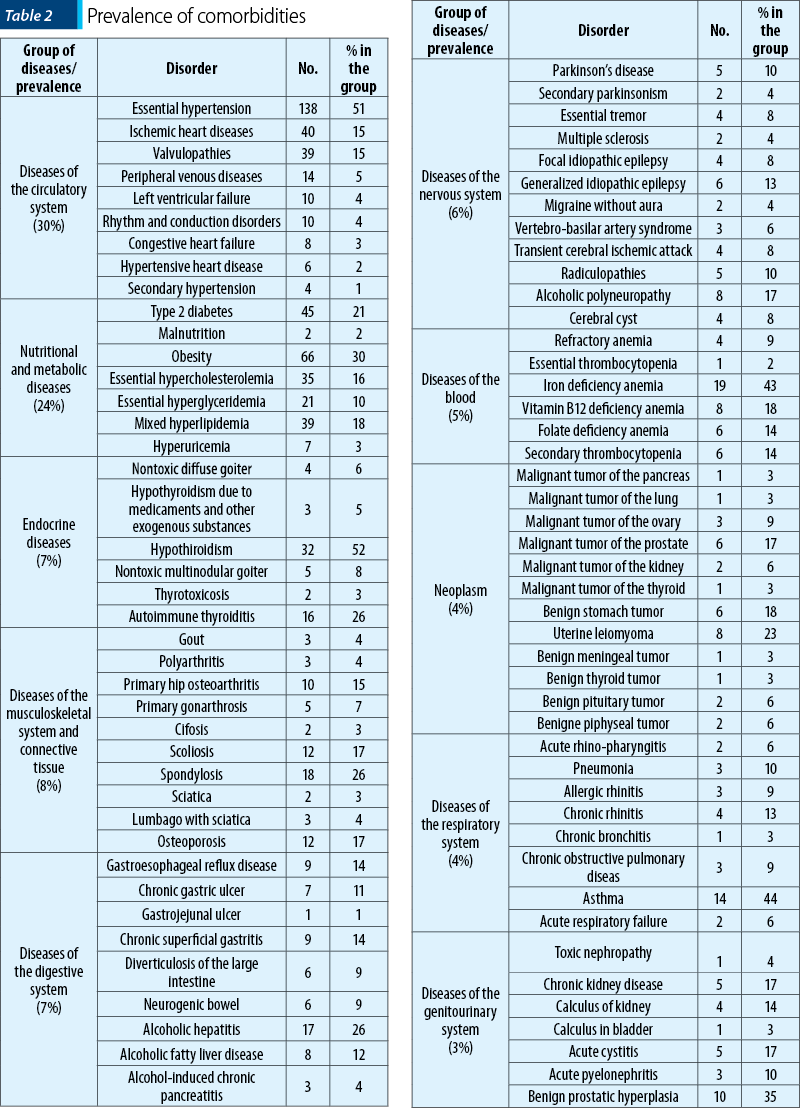
The most common disease of the respiratory system in patients diagnosed with depression was asthma, with a prevalence of 44% (n=14). On the second place there is chronic rhinitis (13%), followed by pneumonia (10%). Allergic rhinitis and chronic obstructive pulmonary disease have an equal prevalence (9%). Acute rhinopharyngitis and acute respiratory failure have a prevalence of 6%. The last place is occupied by chronic bronchitis, with a prevalence of 3%.
The most common urological comorbidity among patients with depression is benign prostatic hyperplasia, with a prevalence of 35% (n=10), followed by acute cystitis and chronic kidney disease, which have a prevalence of 17% (n=5). On the third place there is calculus of kidney, with a prevalence of 14%, followed by acute pyelonephritis, with a prevalence of 10% (n=3). Toxic nephropathy has a prevalence of 4% and calculus in bladder has a prevalence of 3%.
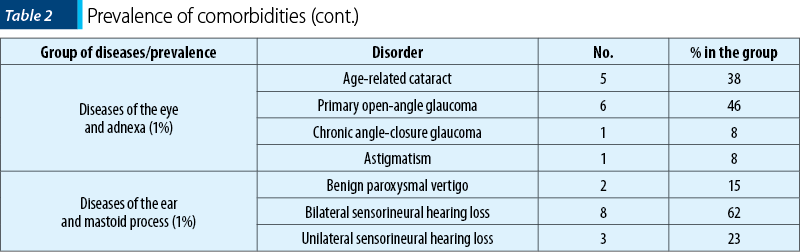
Diseases of the eye and ear (ENT) have the lowest share among somatic comorbidities, with a prevalence of only 1% each. The most common disease of the eye is primary open-angle glaucoma (46%), followed by age-related cataract (38%). Chronic angle-closure glaucoma and astigmatism have a prevalence of 8% (n=1). Bilateral sensorineural hearing loss has the highest prevalence among ENT pathologies, respectively 62%, followed by unilateral sensorineural hearing loss (23%) and benign paroxysmal vertigo (15%).
