Prenatal detection of fetal anomalies allows the adequate counseling of the parents regarding the pregnancy and the neonatal prognosis. This is especially true in the case of congenital heart defects where counseling the parents is essential, given the high neonatal mortality of such anomalies. Conotruncal malformations are made up of a wide variety of congenital heart defects with abnormal ventriculoarterial connections and represent up to 30% of all cases of congenital heart defects. The most common types of conotruncal malformations are tetralogy of Fallot, transposition of great arteries, double outlet right ventricle, common arterial trunk, but numerous anatomical variants exist. The 3-vessel view can be used as an alternative to the ventricular outflow tract views to detect conotruncal malformations and may be used as a screening test. To test this hypothesis, we evaluated the 3-vessel view in both normal cases and cases of conotruncal malformations. As expected, in the 30 normal cases we reviewed, all the criteria for a normal 3-vessel view were met. In the 15 cases of conotruncal malformations (tetralogy of Fallot, transposition of great arteries, double outlet right ventricle, common arterial trunk) that we investigated, at least one criterion for a normal 3-vessel view was not met. This goes to show the utility the 3-vessel view can have in the screening for conotruncal malformations
Imaginea de 3 vase ca metodă de screening a malformaţiilor conotruncale
The 3-vessel view as a means of screening for conotruncal malformations
First published: 16 martie 2020
Editorial Group: MEDICHUB MEDIA
DOI: 10.26416/ObsGin.68.1.2020.3037
Abstract
Rezumat
Detecţia prenatală a anomaliilor fetale permite informarea şi consilierea adecvată a părinţilor privind prognosticul sarcinii şi evoluţia neonatală. Acest lucru este esenţial mai ales la cazurile de malformaţii cardiace, având în vedere rata mare de mortalitate neonatală întâlnită în aceste cazuri. Malformaţiile conotruncale reprezintă un grup heterogen de anomalii cardiace caracterizate de o anomalie a conexiunii ventriculoarteriale. Ca incidenţă, reprezintă până la 30% din totalul malformaţiilor cardiace. Cele mai frecvente malformaţii conotruncale sunt tetralogia Fallot, transpoziţia de mari vase, ventriculul drept cu dublă cale de ejecţie, trunchiul arterial comun, dar există numeroase forme anatomice. Secţiunea de 3 vase poate fi folosită ca o alternativă în locul secţiunilor cu tracturile de ejecţie a ventriculilor pentru a detecta malformaţiile conotruncale în cadrul screeningului cardiac fetal. Pentru a verifica această ipoteză, am evaluat imaginea de 3 vase la un lot de cazuri normale şi la un lot de cazuri cu malformaţii conotruncale. Aşa cum era de aşteptat la cele 30 de cazuri normale, toate criteriile pentru o imagine ecografică de 3 vase normală au fost îndeplinite. În lotul de 15 cazuri de malformaţii conotruncale studiate (tetralogie Fallot, transpoziţie de mari vase, ventricul drept cu dublă cale de ejecţie, trunchi arterial comun), la fiecare caz în parte, cel puţin un criteriu pentru o imagine de 3 vase normală nu a fost îndeplinit. Aceste rezultate vin să confirme utilitatea imaginii de 3 vase în screeningul cardiac fetal şi în special în detecţia malformaţiilor conotruncale.
Introduction
Prenatal detection of fetal anomalies allows the adequate counseling of the parents regarding the pregnancy and the neonatal prognosis. This is especially true in the case of congenital heart defects (CHD), where counseling the parents is essential, given the high neonatal mortality of such anomalies. Also, the prenatal diagnostics improves outcome, by delivering the newborn in a tertiary center with adequate neonatal therapy and the possibility for cardiac surgery(1).
Conotruncal malformations (CTM) represent a wide variety of congenital heart defects with abnormal ventriculoarterial connections. CTM are an important subgroup of CHD, as they represent up to 30% of all cases of CHD(2). The most common types of CTM are tetralogy of Fallot (TOF), transposition of great arteries (TGA), double outlet right ventricle (DORV) and common arterial trunk (CAT), but numerous anatomical variants exist(3,4). The prenatal detection of such conditions is challenging, especially for less experienced examiners, because in most cases during the second-trimester screening, there is a normal 4-chamber view of the heart(5). To correctly diagnose CTM, a detailed fetal echocardiography is usually needed, as these CHD are usually complex and require a good understanding of the cardiac morphology and spacial representation(6,7). The assessment of the ventricular outflow trac views and the great arteries is essential for establishing a complete and detailed diagnosis in CTM. The problem is that these views are slightly oblique planes and are hard to be obtained during routine screening. As Gianluigi Pilu pointed out, they are “beyond the capability of the vast majority of sonographers performing fetal sonographic screening”(8). This is probably why the detection rate for CTM remains much lower than for the rest of CHD, despite the new screening guidelines that include the ventricular outflow tracts as mandatory, especially in cases where the 4-chamber view is normal or slightly “abnormal”(9,10).
