We have conducted this observational retrospective study with the aim to see how different causes of infertility and associated pathologies influence the pregnancy rate in poor responder patients, according to Poseidon criteria. We included 332 women who met the POSEIDON criteria and underwent 438 controlled ovarian stimulation protocols and compared the cumulative pregnancy rate according to associated pathologies. We identified that 53% of the patients had dysmenorrhea, 36.4% had tubal pathology, 12.3% had a history of ovarian surgery, 13.6% had endometriosis, 4.8% had autoimmune thyroiditis, 8.4% had thrombophilia, 5.1% had uterine leiomyoma, and 18.7% had submucous leiomyoma, endometrial polyps or uterine synechia. In 47.7% of the couples, we identified a male infertility factor. The biochemical pregnancy rate was 33.6% and the clinical pregnancy rate was 26.9%. Life birth rate was 18.5%. We compared the pregnancy rate in all 332 patients and observed that no pathology had a significant influence on cumulative pregnancy rate (p>0.05). We also compared the pregnancy rate according to POSEIDON groups and we observed that no pathology had a significant influence on cumulative pregnancy rate (p>0.05), except for POSEIDON 1B group, where endometriosis had a negative effect on cumulative pregnancy rate (37.5% versus 84.8%; p=0.013). When comparing the cumulative pregnancy rate according to age and AMH (antimüllerian hormone), we observed that patients with an AMH≥1.2 ng/ml and maternal age below 35 years old had a significant higher pregnancy rate than patients with AMH<1.2 ng/ml (45.4% versus 25.8%) and maternal age ≥35 years old (49.1% versus 29.7%; p<0.001). We can conclude that age and AMH are the main influencing factors of cumulative pregnancy rate in poor responder patients. The associated pathology has a low or no impact on pregnancy rate in poor responder patients.
Cum influenţează patologia rata cumulativă de sarcini la pacientele cu răspuns ovarian scăzut?
How does pathology influence cumulative pregnancy rate in poor responder patients?
First published: 16 aprilie 2021
Editorial Group: MEDICHUB MEDIA
DOI: 10.26416/ObsGin.69.1.2021.4805
Abstract
Rezumat
Am efectuat acest studiu retrospectiv observaţional cu scopul de a vedea cum este influenţată rata de sarcini la pacientele cu răspuns ovarian scăzut (ROS), grupate conform criteriilor POSEIDON, în funcţie de patologiile asociate. Am inclus 332 de femei care au îndeplinit criteriile POSEIDON şi care au efectuat 438 de protocoale de stimulare ovariană controlată. La aceste paciente, am comparat rata cumulată de sarcină (RCS) în funcţie de patologiile asociate. Am observat că 53% dintre paciente au avut dismenoree, 36,4% au avut patologie tubară, 12,3% au avut antecedente de chirurgie ovariană, 13,6% au avut endometrioză, 4,8% au avut tiroidită autoimună, 8,4% au avut trombofilie, 5,1% au avut leiomiom uterin, iar 18,7% au avut leiomiom submucos, polip endocavitar sau sinechie uterină. Rata sarcinilor biochimice a fost de 33,6%, iar rata de sarcini clinice a fost de 26,9%. Rata de naşteri vii a fost de 18,5%. Am comparat rata de sarcină la toate cele 332 de paciente şi am observat că nicio patologie nu are o influenţă semnificativă asupra RCS (p>0,05). De asemenea, am comparat rata sarcinii în funcţie de grupurile cu POSEIDON şi am observat că nicio patologie nu a avut nicio influenţă semnificativă asupra RCS (p>0,05), cu excepţia grupului POSEIDON 1B, unde endometrioza a avut un efect negativ asupra RCS (p=0,013). Când am comparat RCS în funcţie de vârstă şi AMH (hormon antimüllerian), am observat că pacientele cu AMH ≥1,2 ng/ml şi cu vârsta sub 35 de ani au avut un RCS semnificativ mai mare decât pacientele cu AMH<1,2 ng/ml (45,4% versus 25,8%) şi vârsta maternă ≥35 ani (49,1% versus 29,7%; p<0,001). Putem concluziona că vârsta şi AMH sunt principalii factori care influenţează RCS la pacientele cu ROS. Patologia asociată are un impact redus sau niciun impact asupra RCS la pacientele cu ROS.
