Vertebral hemangioma is one of the most frequent benign tumors of the spine. About 1% of these tumors become aggressive and symptomatic. The aggressive vertebral hemangiomas associated with pregnancy represent an extremely rare condition, and obstetricians should be aware of this pathology in case of subacute onset of motor deficit and paraplegia, especially during the third trimester. The association with pregnancy favors the rapid onset of neurological symptomatology and raises particular issues in terms of prompt diagnosis and treatment, with the aim to prevent both maternal and fetal morbidity. We report a rare case of aggressive thoracic hemangioma during pregnancy. The severe and rapidly progressive neurological deficit caused by the vertebral tumor required complex postpartum interventional and neurosurgical treatment.
Hemangiom vertebral agresiv care determină afectare neurologică severă în al treilea trimestru de sarcină – prezentare de caz
Aggressive vertebral hemangioma, causing severe neurological impairment in the third trimester of pregnancy – case presentation
First published: 30 septembrie 2020
Editorial Group: MEDICHUB MEDIA
DOI: 10.26416/Gine.29.3.2020.4059
Abstract
Rezumat
Hemangiomul vertebral reprezintă una dintre cele mai frecvente tumori benigne ale coloanei vertebrale. Aproximativ 1% dintre aceste tumori se dezvoltă agresiv şi devin simptomatice. Hemangioamele vertebrale agresive asociate cu sarcina reprezintă o afecţiune extrem de rară, iar obstetricienii trebuie să aibă în vedere o astfel de patologie în cazul gravidelor care prezintă deficit motor şi paraplegie debutate subacut, în special în al treilea trimestru de sarcină. Asocierea cu sarcina favorizează instalarea rapidă a simptomatologiei neurologice şi ridică probleme particulare în ceea ce priveşte diagnosticul şi tratamentul prompt, cu scopul de a preveni morbiditatea atât maternă, cât şi fetală. În această lucrare raportăm un caz rar de hemangiom agresiv toracic în timpul sarcinii. Deficitul neurologic rapid progresiv cauzat de tumora vertebrală a necesitat tratament complex post-partum, intervenţional şi neurochirurgical.
Introduction
Hemangiomas are benign vascular tumors characterized by endothelial cell proliferation, most commonly affecting the soft tissues, but they can also be identified in bones, including the vertebral body. These benign tumors of the spine affect 10-12% of the general population and the typical forms represent an incidental imagistic finding, as they are usually asymptomatic(1). About 1% of the vertebral hemangiomas are aggressive(2), a term used to define significant vertebral growth and even epidural extraosseous expansion leading to neurological deficits that require immediate treatment(3). This condition can occur at any age, with maximum prevalence in young women, while in terms of localization, it has been noticed a predilection for the thoracic vertebrae. The appearance of symptoms is more frequent in the 4th decade of life(4). The typical symptomatology includes back pain, subsequent acute or subacute progressive paraplegia and potential sensory deficit.
During pregnancy, the related hemodynamic and hormonal changes have a global effect of promoting the growth of an already existing vertebral hemangioma and can hasten the onset of symptoms. Accordingly, obstetricians should be aware of diagnosis and treatment particularities for this pathology, in order to minimize the maternofetal disability.
Case presentation
A 41-year-old Caucasian female was referred to our hospital from a county maternity in the 37th week of pregnancy for multidisciplinary investigations and therapeutic approach within the context of subacute paraparesis of unspecified etiology.
The patient was a multiparous with one previous caesarean section 14 years ago and an abortion in her obstetrical history, suffering from chronic hypertension efficiently controlled under 500 miligrams of methyldopa daily treatment, with no history of infections or other pathology in the current antenatal care. Her surgical history included appendicectomy and right inguinal hernia treated during childhood. She declared that the onset of the neurological symptoms dated one month ago in the form of paresthesia in the lower limbs, followed by progressive decrease in muscle strength, making ambulation impossible for the last week and associating urinary incontinence for the last three days.
At the time of the presentation in our hospital, the usual laboratory test and blood pressure were within normal limits. The obstetrical examination revealed the uterine height corresponding to the gestational age, normal uterine tone, a breech presentation, centered and short, undilated cervix, intact forewaters and no vaginal bleeding. The ultrasound confirmed the single pregnancy in complete breech presentation, biometrically corresponding to a 37-week pregnancy, with present fetal movements and fetal cardiac activity. The neurological consult suggested thoracic myelopathy, and cervicothoracal vertebro-medullary magnetic resonance imaging (MRI) was indicated.