One solution for improving the detection rate for CTM would be to use a simpler CHD screening protocol that is more accessible to less experienced examiners. Such a protocol was proposed in 2017 by Herghelegiu et al. and it relied solely on the 4-chamber view and 3-vessel view as ultrasound screening planes(11). In this protocol, 3-vessel view is used to detect CHD that involve the great vessels and the ventricular outflow tracts. To test the performance of such a protocol, we set out to assess the 3-vessel view in four of the most common CTM that may have a normal/“nearly normal” 4-chamber view: TOF, TGA, DORV, CAT.
Materials and method
We performed a retrospective study by analyzing ultrasound recordings (videos and images) of CTM cases from the personal archive of Dr. Doru Herghelegiu and Dr. Cătălin Herghelegiu, cases that are included in the PhD thesis “Secţiunile 4 camere şi 3 vase – rol în evaluarea cardiacă fetală”. The ultrasound scans were performed on Voluson 730Expert, E8 ultrasound machines, using transabdominal transducers, between October 2016 and December 2019. The gestational age of the fetuses was 18-28 weeks. Only cases of TOF, TGA, DORV and CAT with a “nearly normal” 4-chamber view were selected. From those cases, the 3-vessel view images were analyzed to check if they were normal or abnormal. Also, the 3-vessel view images from 30 normal, consecutive “control” cases were analyzed.
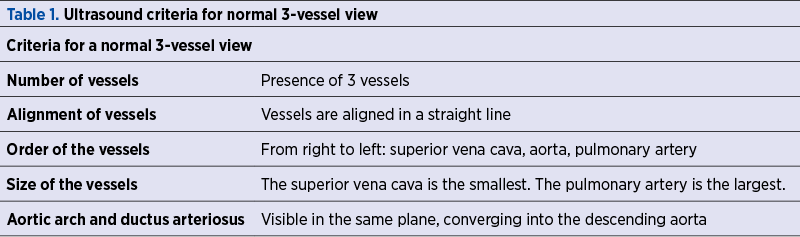
To define the 3-vessel view, we used both the description given originally by Yoo et al. and the one given later by Yagel et al., who describe a slightly more cephalic plane than the original one(12,13). The 3-vessel view described by Yoo is a transverse section across the thorax at the level of the upper mediastinum. In this image, the 3 vessels are seen aligned from right to left, the superior vena cava, the smallest in size, the aorta in the middle and the pulmonary artery, the largest and most anterior vessel, continuing posteriorly with the ductus arteriosus (Figure 1A). If the slightly more cephalic plane, described by Yagel, is chosen, the aortic arch and ductus arteriosus can be observed converging into the descending aorta (Figure 1B). In this view, the trachea is visible and the aortic arch can be observed passing to the left of it.
A series of criteria were selected to define a 3-vessel view image as normal or abnormal and to rule out a CTM (Table 1). If one of these criteria was not met, then the image would be considered abnormal and the case as having a CTM. Furthermore, we tried to describe a pattern of abnormal findings depending on the type of CTM, such that a possible diagnostic could at least be suggested.
Results
All 15 CTM cases had an abnormal 3-vessel view image, failing to meet at least one criterion from Table 1. The following types of CTM were found: 7 cases of TOF, 3 cases of TGA, 3 cases of DORV, 2 cases of CAT. All 3-vessel view images from the control cases met all the criteria from Table 1 and were considered normal.
Tetralogy of Fallot
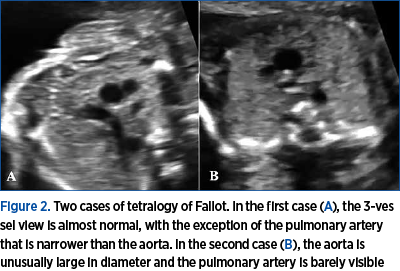
In cases with TOF, the 3 vessels were visible, but the aorta appears slightly anterior such that the vessels are no longer aligned in a straight line. This is because the aorta is overriding the interventricular septum and has a slightly altered course. More importantly, the pulmonary artery is smaller in diameter than the aorta, as pulmonary valve stenosis is one of the four characteristics of TOF (Figure 2A). In the one case with critical pulmonary valve stenosis, the pulmonary artery and ductus arteriosus were barely visible, giving the impression that only 2 vessels are present (Figure 2B). Of the four types of CTM described in this article, TOF has the closest resemblance to the normal 3-vessel view image.