Introduction
1. Working hypothesis
We conducted this study to evaluate how does the associated pathology, AMH (antimüllerian hormone) and age infleunce pregnancy rate in poor responder POSEIDON groups following controlled ovarian stimulation.
2. Relevance of the topic of the paper
In human reproductive technology field, one of the main concerns of the infertility specialists is represented by patients with low ovarian response following exogenous stimulation with gonadotropins (poor responders). Risk factors for poor responders include age and low ovarian reserve. It is generally accepted that poor ovarian response is the consequence of a low ovarian reserve (AMH<1.2 ng/ml) and advanced maternal age (above 35 years old). Also, ovarian stimulation can be seen as a dynamic test for ovarian follicles(1-7).
POSEIDON groups represent the newest way to stratify poor responder patients according to some important quality and quantity parameters, such as: age and aneuploidy rate, AMH and antral follicle count (AFC), previous response to a controlled ovarian stimulation(8).
The variable that POSEIDON groups do not take into consideration is the associated pathology. That’s why we searched the answer to the following question, which is the subject of the current paper: How does pathology influence pregnancy rate in poor responder POSEIDON patients?
3. Objectives
The evaluation by statistical analysis of the influence of associated pathology on cumulative pregnancy rate in poor responder patients, according to POSEIDON criteria, age and AMH.
Materials and method
Study design
We performed a retrospective, observational, non-randomized study on all the women who underwent controlled ovarian stimulation and achieved ≤9 oocytes following oocyte pick-up in the Department of Assisted Human Reproduction of the “Prof. Dr. Panait Sîrbu” Clinical Hospital of Obstetrics and Gynecology, Bucharest, between January 2018 and December 2019. We grouped the patients according to age (<35/≥35) and AMH (<1.2/≥1.2 ng/ml) and according to POSEIDON criteria, as following.
POSEIDON group 1A: patients <35 years old, AMH≥1.2 ng/ml and <4 oocytes after controlled ovarian stimulation.
POSEIDON group 1B: patients <35 years old, AMH≥1.2 ng/ml and 4-9 oocytes after controlled ovarian stimulation.
POSEIDON group 2A: patients ≥35 years old, AMH≥1.2 ng/ml and <4 oocytes after controlled ovarian stimulation.
POSEIDON group 2B: patients ≥35 years old, AMH≥1.2 ng/ml and 4-9 oocytes after controlled ovarian stimulation.
POSEIDON group 3: patients <35 years old, AMH<1.2 ng/ml.
POSEIDON group 4: patients ≥35 years old, AMH<1.2 ng/ml.
Criteria for inclusion: patients undergoing assisted human reproduction (IVF/ICSI) treatments in the “Prof. Dr. Panait Sîrbu” Clinical Hospital of Obstetrics and Gynecology and who achieved ≤9 oocytes following oocyte pick-up. Exclusion criteria: record missing information.
In this study, data from 332 female patients on whom a total of 438 stimulation cycles and oocyte pick-ups were collected from patients records. The statistical analysis was performed using IBM SPSS Statistics 25 and Microsoft Office Excel/Word 2013. The quantitative variables were tested for distribution using the Shapiro-Wilk test and were expressed as means with standard deviations or medians with interpercentile intervals. The categorical variables were expressed in absolute or percentage form and were tested using Fisher’s Exact Test/Pearson Chi-Square Test.
Analyzed variables
To perform the analysis of the patients who participated in our study, the success has been quantified per patient, in all controlled ovarian stimulation protocols that one patient performed, by biochemical pregnancy rate (obtaining a positive b-hCG result), clinical pregnancy rate (ultrasonoghaphic confirmation of the pregnancy) and life birth rate (alive born baby) in all fresh and frozen embryotransfers (cumulative pregnancy rate).
