Depression represents one of the most important burden sources at the global level, bearing significant costs on the society. A major component of these costs is defined by the social dysfunctions and the impact they have at the individual and collective level. In this context, our aim was represented by a comparative assessment of the role the coping mechanisms play on the level of global functioning of patients with major depression disorder under usual antidepressant medication, augmented by cognitive behavioral psychotherapy. The rehabilitation of psychosocial functioning of depressive patients is significantly influenced by cognitive coping mechanisms such as acceptance, rumination or putting into perspective. Thus, the multidisciplinary therapeutic approach becomes a certainty, which would lead to a fast recovery of the depressive person from the clinical and functional point of view.
Strategiile de coping şi funcţionarea globală în depresia majoră
Coping strategies and global functioning in major depression
First published: 20 noiembrie 2021
Editorial Group: MEDICHUB MEDIA
DOI: 10.26416/Psih.67.4.2021.5730
Abstract
Rezumat
Depresia reprezintă una dintre cele mai importante surse de povară la nivel global, impunând costuri semnificative asupra societăţii. O componentă majoră a acestor costuri este reprezentată de disfuncţionalităţile sociale şi de impactul pe care acestea îl au la nivel individual şi colectiv. În acest context, am urmărit evaluarea comparativă a rolului pe care mecanismele de coping îl joacă asupra nivelului de funcţionare globală a pacienţilor depresivi aflaţi sub terapie medicamentoasă augmentată cu intervenţie psihoterapeutică. Reabilitarea funcţionării psihosociale a pacienţilor depresivi este influenţată semnificativ de mecanisme precum acceptarea, ruminaţia sau punerea în perspectivă. Astfel, abordarea terapeutică multidisciplinară devine o necesitate, care ar conduce la o recuperare rapidă a persoanei afectate din punct de vedere clinic şi funcţional.
Introduction
Depression is currently defined as one of the most important public health problems, due to the impact the disorder symptoms have at the individual level, symptoms that determine a high degree of disability, as well as due to the complexity of the therapeutic management process, that requires now a multidisciplinary treatment and in most cases for a long term.
An important characteristic of this disorder, representing one of the main sources of the imposed social and economic burden, is its frequent association with other medical or psychiatric conditions, this real ubiquity determining significant increases of care costs.
Considered one of the main world contributors to the illness burden, expressed in years lived with disability, morbidity and premature mortality, depression has already surpassed the illnesses regarded so far as major sources of disability, such as cardiovascular diseases, hyperglycemia, arthritis or cervical diseases(1,2).
At the individual level, the depressive disorder decreases significantly the quality of life for the affected persons, through the numerous dysfunctionalities and disabilities affecting directly the family, the professional and financial status, thus contributing to the alteration of social roles the person had prior to the onset of the disorder.
The epidemiological studies estimate that 4.4% of the global population is affected by depression (between 5% and 10% at the European level), more frequently found in women (5.1% of the total), compared with men (3.6%), mainly in the age interval 55-74 years old, but all these values record a continuous increase(3-5).
The specificity of the depression makes this disorder to be frequently interpreted as an emotional reaction to an adverse psychosocial context, where more factors gain etiopathogenic features, with a predominance of etiologic models reported to the stress diathesis perspective(6-8), both related to the exposure to acute forms of stress (especially psychotraumatic events), as well as long-term stress exposure, with impact on the individual’s coping capacity.
The importance of the socioeconomic status is decisive in the progress of the depressive disorder(9), its positioning among disadvantaged categories from this perspective leading initially to chronic stress and consequently to depression(10,11). This context includes the persons vulnerable to gender or race discrimination, translated in socioeconomic impact as well as by loss of self-esteem, both phenomena being responsible for the onset of mood disorders, especially depression(12). Thus, the institutional and sociocultural barriers play an important role in setting the conditions for long-term stress, as they put in place disparities between individuals and, even more, contribute to a lower accessibility to mental health services(13).
Cognitive coping strategies play a significant role among the etiopathogenic mechanisms in depression, mentioning here the classical cognitive model, drafted by Beck, which includes the negative visions of self, the world and the future(14), the depressive cognitive styles specific to hopelessness(15) and the information processing perspectives(16).
Regarding the vulnerability induced by interpersonal relations, among which marital and parental problems, domestic violence, lack of emotional attachment or social support, there is also a reciprocity relation, meaning that the aforementioned elements represent risk factors for depression and, in turn, the depressive symptoms contribute to the amplification of their action. Irritability, fatigability, anhedonia, exacerbated pessimism or even suicidal ideation represent amplifying factors for the networking deficiencies, thus leading to the loss of social support(17,18).
Marital dysfunctionalities are significantly and bilaterally associated with depression(19,20), since the single or divorced persons are predominant among those with depressive predisposition(21), while depressed individuals are more frequently faced with negative interaction with their partners(22,23). In addition, the duration and frequency of depressive episodes represent a negative prediction factor for the quality of the couple relationship(24,25).