Discussion
The risk of depression is twice as high among people with multiple comorbidities, compared to people who have only one comorbidity, and three times higher than in people without associated somatic pathology(17). With each additional somatic pathology, the chances of developing a depressive disorder are 45% higher(17).
Comorbid depression should be treated vigorously and serotonin reuptake inhibitors (SSRIs) were shown to have beneficial effects not only in relieving symptoms depression, but also in inactivating blood platelets and in reducing inflammation, thus reducing cardiovascular morbidity and mortality(18). Early diagnosis of depression in patients with cardiovascular disease, especially in those with a history of myocardial infarction, and starting the treatment with SSRI in combination with psychotherapy significantly prolong the patient’s life and improve its quality(19).
Depression and cardiovascular disease (CVD) coexist in many cases. Depression is a common disorder in cardiovascular patients, with a prevalence of 20% to 45%(8). The present study identified a 30% prevalence of CVD among patients with depression, similar to previous studies. The most common cardiovascular pathology identified in this group was essential hypertension. Clinical and epidemiological studies have shown that the presence of depression and its severity are closely correlated with the prognosis of hypertensive patients. Adamis and colleagues have shown that the incidence of depression is higher in patients with high blood pressure and depressive disorder is associated with high blood pressure(17).
Depression increases the risk of coronary heart disease by 1.5-2 times in the clinically healthy population(20). Among patients with coronary heart disease, depression increases the risk of myocardial infarction by 1.5-4.5 times(21,22). In this study, 15% of patients with cardiovascular disease had ischemic heart disease, of which only 5% had a history of myocardial infarction.
The prevalence rate of depression is three times higher among patients with type 1 diabetes (12%) and twice as high among patients with type 2 diabetes (19.1%)(23). The prevalence of diabetes and metabolic diseases was 24% in the present study. Endocrine comorbidities had a prevalence of 7%. Depression and obesity are important public health issues. Several longitudinal studies have established that obesity is a risk factor for affective disorders and vice versa(24). Obesity (n=66) ranks second among nutritional and metabolic disorders, followed by mixed hyperlipidemia (n=39).
Many of the comorbidities associated with depression are metabolic risk factors for cardiovascular disease and lead to an increased risk of mortality and early morbidity.
Conclusions
It remains unclear to what extent somatic pathologies influence the onset of depressive disorder. Being a retrospective study, we do not have data on the history of the diseases (onset of depression, onset of associated pathologies, the existence of a temporal link between them).
Longitudinal studies in which patients diagnosed with major depressive disorder (with single episode or recurrent) are closely monitored, in order to identify the appearance of somatic comorbidities, are needed. It is necessary to identify and monitor patients with somatic diseases at risk of developing secondary depression, as well as to develop and implement national screening programs. Physicians in other specialties should be informed on the need to identify depressive symptoms in patients and trained in applying depression screening scales, for an early intervention and increased effectiveness of treatment.
Early treatment of depression, in combination with the treatment of comorbidities, can decrease mortality and increase the patients’ quality of life.
Bibliografie
-
Zhang Y, Chen Y, Ma L. Depression and cardiovascular disease in elderly: Current understanding. J Clin Neurosci. 2018 Jan;47:1-5. doi: 10.1016/j.jocn.2017.09.022.
-
Lépine JP, Briley M. The increasing burden of depression. Neuropsychiatr Dis Treat. 2011;7(Suppl 1):3-7. doi:10.2147/NDT.S19617.
-
Marcus MD, Yasamy T, van Ommeren M, Chisholm D, Saxena S. Depression: A global public health concern, World Federation of Mental Health. WHO, 2012.
-
Moussavi S, Chatterji S, Verdes E, Tandon A, Patel V, Ustun B. Depression, chronic diseases, and decrements in health: results from the World Health Surveys. Lancet. 2007;370(9590):851-858. doi:10.1016/S0140-6736(07)61415-9.
-
van den Akker M, Buntinx F, Roos S, Knottnerus JA. Problems in determining occurrence rates of multimorbidity. J Clin Epidemiol. 2001;54(7):675-679. doi:10.1016/s0895-4356(00)00358-9.
-
Schulberg HC, Schulz R, Miller MD, Rollman B. Depression and physical illness in older primary care patients: Diagnostic and treatment issues. In: Williamson GM, Shaffer DR, Parmelee PA (Eds.). Physical illness and depression in older adults. New York, 2020, 239-256.