Results
Characteristics of the studied group
The study was performed on 332 female patients, but the total number of cases investigated was 438. The average age was 37.14 ± 4.427 years old, with a median of 38 years old, the interval being between 24 and 47 years old. The mean value of AMH was 1.65 ± 2.66 ng/ml, with a median of 1.18 ng/ml, the interval being between 0.04 and 37.97 ng/ml. Most patients were classified in group 4 POSEIDON (39.8%) or group 2B (25.9%). Regarding the observed diagnostics, 53% of patients had dysmenorrhea (the most common pathology), 36.4% had tubal pathology, 12.3% had a history of ovarian surgery, 13.6% had endometriosis, 4.8% had autoimmune thyroiditis, 8.4% had thrombophilia, 5.1% had uterine leiomyoma, and 18.7% had submucosal fibroids/polyps/synechiae. In 47.7% of cases, the association of a male pathology was observed as an indicator of sterility. Regarding the stimulation protocol used, in 68.5% of the cases the GnRH antagonist short protocol was used (most frequently observed), 11.2% followed the GnRH agonist long protocol, 2.5% – the luteal phase ovarian stimulation protocol, 9.4% – the mild stimulation protocol, and 8.4% – natural cycle. In relation to the administered treatment, it was observed that 41.6% had follitropin alpha, 81.5% menotropin, 17.1% follitropin beta, 12.3% corifollitropin alpha, 7.3% follitropin delta, 8.9% letrozol, 3.9% clomiphene citrate, 0.9% folitropin alpha/lutropin alpha (for ovarian stimulation), 63.7% cetrorelix, 10.7% ganirelix, 11.4% triptoreline (for LH surge inhibition), 96.4% choriogonadotropin alpha and 25.1% had triptoreline (for LH surge induction). The mean value of the number of oocytes collected was 3.89 ± 2.751, with a median of 4 oocytes collected. The mean value of the number of mature oocytes was 3.03 ± 2.327, with a median of 3 mature oocytes. The mean value of the number of embryos was 2.38 ± 2.02, with a median of 2 embryos. The mean value of the number of embryos transferred fresh was 0.92 ± 0.881, with a median of 1 embryo. In relation to the embryo transfers protocols, it was observed that the most common procedures were performed in hormone replacement therapy (40.6% first embryo transfer/39.5% second embryo transfer/40% third embryo transfer) or natural cycle (39.1% first embryo transfer/44.7% second embryo transfer/40% third embryo transfer). Pregnancy was obtained in 34.5% of cases, more frequently following fresh embryo transfer (64.2%). Biochemical pregnancy was obtained in 33.6% of cases and clinical pregnancy in 26.9% of cases. In 18.5% of cases, live births were registered.
Comparison of the pregnancy rate in the whole group and in POSEIDON groups according to the frequency of the investigated pathologies (Table 1)
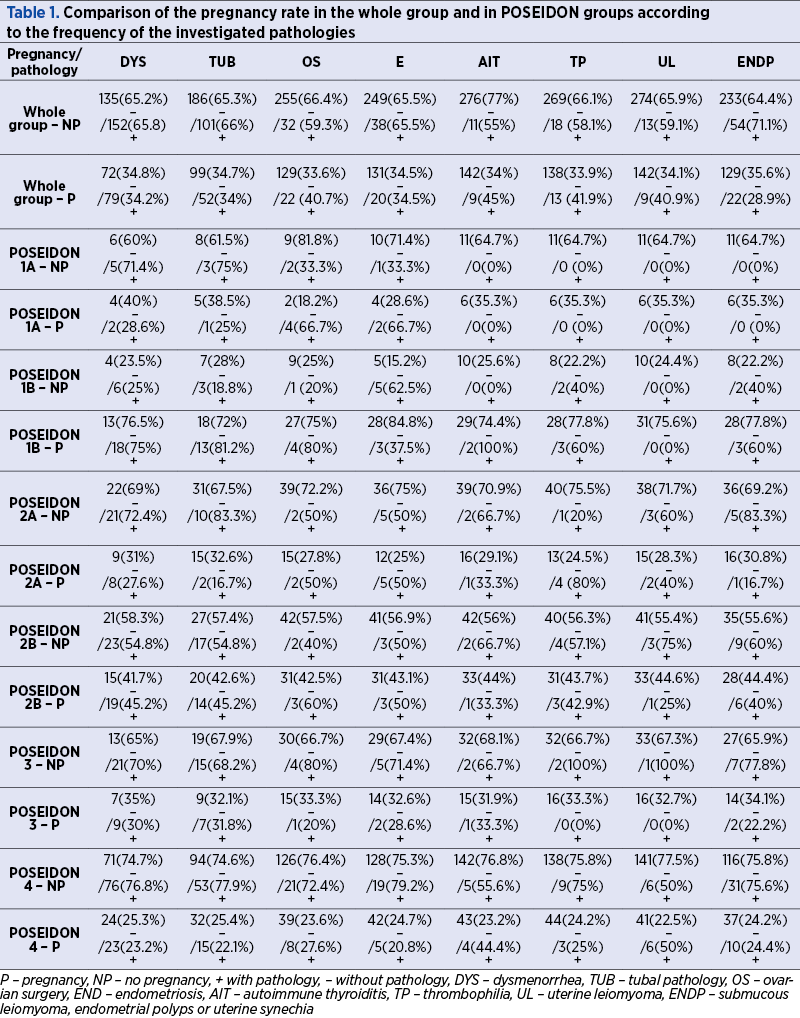