Domestic violence is a major risk factor for an entire spectrum of psychiatric illnesses(26, 27), but in the case of depression there is a higher frequency of up to 47%(28). Violent acts lead to vulnerability for the onset of depression, combined with the assimilation of maladaptive coping mechanisms and a tendency towards isolation(29), amplified especially in the case of violence towards the mother or in violent maternal behavior(30). Consequently, the vulnerability potential for depression is transmitted to the children, as there is sufficient evidence to correlate the marital problems and the violent behavior with the onset of depression in children and teenagers or creating a depressive background for the adult(31).
Another relevant aspect was distinguished regarding the social networking, namely that persons with a predisposition for depression tend to make couple with individuals who also have psychological problems, especially antisocial personality disorders or abusive consumption of substances, thus amplifying the marital problems and the risk for developing mental health disorders(32,33).
The lack of social support and the loss of social networking contribute both to the onset of depression and to its recurrence due to the increased number and frequency in episodes(34,35), especially in case of individuals with a predisposition for isolation, introverted and behaviorally inhibited or who do not have social networking skills. In their case, we can also see a bidirectional relation between this behavioral typology, contributing to the onset of depression, and the disorder itself, which in turn amplifies the negative perceptions over self and the quality and efficiency of relationships and social support(36,37).
Methodology
The aim of our research was the comparative assessment of the role played by cognitive coping mechanisms on the level of global functioning in depressive patients benefitting from pharmacotherapy, respectively subjects for which the medication therapy was augmented with cognitive‑behavioral psychotherapeutic interventions. In this respect, we considered two groups of patients diagnosed with major depressive disorder (according to ICD-10 criteria), admitted in the period 1st of January 2017 – 31st of December 2019 in the Psychiatric Clinic I Craiova:
-
Group M = 136 patients treated only with psychotropic medication according to current guides and protocols.
-
Group P = 137 subjects who, besides medication therapy, received a cognitive‑behavioral psychotherapeutic intervention performed by the psychologist psychotherapist in the clinic.
Besides the sociodemographic and clinical indicators, we also monitored the level of global functioning and social adjustment at the moment of admission (inclusion in the study) and after 12 weeks, using the Global Assessment of Functioning (GAF) questionnaire, respectively the identification of the cognitive emotional coping strategies by using the Cognitive Emotional Regulation Questionnaire (CERQ).
The data were collected in a prospective manner from the medical documentation of each patient, as well as by applying the work instruments, while for their processing we used Microsoft Excel (Microsoft Corp., Redmond, WA, USA), together with XLSTAT suite for MS Excel (Addinsoft SARL, Paris, France).
The study was performed in accordance with the provision of the Declaration of Helsinki and was approved by the Ethics Committee of the University of Medicine and Pharmacy of Craiova. All participants in the study were volunteers, based on informed consent, and the collection and storage of data respected the rules for anonymity and security.
Results
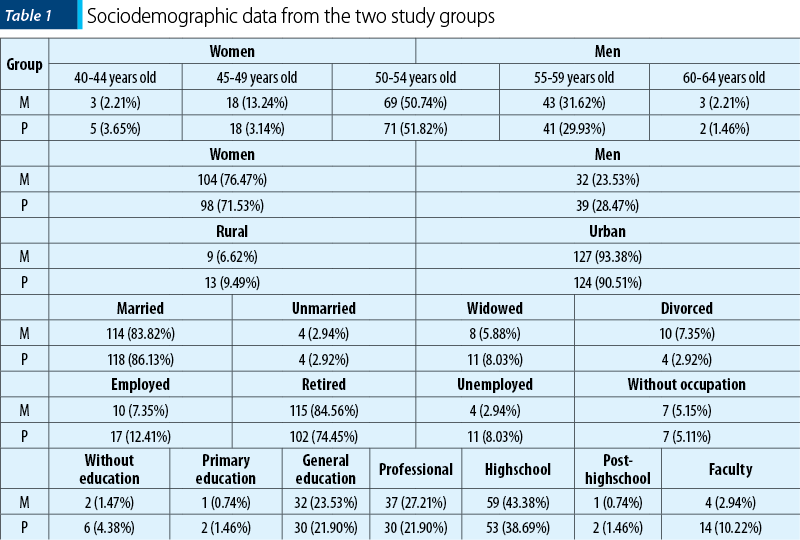
The sociodemographic data for the two groups were approximately similar, without statistically significant differences, an aspect that leads to a better comparison of the results from the two therapeutic approaches and the results of the psychometric instruments used. Therefore, we recorded close values for the subjects’ average age, with a predominance of the 50-54 years old age interval in both groups. Also, a ratio of 3 to 1 for women was observed, regarding the subjects’ gender distribution, as well as a majority of urban residence (93.38% for group M, respectively 90.51% for group P). Related to the marital status, we noted that most subjects were involved in a relationship (83.82% for group M, 86.13% for group P), but with a very reduced involvement in professional activities (7.35% for group M, 12.41% for group P). Regarding the educational level expressed as the latest graduated levels, the predominant ones were general, highschool and professional education (70.59% for group M, 60.59% for group P) – Table 1.