The native MRI described multiple body vertebral hemangiomas of variable size affecting C2, C4, T10, T11, T12, L1, L2, L3 and L4 vertebrae and an aggressive hemangioma in the fourth thoracic vertebra. This aggresive T4 hemangioma was affecting the body and vertebral pedicles, with endocanal bulging of the posterior wall and occupation of paravertebral spaces (Figure 1). The lesion assembly was causing stenosis of conjugation holes and stenosis of the thoracic vertebral canal at T4-T5 (the remaining canal measuring 5 mm in anteroposterior and transverse diameters). In addition, MRI also identified small posteromedial T6 and T7 herniated discs that cleared the anterior epidural space without compression.

The multidisciplinary discussion among obstetricians, neurosurgeons and intensivists favored a caesarean section action before the decompressive intervention for the aggressive hemangioma.
The patient was admitted to our clinic and emergency segmental-transverse caesarean section was carried out under AG-IOT without intraoperative incidents. On the second day postpartum, the patient was transferred to the neurosurgery department.
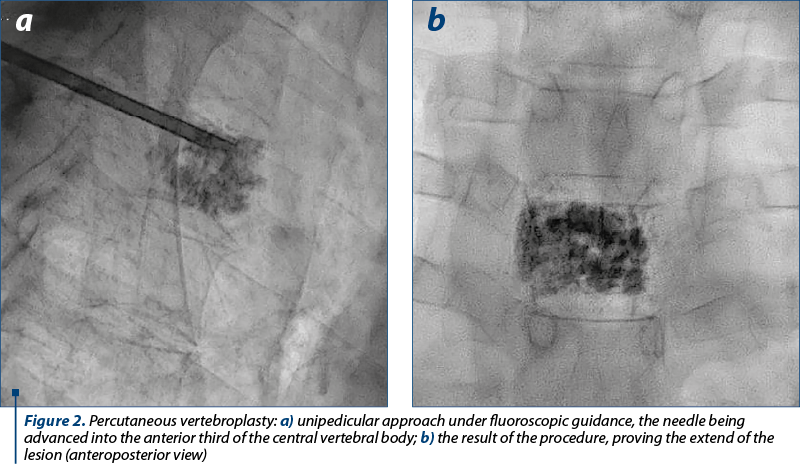
The neurological examination at the time of transfer identified symmetrical paraparesis (Frankel C grade), hypotonia, absent involuntary movements, subjective hypoaesthesia with T4 level, without pain charges, myoarthrokinetic sensitivity present and diminished dermoalgesic sensitivity, symmetrically diminished ROT, and bilateral positive Babinski. The first therapeutic procedure consisted of percutaneous vertebroplasty with acrylic cement. A transpedicular unilateral approach was used, reaching the center of the vertebral body T4 (Figure 2a). The cementoplasty efficiently stabilized the weakened T4 vertebra, without complications.
The neuroimagistic extension of the lesion and the significant myelopathy required a complementary decompressive surgery. Considering the endocanal bulging of the posterior wall and severe spinal and foraminal stenosis, neurosurgeons decided to perform laminectomy. The T4 and partially T5 laminae were removed, safely controlling the intraoperative bleeding, followed by epidural drain placement.
After 24 hours in the intensive care unit for monitoring and supporting vital functions, the patient returned to our clinic. Epidural drainage was safely suppressed and, for the next days, a slow favorable neurological evolution was observed, with visible motor total recovery for the right lower limb and weaker, partial recovery for the left lower limb. The evolution was burdened by a Clostridium difficile infection (positive GDH, negative toxins A and B), possibly in the context of previous hospitalization in another clinic, but the effective remission of symptoms was obtained under specific antibiotics.
During the sixth day of hospitalization, the patient requested the discharge contrary to medical advice. At the time of hospital discharge, the patient was in good condition, with supple surgical wounds, patent indwelling urinary catheter with normal diuresis and therapeutically controlled blood pressure values. Unfortunately, the patient was lost to neurological follow-up.
Discussion
Very few cases of aggressive vertebral hemangiomas associated with pregnancy are reported in the literature, the first case being mentioned in 1927(5,6).
The hemodynamic changes in the modified vessels cause an increase in previously existing vertebral hemangiomas. These changes appear due to venous obstruction, as the distended pregnant uterus increases the intraabdominal pressure and compresses the inferior vena cava. Consequent blood redistribution and increased blood flow through the vertebral venous plexus trigger structural changes in the vascular wall of the tumor vessels(7). In terms of hormonal changes related to pregnancy, maternal progesterone increases venous distensibility and reduces the response to vasoconstrictor stimuli, estrogen has a stimulating effect on endothelial growth, and relaxin has heterogeneous actions on different vascular beds, also modulating structural changes in the vascular wall. Along with the increased plasma volume, the vascular distensibility may help increase the size of a preexisting hemangioma, although the expression of estrogen and progesterone receptors in tumor tissue is still controversial among immunohistochemical analyses performed on vertebral hemangiomas(1,8).
