In the last decades, the screening for Down syndrome brought the 11- to 14-week scan to the forefront of modern pregnancy care. Initially just a nuchal scan as part of the combined test, it upgraded to a detailed anatomy scan that should be done always where the ultrasound machine and the expertise allow, as instructed by current guidelines. Though a lot of the anatomy can be assessed at this age, it is still mainly used only for the measurements necessary for the combined tests or for noninvasive prenatal testing, hence a lot of the structural anomalies are missed. Our paper focuses on cases in which the anatomy scan was not performed, and structural and chromosomal anomalies were missed.
OBSTRETICS
Importanţa evaluării anatomiei fetale la screeningul de 11-14 săptămâni
The importance of anatomy scan at the 11-14-week screening
First published: 30 noiembrie 2022
Editorial Group: MEDICHUB MEDIA
DOI: 10.26416/Gine.38.4.2022.7379
Abstract
Rezumat
În ultimi anii, screeningul pentru sindromul Down a adus ecografia de 11-14 săptămâni în centrul atenţiei îngrijirii prenatale moderne. Iniţial destinată doar măsurării translucenţei nucale ca parte a testului combinat, a evoluat către o evaluare detaliată a anatomiei fetale care trebuie efectuată, în limitele rezoluţiei aparatului şi ale experienţei examinatorului, cât mai aproape de recomandările ghidurilor de bună practică. Deşi o bună parte din anatomie poate fi evaluată la această vârstă de sarcină, este în continuare frecventă doar efectuarea măsurătorilor strict necesare pentru testul combinat sau pentru testarea neinvazivă (NIPT), ratând astfel diagnosticul unor anomalii structurale. Această lucrare se concentrează pe consecinţele evaluării ecografice de 11-14 săptămâni la care nu a fost efectuată evaluarea anatomiei, iar unele anomalii structurale şi cromozomiale au scăpat diagnosticului.
In the last decades, the 11-14-week ultrasound scan has become a routine, offering the best compromise between early detection and the amount of information offered, hence its importance in screening. Though initially only a part of the Down screening protocol, it has increased in importance, with the improvement of ultrasound machine, becoming the first anomaly scan.
The 11- to 14-week scan should reveal information regarding:
-
the confirmation of the gestational age;
-
chromosomal anomaly screening (together with PAPP-A and beta-HCG);
-
a detailed anatomy scan (as detailed as the sonographer and the machine can provide);
-
evaluation of the uterine arteries, which has become a promising marker for preeclampsia.
Other information (location, viability) is already established at an earlier gestational age.
The early anatomy scan at the 11-14-week scan provides the diagnosis of major fetal anomalies and access to termination of pregnancy (TOP) at a smaller gestational age or access to invasive maneuvers earlier in pregnancy than if we only relied on the 19-23-week scan(1,2). Most organs and systems are partially accessible (some more than others) at the 11-14-week ultrasound scan, with some difference between the 11-12-week scan and the 13-14-week scan. A normal result of the early anatomy scan will reduce the couple’s anxiety, especially if there has been a previous unsuccessful pregnancy. The amount of information obtained depends mainly on the experience of the examiner, but it is also dependent on the protocol you are using – one will only see what he is looking for. We will discuss what guides advise us to look for at the present time (they are always subject to updating) and what can reasonably be seen at 11-14 weeks.
The examination should try to get as much information as possible regarding(3,4):
-
The fetal head – the falx cerebri, the butterfly image of the choroid plexus, integrity of the skull; the examiner should always try to get a normal image of the falx and the choroid plexus, as failure to obtain it may lead to missing one of the most important diagnoses in the first trimester scan, holoprosencephaly.
-
The face – orbits, lens, fetal profile with the nasal bone; careful consideration should be given to the lens, as congenital cataract can easily be missed for a transabdominal scan if there is poor resolution.