-
Gunn JM, Ayton DR, Densley K, Pallant JF, Chondros P, Herrman HE, Dowrick CF: The association between chronic illness, multimorbidity and depressive symptoms in an Australian primary care cohort. Soc Psychiatry Psychiatr Epidemiol. 2012;47(2):175–184.
-
Raič M. Depression and Heart Diseases: Leading Health Problems. Psychiatr Danub. 2017 Dec;29 Suppl 4(Suppl 4):770-777.
-
Jantaratnotai N, Mosikanon K, Lee Y, McIntyre RS. The interface of depression and obesity. Obes Res Clin Pract. 2017 Jan-Feb;11(1):1-10. doi: 10.1016/j.orcp.2016.07.003.
-
The World Health Organization. The Global Burden of Disease: 2004 Update. 2008.
-
Rack SK, Makela EH. Hypothyroidism and depression: a therapeutic challenge. Ann Pharmacother. 2000;34(10):1142-1145. doi:10.1345/aph.10022.
-
Whybrow PC, Prange AJ Jr, Treadway CR. Mental changes accompanying thyroid gland dysfunction. A reappraisal using objective psychological measurement. Arch Gen Psychiatry. 1969;20(1):48-63. doi:10.1001/archpsyc.1969.01740130050004.
-
Villar HC, Saconato H, Valente O, Atallah AN. Thyroid hormone replacement for subclinical hypothyroidism. Cochrane Database Syst Rev. 2007;2007(3):CD003419.
-
Korkmaz S, Yildiz S, Korucu T, et al. Frequency of anemia in chronic psychiatry patients. Neuropsychiatr Dis Treat. 2015;11:2737-41.
-
Murat S, Ali U, Serdal K, et al. Assessment of subjective sleep quality in iron deficiency anaemia. Afr Health Sci. 2015;15:621-7.
-
Stewart R, Hirani V. Relationship between depressive symptoms, anemia, and iron status in older residents from a national survey population. Psychosom Med. 2012;74:208-13.
-
Read JR, Sharpe L, Modini M, Dear BF. Multimorbidity and depression: A systematic review and meta-analysis. J Affect Disord. 2017;221:36-46. doi:10.1016/j.jad.2017.06.009.
-
Boden JM, Fergusson DM. Alcohol and depression. Addiction. 2011 May;106(5):906-14. doi: 10.1111/j.1360-0443.2010.03351.x.
-
Filaković P. Terapija depresija kod bolesnika s komorbiditetom. Medicus. 2014;13:59-67.
-
Lett HS, Blumenthal JA, Babyak MA, Sherwood A, Strauman T, Robins C, et al. Depression as a risk factor for coronary artery disease: evidence, mechanisms, and treatment. Psychosom Med. 2004;66(5):305–15.
-
Pratt LA, Ford DE, Crum RM, Armenian HK, Gallo JJ, Eaton WW. Depression, psychotropic medication, and risk of myocardial infarction. prospective data from the Baltimore ECA follow-up. Circulation. 1996;94(12):3123–9.
-
Aromaa A, Paitasalo R, Reunanen A, Impivaara O, Heliovaara M, Knekt P, et al. Depression and cardiovascular disease. Acta Psychiatr Scand. 1994;377(S):77–82.
-
Roy T, Lloyd CE. Epidemiology of depression and diabetes: a systematic review. J Affect Disord. 2012 Oct;142 Suppl:S8-21. doi: 10.1016/S0165-0327(12)70004-6.
-
Jantaratnotai N, Mosikanon K, Lee Y, McIntyre RS. The interface of depression and obesity. Obes Res Clin Pract. 2017 Jan-Feb;11(1):1-10. doi: 10.1016/j.orcp.2016.07.003.
Articole din ediţiile anterioare
Evaluarea multidimensională a demenţelor. Rolul scalelor clinice în managementul de caz
Deși au fost concepute multiple scale clinice pentru evaluarea demențelor, doar o parte dintre ele sunt utilizate frecvent în practica clinică sau ...
Integrarea datelor farmacogenetice în practica psihiatrică
Medicina personalizată este un deziderat care prezintă avantajele unei eficacităţi sporite şi ale unei tolerabilităţi superioare, aspecte care ar î...
Importanţa reintegrării sociale în cazul pacienţilor cu tulburare depresivă majoră
Tulburarea depresivă majoră este principala cauză a dizabilităţii la nivel mondial, aceasta fiind asociată cu tulburări de consum de substanţe, num...
Aspecte de diagnostic şi tratament al tulburărilor asociate stresului profesional la personalul medical în contexul pand
Profesioniştii din domeniul sănătăţii se confruntă cu numeroşi factori de stres în practica de zi cu zi, iar datele existente în literatură arată o...