The presented case fulfills some of the risk factors mentioned in literature, as the female sex and the 4th decade of life are associated with a higher incidence of symptomatic vertebral hemangiomas. The most frequent localization in the upper thoracic level(9) and the association with rapid onset of neurological symptoms in the third trimester(6) are also criteria fulfilled by the reported case. Although back pain is frequent, our patient presented pain symptoms only for a short while, and the motor deficit progressed rapidly within one month to paraparesis.
MRI is the imagistic diagnostic examination of choice in pregnancy. The differential diagnosis includes metastases and lymphoma. Preoperative imagistic diagnosis is essential to appreciate the local extension and the intraoperative bleeding risk(10). The neurological manifestations usually result from compression fracture of the vertebrae, acute hemorrhage in the extradural space, angiomatous invasions of laminae or cortex, spinal cord ischemia by “steal” mechanism, subperiosteal growth of the tumor etc. In this case, the subacute neurological impairment resulted from the extradural extension and compression of the spinal cord, given a high degree of stenosis of the thoracic spinal canal at T4-T5.
The conservative treatment may be efficient for mild symptoms, as spontaneous remission of symptomatology after birth is possible, but the aggressive vertebral hemangioma in pregnancy usually causes progressive neurological impairment. The therapeutic options include radiotherapy for slow progressive neurological deficiency, modern minimally invasive procedures like balloon kyphoplasty or transarterial embolization with associated laminectomy for smaller lesions or surgery in cases of rapidly progressive neurological symptoms, such as compressive myelopathy or radiculopathy(11). Pregnancy is a relative contraindication to radiation therapy. Endovascular embolization usually produces transient remission, but despite the risk related to exposure of the fetus to radiation during fluoroscopy, there are reported cases of successful embolization in pregnant women, followed by complete recovery. Percutaneous cementoplasty, also known as vertebral packing or vertebroplasty with acrylic cement, is a promising therapeutic technique for preventing vertebral body collapse and pain in patients with pathologic vertebral body(12). This relatively new treatment option may be contraindicated in patients with epidural hemangiomas, where careful injection of the cement is required in order to prevent epidural overflow and spinal cord compression by the cement or displaced epidural tissue(13). The anterior corpectomy is potentially curative, but the risk of intraoperative bleeding during this maneuver is substantial. Laminectomy may allow appropriate emergency decompression in selected cases, especially in those with epidural tumors or laminar involvement, but the recurrence of symptoms is common, eventually requiring definitive treatment.
The timing of surgery in cases diagnosed antepartum is controversial. The duration of pregnancy and the status of neurological deficits are useful in planning treatment(14). An expectant conservative approach is attempted whenever the location of the tumor in the vertebrae does not cause rapidly worsening myelopathy or radiculopathy. Earlier than 32 weeks of gestation, antepartum procedure is reserved for severe cases of paraplegia. Cases of premature birth and postoperative fetal death inclusively have been reported in antepartum surgery. After 32 weeks of gestation, if neurological function deteriorates, caesarean section can be considered, followed by the appropriate management of the spinal tumor(2).
In the reported case, multiple body vertebral hemangiomas with variable dimensions were found along cervical, thoracic and lumbar vertebrae. The patient was asymptomatic previous to the third trimester, inclusively during her first pregnancy. The extension of the T4 aggressive vertebral hemangioma and the severity of symptoms imposed emergency caesarean section to allow advanced postpartum neurosurgical treatment. The patient presented in our service at 37 weeks of gestation and the fetus was safely delivered, without any negative fetal impact from the maternal neurological impairment. The vertebroplasty aimed to stabilize the vertebral body, preventing a compression fracture, since the tumor affected more than half of the vertebral body. Given the stenosis of the thoracic spinal canal, laminectomy was decided as a complementary palliative therapy. Despite the favorable postoperative neurological evolution, symptoms may recur at a variable distance from the intervention, since the curative treatment was not possible, thus the neurological long-term follow-up is important.