-
The spine – correct alignment of the vertebrae with intact overlying skin.
-
The neck – the sonographer should be able to detect cystic hygroma and do a correct measurement of the nuchal translucency (this measurement is standardized and the recommendations of the Fetal Medicine Foundation should be respected).
-
The heart – the examiner should see the heart on the left and a normal cardiac axis with a regular cardiac activity and should also try to obtain a four-chamber view, sometimes more difficult especially with transabdominal ultrasound. A more efficient screening can be done with the help of color Doppler, showing normal atrioventricular flow and normal three-vessel view.
-
The abdomen and the abdominal wall – the stomach on the left, the kidneys, the bladder and the cord insertion. The stomach should always be seen after 12 weeks and the bladder should be seen 80% of the time after 12 weeks and 90% of the time after 13 weeks. In our opinion, the stomach and the bladder can always be seen in normal circumstances, but it may require reexamining the patient after 30 minutes. The evaluation of the fetal bladder should be accompanied by Doppler confirmation of the umbilical arteries.
-
The extremities – four limbs with three segments each should be demonstrated, either on separate images or short clips.
-
Sometimes, the sex of the baby can be determined, though it is not included or recommended in any guide.
-
Placenta and the umbilical cord. The location of the placenta(5) should be mentioned, along with size and texture. The umbilical cord should have three vessels, and any cysts or other anomalies should be noticed and mentioned.
At this time, there are four standard images at the 11-14-week scan:
-
CRL (crown rump length).
-
Nuchal translucency.
-
Situs solitus (heart on the same side with the stomach).
-
The symmetry of the cerebral structures (the butterfly image of the choroid plexus).
Noninvasive prenatal screening (NIPT)
The analysis of the fetal free DNA in the maternal blood may detect 99% of Down syndrome cases, 97% of trisomy 18 cases and 92% of trisomy 13 cases, with a false positive ratio of 0.1%, 0.2% and 0.2%, respectively. The results should be carefully interpreted as the aforementioned values are for an ideal quantity of fetal free DNA.
For a good cost detection rate and cost-efficient ratio (for the health systems), probably the most efficient way would be a two-step system:
-
first line – the combined test;
-
patients above a certain cut-off should receive NIPT.
There are current studies that show good detection rate, lowering of the numbers of invasive procedures and good acceptance among pregnant women.
What is currently done at 11-14 weeks?
Probably, more than 50% (there are no randomized studies on this subject(6,7)) receive a basic model of combined test consisting of measurement of the CRL and the nuchal translucency together with the results of beta-HCG and PAPP-A. A small percentage of pregnant women will have an NIPT (which needs just measurement of the CRL).
A complete evaluation of the fetal anatomy or as much as reasonably achievable at 11-14 weeks should always be performed, as we are frequently confronted with major malformations that can be detected at 11-14 weeks and sometimes with anomalies that suggest false negative results of the combined test or even of NIPT.
We present a few cases of patients who presented for anatomy scan after a normal combined test or NIPT or for a second combined test (after a previous combined test that did not meet their expectations).
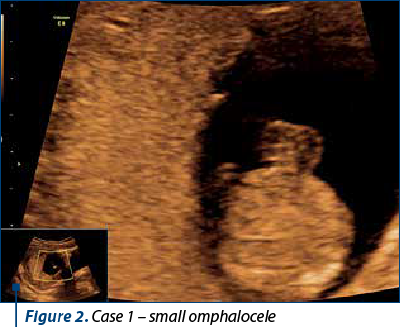
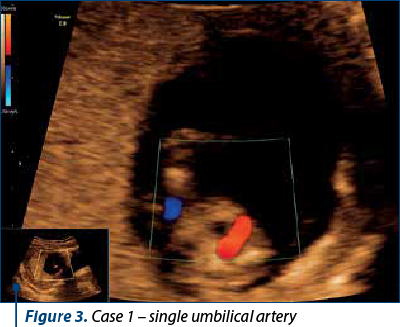
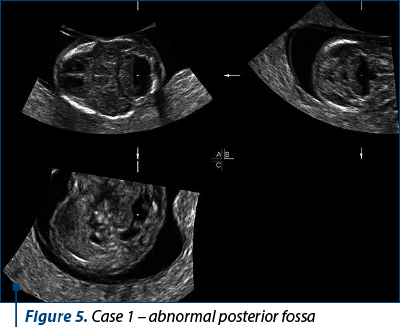
Case 1
A 28-year-old patient presented for anatomy scan at 13 weeks + 4 days. She had a normal NIPT at approximately 11 weeks, with a borderline free fetal DNA value.
The ultrasound scan revealed polydactyly, a small omphalocele and single umbilical artery, bilateral pyelectasis, and an abnormal image of the posterior fossa. The patient decided to have chorionic villus sampling – the result was trisomy 18.