It is observed that in the POSEIDON 1A group, there is no pathology that has a significant effect of changing the cumulative pregnancy rate (p>0.05). It is observed that in the POSEIDON 1B group, there is no pathology that has a significant effect of changing the cumulative pregnancy rate (p>0.05), except for endometriosis, where a significantly lower cumulative pregnancy rate is observed in cases in which there was endometriosis (37.5% versus 84.8%; p=0.013). It is observed that in the POSEIDON 2A group, there is no pathology that has a significant effect of changing the cumulative pregnancy rate (p>0.05), except for thrombophilia, where a significantly higher cumulative pregnancy rate is observed in cases in which there was thrombophilia (80% versus 24.5%; p=0.023). It is observed that in the POSEIDON 2B group, there is no pathology that has a significant effect of changing the cumulative pregnancy rate (p>0.05). It is observed that in the POSEIDON 3 group, there is no pathology that has a significant effect of changing the cumulative pregnancy rate (p>0.05). It is observed that in the POSEIDON 4 group, there is no pathology that has a significant effect of changing the cumulative pregnancy rate (p>0.05), except for uterine leiomyoma where a significantly higher cumulative pregnancy rate was observed among cases in which the uterine leiomyoma was present (50% versus 22.5%; p=0.031) – Table 1.
Discussion
This retrospective observational study evaluated how the associated pathology influenced the cumulative pregnancy rate (fresh and frozen embryo transfers) in poor responder patients according to the POSEIDON criteria.
Our study reveals that there is no pathology that has a significant effect of changing the cumulative pregnancy rate in this low-prognosis patients. The only variables that change pregnancy rate with statistically significance are women’s age and AMH.
Explanation of findings
These findings are in line with several studies which demonstrated that female age and AMH are the main predictors of pregnancy in IVF/ICSI treatment. Moreover, the primary objective of IVF treatments is to achieve a term live birth. As many studies proved before, there is a strong relationship between the number of eggs and the live birth rate(9). The number of eggs is directly proportional to age and AMH. Antimüllerian hormone is a strong predictor of ovarian reserve and of the outcome after IVF(10,11). The age-related decline of the success in IVF is largely attributable to a progressive decline of ovarian oocyte quality and quantity(12).
As our study shows, there is little or no influence on associated pathologies on cumulative pregnancy rate in POSEIDON groups. The reasons for this result might be due to appropriate ovarian stimulation protocols chosen for each patient and due to individualization of treatment.
It’s of extreme importance to know the factors that predict IVF success, because IVF specialists need to make informed decisions on IVF treatment and on ovarian stimulation regimens. Also, the patients need to be informed about the rate of success. The way the associated pathologies influence the pregnancy rate in POSEIDON groups represent an interesting hypothesis that needs further randomised controlled studies.
Conclusions
As previously known, variables that change pregnancy rate with statistically significance are: women’s age and AMH. The influence of the other pathologies in patients performing controlled ovarian stimulation for IVF/ICSI is of no statistical significance.