Conclusions
Quiescent vertebral hemangioma can grow aggressively in pregnancy, becoming symptomatic more often in the third trimester. Aggressive vertebral hemangiomas causing rapidly progressive neurological deficit in pregnancy are extremely rare. The reported case is particular due to the presence of multiple vertebral hemangiomas and the extension of the upper thoracic lesion. The severe and rapidly progressive symptomatology required immediate decompressive intervention. Complex neurosurgical treatment was performed after delivery, achieving satisfactory recovery. Since such cases are extremely rare, the management of symptomatic vertebral hemangiomas must be tailored depending on the week of gestation and the clinical severity.
Bibliografie
-
Slimani O, Jayi S, Alaoui FF, Bouguern H, Chaara H, Fikri G, Rachidi SA, Sqalli Houssaini N, Himmich M, Melhouf MA. An aggressive vertebral hemangioma in pregnancy: A case report. J Med Case Rep. 2014;8:207.
-
Chi JH, Manley GT, Chou D. Pregnancy-related vertebral hemangioma. Case report, review of the literature, and management algorithm. Neurosurg Focus. 2005;19(3):E7.
-
Fox MW, Onofrio BM. The natural history and management of symptomatic and asymptomatic vertebral hemangiomas. J Neurosurg. 1993;78(1):36-45.
-
Slon V, Stein D, Cohen H, Sella-Tunis T, May H, Hershkovitz I. Vertebral hemangiomas: their demographical characteristics, location along the spine and position within the vertebral body. Eur Spine J. 2015;24(10):2189-95.
-
Fields WS, Jones JR. Spinal epidural in hemangioma in pregnancy. Neurology. 1957;7(12):825-8.
-
Wang B, Jiang L, Wei F, Liu XG, Liu ZJ. Progression of aggressive vertebral hemangiomas during pregnancy. Medicine (Baltimore). 2018;97(40):e12724.
-
Nelson DA. Spinal cord compression due to vertebral angiomas during pregnancy. Arch Neurol. 1964;11(4):408-13.
-
Schwartz TH, Hibshoosh H, Riedel CJ. Estrogen and progesterone receptor-negative T11 vertebral hemangioma presenting as a postpartum compression fracture: case report and management. Neurosurgery. 2000;46(1):218-21.
-
Lavi E, Jamieson DG, Granat M. Epidural haemangiomas during pregnancy.
-
J Neurol Neurosurg Psychiatry. 1986;49(6):709-12.
-
Meng T, Yin H, Li Z, Li B, Zhou W, Wang J, Zhou L, Song D, Xiao J. Therapeutic strategy and outcome of spine tumors in pregnancy: A report of 21 cases and literature review. Spine (Phila Pa 1976). 2015;40(3):E146-53.
-
Moles A, Hamel O, Perret C, Bord E, Robert R, Buffenoir K. Symptomatic vertebral hemangiomas during pregnancy. J Neurosurg Spine. 2014;20(5):585-91.
-
Galibert P, Déramond H. Percutaneous acrylic vertebroplasty as a treatment of vertebral angioma as well as painful and debilitating diseases. Chirurgie. 1990;116(3):326-34.
-
Inamasu J, Nichols TA, Guiot BH. Vertebral hemangioma symptomatic during pregnancy treated by posterior decompression, intraoperative vertebroplasty, and segmental fixation. J Spinal Disord Tech. 2006;19(6):451–4.
-
Liu S, Wang Y, Yang X, Lei B, Liu L, Li SX, Ni D, Wang T. Deep learning in medical ultrasound analysis: a review. Engineering. 2019;5(2):261–75.
Articole din ediţiile anterioare
Complicaţii materne şi neonatale în sarcina gemelară obţinută spontan versus sarcina gemelară obţinută prin FIV
Acest studiu a avut ca obiectiv identificarea complicaţiilor materne şi neonatale din sarcina gemelară obţinută spontan, comparativ cu sarcina gem...
Efectele vitaminei D în sarcină
Naşterea, creşterea, dezvoltarea, reproducerea şi îmbătrânirea în condiţii fiziologice pot fi realizate fără a diminua rolul celorlalte aspecte ...
Implicaţii şi consecinţe ale sarcinii la adolescente
Context. Numărul sarcinilor în rândul adolescentelor este în continuă creştere la nivel global, ca urmare a schimbărilor sociale şi libertăţii sexu...
O singură inimă nu e de ajuns – gemeni conjuncţi: diagnosticul prenatal şi evaluarea malformaţiilor asociate. Prezentare de caz
Incidenţa sarcinilor multiple a crescut de-a lungul timpului datorită îmbunătăţirii tehnicilor de reproducere asistată şi reprezintă de obice...