Case 2
A 35-year-old patient had an NIPT at 10 weeks + 0 days. The results came back negative, but she decided to have an anatomy scan at 12-13 weeks. The ultrasound scan demonstrated the presence of an omphalocele – CVS revealed trisomy 18.

Case 3
A patient presented for anomaly scan at 12 weeks + 6 days. NIPT was performed at 10 weeks (the results are pending). The scan revealed multiple skeletal anomalies, a large nuchal translucency and retrognathia. The patient opted for TOP.





Case 4
A 32-year-old patient had an inconclusive result at NIPT. She was rescheduled for another test, but presented for anomaly scan and combined test just in case the next NIPT fails as well. The examination revealed holoprosencephaly.

Case 5
A 26-year-old patient had a combined test that showed a low risk (1 in 10,000), but she decided to have an early anatomy scan after discussing with friends about what information they received at their 11-14-week ultrasound. We diagnosed amniotic band syndrome with limb amputation.


Case 6
A 26-year-old patient, without prior risk, had a negative combined test at 12 weeks – she presented for anatomy scan at 18 weeks. The scan detected an open spina bifida. Though spina bifida is not always detected at the 11-14-week scan, sometimes an abnormal intracranial translucency (IT) or an abnormal image of the choroid plexus can lead to the diagnosis(8).

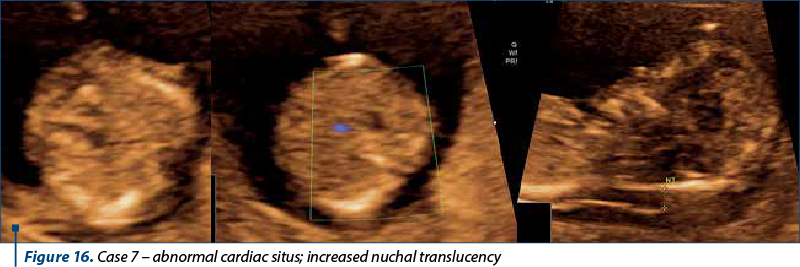
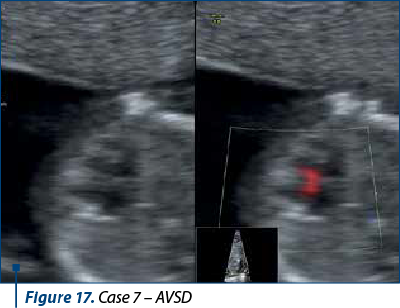
Case 7
A 30-year-old patient presented for anatomy scan and NIPT. The examination revealed an abnormal situs (the stomach was on the left, but the heart was on the right), increased nuchal translucency, and an atrioventricular septal defect. She decided for TOP, and the post-abortum karyotype confirmed our suspicion of Down syndrome.
Conclusions
A detailed anatomy scan should always be a part of the 11-14-week scan, and respecting the guidelines should be a target of our examination.
Conflict of interests: The authors declare no conflict of interests.
Bibliografie
-
Chaoui R, Nicolaides KH. From nuchal translucency to intracranial translucency: towards the early detection of spina bifida. Ultrasound Obstet Gynecol. 2010;35(2):133–8.
-
Efrat Z, Perri T, Ramati E, Tugendreich D, Meizner I. Fetal gender assignment by first- trimester ultrasound. Ultrasound Obstet Gynecol. 2006;27(6):619–21.
-
Ghidul privind examinarea ecografică de screening pentru anomalii de sarcină în trimestrul I, din 09.08.2019. Monitorul Oficial. Partea I, nr. 738bis, 10 septembrie 2019. Available at: https://sogr.ro/wp-content/uploads/2019/11/22.1.-Ghid-de-examinare-ecografică-de-screening-pentru-anomalii-de-sarcină-în-trimestrul-1.docx.pdf.
-
ISUOG Practice Guideline: performance of first trimester fetal ultrasound scan. Ultrasound Obstet Gynecol. 2013;41(1):102-13.
-
Michailidis GD, Papageorgiou P, Economides DL. Assessment of fetal anatomy in the first trimester using two- and three-dimensional ultrasound. Br J Radiol. 2002;75(891):215–9.
-
Nicolaides KH, Wright D, Poon LC, Syngelaki A, Gil MM. First‐trimester contingent screening for trisomy 21 by biomarkers and maternal blood cell‐free DNA testing. Ultrasound Obstet Gynecol. 2013;42(1):41-50.
-
Sánchez-Durán MÁ, Bernabeu García A, Calero I., et al. Clinical application of a contingent screening strategy for trisomies with cell-free DNA: a pilot study. BMC Pregnancy Childbirth. 2019;19(1):274.
-
Timor-Tritsch IE, Bashiri A, Monteagudo A, Arslan AA. Qualified and trained sonographers in the US can perform early fetal anatomy scans between 11 and 14 weeks. Am J Obstet Gynecol. 2004;191(4):1247–52.