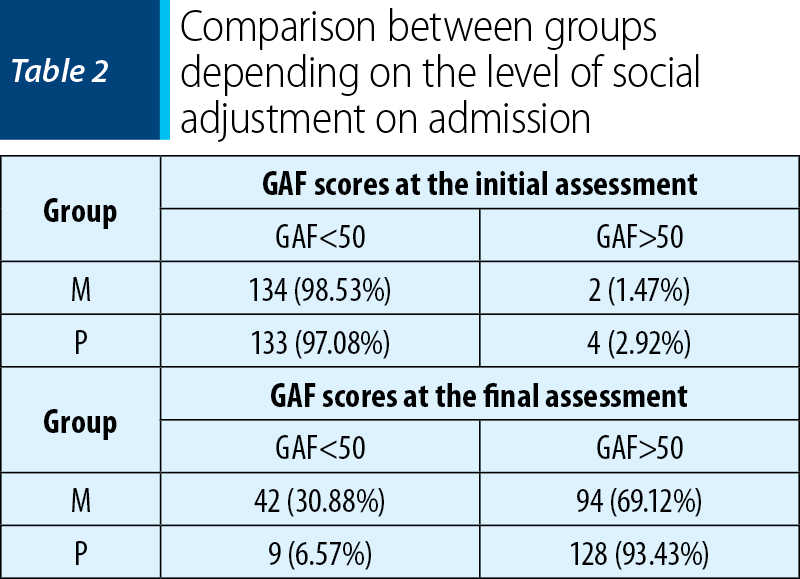
The level of functionality and social adjustment on initial (admission) and final assessments were evaluated with GAF scale and quantified according to the adverse scores (GAF score <50), respectively positive scores (GAF score >50). Therefore, the GAF scores recorded for both groups demonstrated the impact of depression on the ability to function and social networking of the affected individuals (98.53% for group M, respectively 97.08% for group P) (pχ2 = 0.414, p>0.05), the statistical analysis showing a highly significant statistical difference between the two groups (pχ2 = 2.558E-07, p<0.001). Then it was noted that the social skills of the subjects from group P have clearly improved from the perspective of GAF scores obtained by the majority of subjects (93.43%), probably as a result of the cognitive‑behavioral training, compared with only 69.12% in group M that benefited only from medication therapy (Table 2).
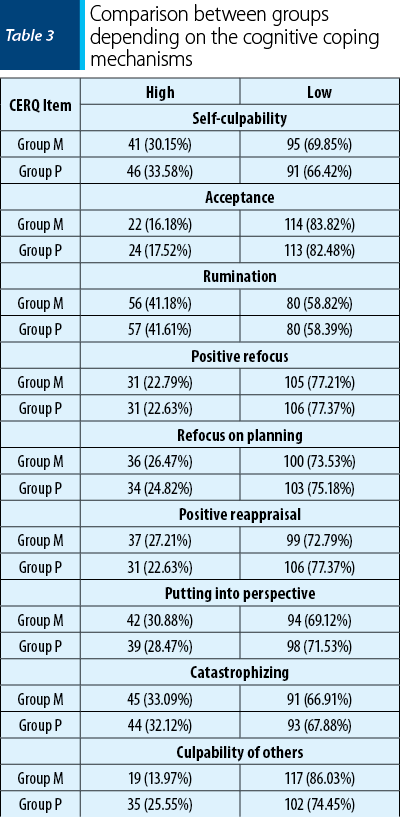
With CERQ we identified the extent to which a person uses adaptative or maladaptive coping strategies, when faced with events that negatively influence the individual’s psychological status. Highlighting these mechanisms is required since it facilitates the choice of a certain therapeutic approach, either pharmacologic or psychotherapeutic, as well as for the investigation of the relationship between these defense mechanisms and personality traits or psychic disorders. This multidimensional questionnaire distinguishes, based on 36 items, nine different types of cognitive coping strategies that a person uses consecutive to negative events or life situations, evaluating exclusively that person’s thoughts. The results of the test were grouped in two levels, according to the values obtained on each scale, in high, respectively low, referring to the frequency of using the respective coping strategy, with the following results in both groups.
-
Self-culpability – thoughts of taking the guilt for the negative event: low (69.85% for group M; 66.42% for group P).
-
Acceptance – resignation to the negative situation: low (83.82% for group M; 82.48% for group P).
-
Rumination – continuous thoughts of emotions and ideas associated with the negative event: low (58.82% for group M; 58.39% for group P).