Following the study, we can draw the following conclusions:
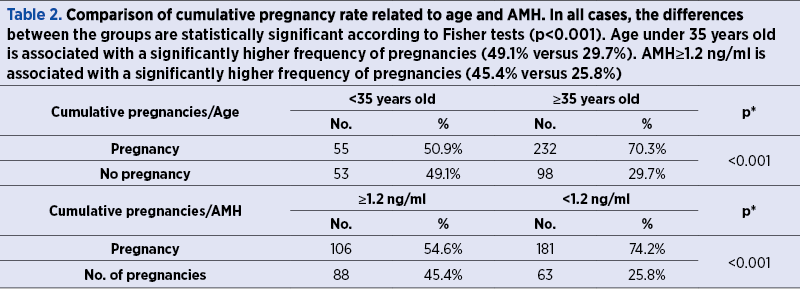
1. Age under 35 years old is associated with a significantly higher frequency of pregnancy.
2. AMH≥1.2 ng/ml is associated with a significantly higher frequency of pregnancy.
3. The comparison of the pregnancy rate in the POSEIDON groups according to the frequency of the investigated pathologies has no significant effect of changing the cumulative pregnancy rate, except for POSEIDON 1B group (patients <35 years old, AMH ≥1.2 ng/ml and 4-9 oocytes after controlled ovarian stimulation), where endometriosis had a negative effect on cumulative pregnancy rate.
Conflict of interests: The authors declare no conflict of interests.
Bibliografie
- Ferraretti AP, La Marca A, Fauser BCJM, Tarlatzis B, Nargund G, Gianaroli L. ESHRE consensus on the definition of “poor response” to ovarian stimulation for in vitro fertilization: the Bologna criteria. Human Reproduction. 2011;26(7):1616–1624.
- Frydman R. Poor responders: still a problem. Fertil Steril. 2011;96:1057.
- Broekmans FJ, Kwee J, Hendriks DJ, Mol BW, Lambalk CB, et al. A systematic review of tests predicting ovarian reserve and IVF outcome. Human Reprod Update. 2006;12:685–718.
- Papathanasiou A. Implementing the ESHRE ‘poor responder’ criteria in research studies: methodological implications. Hum Reprod. 2014;29:1835–8.
- Ferraretti AP, Gianaroli L. The Bologna criteria for the definition of poor ovarian responders: is there a need for revision? Hum Reprod. 2014;29:1842–1845.
- Devine K, Mumford SL, Wu M, DeCherney AH, Hill MJ, Propst A. Diminished ovarian reserve in the United States assisted reproductive technology population: diagnostic trends among 181,536 cycles from the Society for Assisted Reproductive Technology Clinic Outcomes Reporting System. Fertil Steril. 2015;104:612–9.
- Broer S, Mol B, Hendricks D, Broekmans F. The role of antimullerian hormone in prediction of outcome after IVF: comparison with antral follicle count. Fertil Steril. 2009;91:705–713.
- Humaidan P, Alviggi C, Fischer R, Esteves SC. The novel POSEIDON stratification of “Low prognosis patients in Assisted Reproductive Technology” and its proposed marker of successful outcome. F1000Research. 2016 Dec 23;5:2911.
- Sunkara SK, Rittenberg V, Raine-Fenning N, Bhattacharya S, Zamora J, Coomarasamy J. Association between the number of eggs and live birth in IVF treatment: an analysis of 400,135 treatment cycles. Human Reproduction. 2011 Jul;26(7):1768–1774.
- Kwee J, et al. Evaluation of anti-Müllerian hormone as a test for the prediction of ovarian reserve. Fertility and Sterility. 2008 Sep;90(3):737-43.
- Broer SL, Mol BW, Hendriks D, Broekmans FJ. The role of antimullerian hormone in prediction of outcome after IVF: comparison with the antral follicle count. Fertil Steril. 2009 Mar;91(3):705-14.
- Broekmans FJ, Kwee J, Hendriks DJ, Mol BW, Lambalk CB. A systematic review of tests predicting ovarian reserve and IVF outcome. Hum Reprod Update. 2006 Nov-Dec;12(6):685-718.