-
Positive refocus – thinking is intended to pleasant things and not to the negative situation: low (77.21% for group M; 77.37% for group P).
-
Refocus on planning – concentration on measures to be taken to confront the event: low (73.53% for group M; 75.18% for group P).
-
Positive reappraisal – attributing a positive significance to the negative situation, in the perspective of personal development: low (83.82% for group M; 82.48% for group P).
-
Putting into perspective – minimizing the seriousness of the event compared with other negative situations: low (69.12% for group M; 71.53% for group P).
-
Catastrophizing – emphasizing the degree of terror generated by the event: low (66.91% for group M; 67.88% for group P).
-
Culpability of others – guilt for bringing about the negative event is attributed to others: low (86.03% for group M; 74.45% for group P) – Table 3.
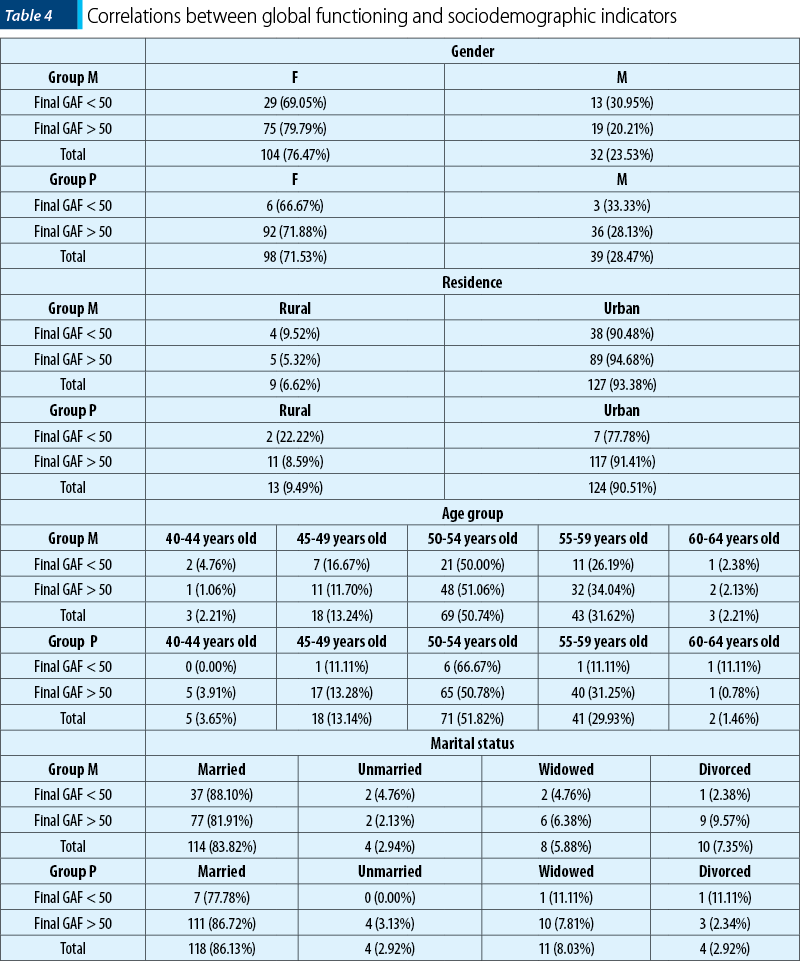
The extent of the impact on everyday life for the depressive patients included in the two groups evaluated with GAF scale provided an objective image on the level of functional and social adjustment of the subjects. Analyzing the correlation with the sociodemographic factors characteristic for the two groups, the global functioning was not significantly influenced by the subjects gender (group M: pχ2 = 0.173, p>0.05; group P: pχ2 = 0.738, p>0.05), place of residence (group M: pχ2 = 0.362, p>0.05; group P: pχ2 = 0.178, p>0.05), age of patients (group M: pχ2 = 0.571, p>0.05; group P: pχ2 = 0.089, p>0.05), or marital status (group M: pχ2 = 0.393, p>0.05; group P: pχ2 = 0.442, p>0.05) – Table 4.
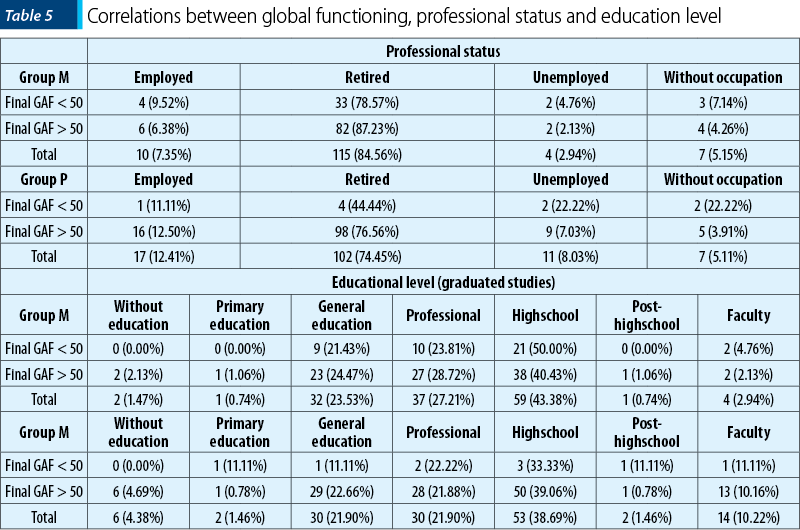
The global functioning deficit can result in the depreciation of the socioprofessional status of the affected person, a situation found in the subjects of our study, even though a significant correlation was underlined by the statistical calculation only in group P, which included patients receiving cognitive behavioral psychotherapy (group M: pχ2 = 0.614, p>0.05; group P: pχ2 = 0.027, p<0.05). Another significant contributor to the burden expressed by the level of global dysfunctionality was the educational level of the depressive patients that was significantly associated with the GAF scores also in the case of the second group studied (group M: pχ2 = 0.750, p>0.05; group P: pχ2 = 0.038, p<0.05) – Table 5.
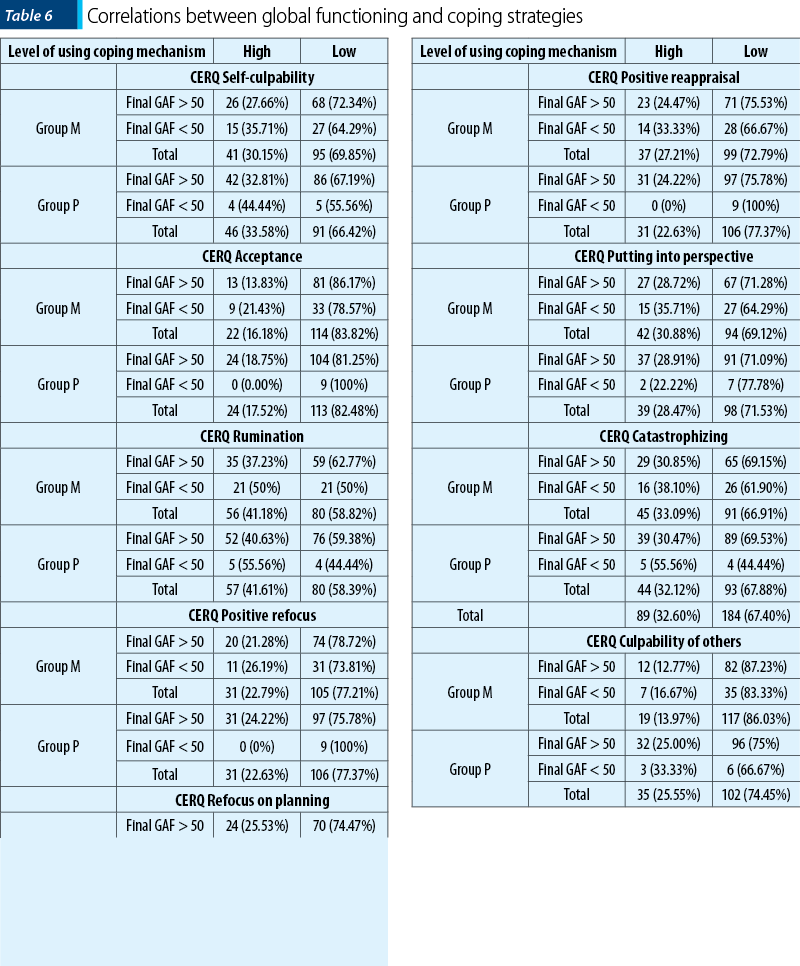
The role that individual coping strategies had on the patients’ functionality level was evaluated with the χ2 testing, respectively by calculating the Odds Ratio, in a comparative manner for both groups. Therefore, regarding self-culpability, we identified causal links in the subjects from group M, but no statistically significant associations (group M: pχ2 = 0.344, p>0.05; OR = 1.1; group P: pχ2 = 0.475, p>0.05; OR = 0.610).
Acceptance of the current situation or resignation to the negative situation represents one of the coping mechanisms with a strong impact on the personal skills regarding the descriptive elements of global functioning, thus representing a protective factor, determining the improvement of the functional level consequent to complex therapeutic intervention received by the subjects in group P (group M: pχ2 = 0.266, p>0.05; OR = 0.588; group P: pχ2 = 0.153, p>0.05; OR = 0). Rumination didn’t have a determining role in evaluating the influence of the global functioning either (group M: pχ2 = 0.162, p>0.05; OR = 0.593; group P: pχ2 = 0.380, p>0.05; OR = 0.547). Otherwise, the shift in attention and thinking towards pleasant situation and avoidance of the negative event led to a significant impact on regaining psychosocial abilities (group M: pχ2 = 0.528, p>0.05; OR = 0.762; group P: pχ2 = 0.093, p>0.05; OR = 0). Also, related to the assocition between coping mechanisms and good functionality, the statistical calculation revealed a strong causal link between the effects of combined therapy in group P and rethinking the measure to be taken to confront the negative life event (group M: pχ2 = 0.710, p>0.05; OR = 0.857; group P: pχ2 = 0.325, p>0.05; OR = 2.779), with a similar assessment for the influence of positive reappraisal (group M: pχ2 = 0.283, p>0.05; OR = 0.648; group P: pχ2 = 0.093, p>0.05; OR = 0). We did not observe the same level of association between the scores on GAF scales and the other two cognitive coping strategies, namely putting into perspective (group M: pχ2 = 0.415, p>0.05; OR = 0.725; group P: pχ2 = 0.668, p>0.05; OR = 1.423), and catastrophizing (group M: pχ2 = 0.407, p>0.05; OR = 0.725; group P: pχ2 = 0.119, p>0.05; OR = 0.351). The last evaluation scale for coping ways, culpability of others, also revealed a link with no statistical significance in both groups (group M: pχ2 = 0.544, p>0.05; OR = 0.732; group P: pχ2 = 0.580, p>0.05; OR = 0.667) – Table 6.
Discussion
It is well known that the major depressive disorder has a severe impact on the everyday life of the individual. In this respect, the comparative evaluation of the global functioning levels of the subjects in the two groups did not reveal significant differences between the groups at the admission moment, these being equally perceived as affecting the life of the patients, the majority (98.53% for group M, respectively 97.08% for group P) considering that the psychic disorder is severely debilitating their functioning abilities.
Upon final assessment, performed 12 weeks after starting the study, compared with the effects of the medication therapy, the analysis showed a net improvement (93.43% versus 69.12%, p<0.001) of the global functioning (psychological, social, occupational) of the patients receiving also psychotherapeutic intervention. We can advocate in this case that the results were not only due to the well-known efficacy of this technique as an interventional algorithm in the management of the depressive disorder(38), but rather due to the complex levels of its action, involving the biopsychosocial triangle so specific to the depressive disorder(39-42).
The depression requires the individual development of coping mechanisms contributing to the management of the disorder and the stress level, in close correlation with the psychological profile and the personality of the individual(43,44).
In the case of the two groups studied, the results from using CERQ lead to showing the most frequently used cognitive coping strategies by the subjects of the research, respectively rumination (41.39%), catastrophizing (32.60%), self-culpability (31.87%) and putting into perspective (29.67%). Thus, analyzing the frequency of use and the way each adjusting mechanism was reflected in the results of the therapeutic results, we were able to highlight the coping strategies that should be the target of the cognitive behavioral psychotherapy and, moreover, the consolidation of its results. In the context of rehabilitation of the psychosocial functionality of the depressive patients, we could underline an important role of the acceptance process, respectively of ruminative thinking, as intervention on these leads to positive effects in global functioning, as it was the case of the subjects using mainly putting into perspective as adjusting mechanism(41,45).
By correcting false beliefs about one's own person, which leads to maladaptive states and behaviors, the cognitive-behavioral therapy offers a viable therapeutic option in the approach of the depressive disorder, based on the principle that a thought precedes a state of mind and, in turn, these are correlated with the environment, physical and behavioral reaction of a person(46,47). In case of depressive, its efficiency is based both on the use of behavioral principles aimed at overcoming illness-induced inertia and on the consolidation of positive activities, as well as the opportunity for social networking, in a controlled environment that leads not only to improving the symptomatology, but also to regaining the social functioning(48).
Similar to the results of our research, numerous other studies and meta-analyses(49,50) demonstrate that cognitive-behavioral psychotherapeutic interventions are even more efficient than the medication therapy for the subjects with unipolar major depression, especially when referring to low to moderate forms of unipolar depression(51-53). Moreover, we can add the evidence suggesting that the relapse rate of the patients receiving cognitive-behavioral therapies is significantly lower compared with the one of individuals where the treatment was based only on pharmacotherapeutic methods(54,55).
Conclusions
Severe depression is significantly associated with psychosocial dysfunction, for the entire duration of the disorder, and the cognitive coping mechanisms used by the depressive patients represent elements with decisive influence on the onset moment, as well as on the quality of the therapeutic response. Consequently, a complex, multidisciplinary therapeutic management of this disorder is required, thus leading to a fast and complete recovery of the affected person, both from the clinical point of view and regarding the level of global functioning.
Bibliografie
Kessler RC. The costs of depression. Psychiatr Clin North Am. 2012;35:1-14.
World Health Organization. Depression and Other Common Mental Disorders Global Health Estimates. Geneva: World Health Organization, 2017.
GBD 2015 Disease and Injury Incidence and Prevalence Collaborators, and others. Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990-2015: a systematic analysis for the Global Burden of Disease Study 2015. The Lancet. 2016 Oct 8;388(10053):1545-1602.
Arias-de la Torre J, Vilagut G, Ronaldson A, Serrano-Blanco A, Martín V, Peters M, Valderas JM, Dregan A, Alonso J. Prevalence and variability of current depressive disorder in 27 European countries: a population-based study. Lancet Public Health. 2021;6(10). DOI:10.1016/S2468-2667(21)00047-5.
Kessler RC. The effects of stressful life events on depression. Annual Review of Psychology. 1997;48:191-214.
Hammen C. Stress and depression. Annual Review of Clinical Psychology. 2005;1:293-319.
Mazure CM. Life stressors as risk factors in depression. Clinical Psychology: Science and Practice. 1998;5:291–313.
Barrett AE, Turner RJ. Family structure and mental health: The mediating effects of socioeconomic status, family process, and social stress. Journal of Health and Social Behavior. 2005;46:156-169.
Muntaner C, Eaton WW, Miech R, O’Campo P. Socioeconomic position and major mental disorders. Epidemiologic Reviews. 2004;26:53-62.
Malik N, Boris N, Heller S, Harden B, Squires J, Chazan-Cohen R, Beeber LS, Kaczynski KJ. Risk for maternal depression and child aggression in Early Head Start families: A test of ecological models. Infant Mental Health Journal. 2007;28:171-191.
Gee GC, Spencer M, Chen J, Yip T, Takeuchi DT. The association between self-reported racial discrimination and 12-month DSM-IV mental disorders among Asian Americans nationwide. Social Science and Medicine. 2007;64:1984-1996.
Chin MH, Walters AE, Cook SC, Huang ES. Interventions to reduce racial and ethnic disparities in health care. Medical Care Research and Review. 2007;64:7S–28S.
Beck AT. Depression: Clinical, Experimental, and Theoretical Aspects. New York: Harper and Row, 1967.
Abramson LY, Metalsky GI, Alloy LB. Hopelessness depression: A theory-based subtype of depression. Psychological Review. 1989;96:358-372.
Joorman J. Cognitive aspects of depression. In: Gotlib I and Hammen C (Eds.), Handbook of Depression (2nd ed.), New York: Guilford Press, 2008, 298-321.
Hammen C, Brennan PA. Interpersonal dysfunction in depressed women: Impairments independent of depressive symptoms. Journal of Affective Disorders. 2002;72:145-156.
Eberhart NK, Hammen CL. Interpersonal predictors of stress generation. Pers Soc Psychol Bull. 2009;35(5):544-556.
Whisman MA, Bruce ML. Marital dissatisfaction and incidence of major depressive episode in a community sample. Journal of Abnormal Psychology. 1999;108:674-678.
Whisman MA. The association between depression and marital dissatisfaction. In: Beach SRH (Ed.), Marital and Family Processes in Depression: A Scientific Foundation for Clinical Practice. Washington, DC: American Psychological Association, 2001, 3-24.
Coryell W, Scheftner W, Keller M, Endicott J, Maser J, Klerman GL. The enduring psychosocial consequences of mania and depression. American Journal of Psychiatry. 1993;150:720-727.
Zlotnick C, Kohn R, Keitner G, Della Grotta SA. The relationship between quality of interpersonal relationships and major depressive disorder: Findings from the National Comorbidity Survey. Journal of Affective Disorders. 2000;59:205-215.
Whisman MA, Uebelacker LA, Weinstock LM. Psychopathology and marital satisfaction: The importance of evaluating both partners. Journal of Consulting and Clinical Psychology. 2004;72:830-838.
Coyne JC, Thompson R, Palmer SC. Marital quality, coping with conflict, marital complaints, and affection in couples with a depressed wife. Journal of Family Psychology. 2002;16:26-37.
Davila J, Karney BR, Hall TW, Bradbury TN. Depressive symptoms and marital satisfaction: Within-subject associations and the moderating effects of gender and neuroticism. Journal of Family Psychology. 2003;17:557-570.
Campbell JC. Health consequences of intimate partner violence. The Lancet. 2002;359:1331–1336.
O’Campo P, Ahmad F, Cyriac A. Chapter 12: Role of healthcare professionals in preventing and intervening on IPV. In Keeling J and Mason T (Eds.), Domestic Violence: A Multi-professional Approach for Health Professionals. Maidenhead, UK: Open University Press, 2008, 107-115.
Golding JM. Intimate partner violence as a risk factor for mental disorders: A metaanalysis. Journal of Family Violence. 1999;14:99-132.
Calvete E, Corral S, Estevez A. Cognitive and coping mechanisms in the interplay between intimate partner violence and depression. Anxiety, Stress and Coping. 2007;20:369-382.
Boris NW, Larrieu JA, Zeanah PD, Nagle GA, Steier A, McNeill P. The process and promise of mental health augmentation of nurse home-visiting programs: Data from the Louisiana Nurse-Family Partnership. Infant Mental Health Journal. 2006;27:26-40.
Bifulco A, Moran P, Ball C, Bernazzani O. Adult attachment style. I: Its relationship to clinical depression. Social Psychiatry and Psychiatric Epidemiology. 2002;37:50-59.
Mathews CA, Reus VI. Assortative mating in the affective disorders: A systematic review and meta-analysis. Comprehensive Psychiatry. 2001;42:257-262.
Hammen C, Brennan PA. Interpersonal dysfunction in depressed women: Impairments independent of depressive symptoms. Journal of Affective Disorders. 2002;72:145-156.
Burton E, Stice E, Seeley JR. A prospective test of the Stress-Buffering Model of Depression in adolescent girls: No support once again. Journal of Consulting and Clinical Psychology. 2004;72:689-697.
Dalgard OS, Dowrick C, Lehtinen V, Vazquez-Barquero JL, Casey P, Wilkinson G, Ayuso-Mateos JL, Page H, Dunn G, and the ODIN Group. Negative life events, social support and gender difference in depression. Social Psychiatry and Psychiatric Epidemiology. 2006;41: 444-451.
Tse WS, Bond AJ. The impact of depression on social skills. Journal of Nervous and Mental Disease. 2004;192:260-268.
Gladstone GL, Parker GB. Is behavioral inhibition a risk factor for depression? Journal of Affective Disorders. 2006;95:85-94.
Markowitz JC. Psychotherapy of the post-dysthymic patient. J Psychother Pract Res. 1993;2:157-163.
Bandura A. Social Learning Theory. Englewood Cliffs, NJ: Prentice-Hall, 1977.
Rehm LP. Behavior Therapy for Depression. New York: Academic Press, 1979.
Nezu AM. Efficacy of a social problem-solving therapy approach for unipolar depression. J Consult Clin Psychol. 1986;54:196-202.
Martell CR, Addis ME, Jacobson NS. Depression in Context: Strategies for Guided Action. New York: W.W. Norton, 2001.
Dunkel-Schetter CD, Feinstein LG, Taylor SE, Falke RL. Patterns of coping with cancer. Health Psychology. 1992;11:79-87.
Maddux JE. Stopping the “madness”: Positive psychology and the deconstruction of the illness ideology and the DSM, in Snyder CR, Lopez SJ (eds.) Handbook of positive psychology. New York: Oxford University Press, 2005.
Bellack AS, Hersen M, Himmelhoch JM. A comparison of social-skills training, pharmacotherapy and psychotherapy for depression. Behav Res Ther. 1983;21:101-107.
Beck AT. Cognitive therapy and the emotional disorders. New York: International Universities Press, 1976.
Greenberger D, Padesky CA. Mind over mood: a cognitive therapy treatment manual for clients. New York: Guilford Press, 1995.
Beck A, Rush A. Cognitive therapy. In: Kaplan H, Sadock B, et al (eds.) Comprehensive textbook of psychiatry. 6th ed. Baltimore: Williams & Wilkins, 1995, 1849-50.
Wampold BE, Minami T, Baskin TW, Callen Tierney S. A meta-(re)analysis of the effects of cognitive therapy versus ’other therapies’ for depression. J Affect Disord. 2002;68:159–65.
DeRubeis RJ, Gelfand LA, Tang TZ, Simons AD. Medications versus cognitive behavior therapy for severely depressed outpatients: meta-analysis of four randomized comparisons. Am J Psychiatry. 1999;156:1007–13.
Fennell M. Cognitive behaviour therapy for depressive disorders. In: Gelder M, Andreasen N, Lopez-Ibor J, Geddes J, editors. New Oxford Textbook of Psychiatry. New York: Oxford University Press, 2012, 1304-12.
Dobson KS. A meta-analysis of the efficacy of cognitive therapy for depression. J Consult Clin Psychol. 1989;57:414-9.
Robinson LA, Berman JS, Neimeyer RA. Psychotherapy for the treatment of depression. Psychol Bull. 1990;108:30–49.
American Psychiatric Association. Treatment of patients with major depressive disorder. American Psychiatric Association Practice Guidelines (3rd ed.), 2010.
Gautam M, Tripathi A, Deshmukh D, Gaur M. Cognitive Behavioral Therapy for Depression. Indian J Psychiatry. 2020;62(Suppl 2):S223-S229.
Articole din ediţiile anterioare
Modele de adaptare şi acceptare a schimbării la femeile din România. Resurse, limite şi consecinţe
Obiectivul principal al lucrării de faţă este prezentarea mecanismelor de coping folosite de femeile care se consideră afectate de criza economică ...