Transposition of great arteries
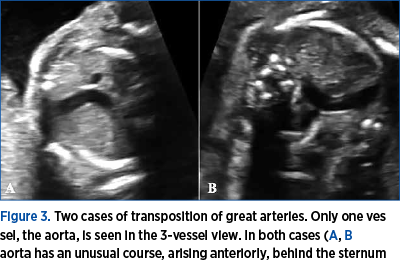
In cases with TGA, the 3 vessels are usually not visible in the same plane as the pulmonary artery and the ductus are located in a much more caudal plane than the ascending aorta and aortic arch. As a consequence, in most cases in the 3-vessel view, usually only the aorta is seen. In the more cephalic 3-vessel plane described by Yagel, only the aortic arch is visible. Also, the aorta has a much more anterior position, behind the sternum, as it emerges from the right ventricle (Figure 3).
Double outlet right ventricle
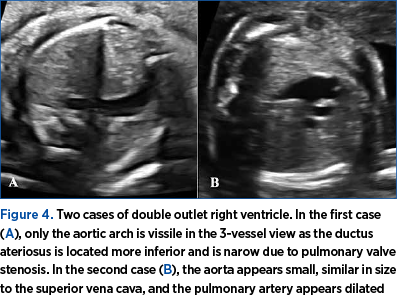
The cases with DORV proved to be heterogenous in appearance, but all of them had an abnormal 3-vessel view image. This is because in this CTM there are usually multiple structural abnormalities associated. First of all, the aorta is usually transposed to the right of the pulmonary artery, so during the ultrasound examination an appearance similar to that of TGA is seen. Thus, it is not possible to visualize both the aortic arch and the ductus arteriosus in the same plane (Figure 4A). Secondly, in many cases, either the pulmonary or aortic valves are stenotic and, as a consequence, the corresponding great artery appears narrower in the 3-vessel view (Figure 4B). One case also had a right aortic arch visible in the 3-vessel view.
Common arterial trunk
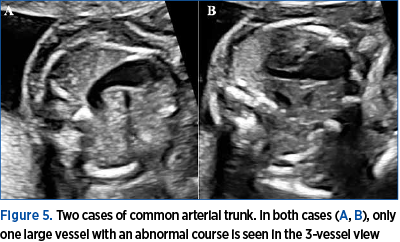
The cases with CAT were by far the most easily recognizable, as the 3-vessel view was in all cases completely abnormal. A single large, common arterial vessel, with an abnormal course, was seen in all cases (Figure 5). Depending on the subtype of CAT, separate pulmonary arterial branches or a pulmonary trunk could be seen emerging from this common arterial vessel.
Discussion and conclusions
CTM are complex CHD, with many anatomical variants that are difficult to be detected and accurately described prenatally or even in some cases postnatally(4,14). The 3-vessel view can be a useful tool for CHD screening and especially for detecting CTM. As shown in our study, the most common types of CTM (TOF, TGA, DORV, CAT) have an abnormal 3-vessel view and would be detected by a screening protocol based on this view. If only one arterial vessel is seen on the 3-vessel view, it is a sign of severity, suggesting a complex CTM, such as TGA, CAT or severe stenosis of either the aortic or pulmonary valve. These malformations may require immediate cardiac surgery after birth. An advantage of the 3-vessel view in comparison to the ventricular outflow tract views is that the former is a transverse plane with simple to follow criteria for a normal image, while the later is represented by oblique planes that are difficult to be obtained and require an experienced examiner. The 3-vessel view should become a mandatory part of the fetal cardiac screening in the second trimester.
Conflict of interests: The authors declare no conflict of interests.
Bibliografie
2. Galindo A, Mendoza A, Arbues J, Grañeras A, Escribano D, Nieto O. Conotruncal anomalies in fetal life: Accuracy of diagnosis, associated defects and outcome. Eur J Obstet Gynecol Reprod Biol. 2009; 146:55–60.
3. Lacour-Gayet F, Bove EL, Hraska V, Morell VO, Spray TL (eds). Surgery of conotruncal anomalies. Springer International Publishing. 2016.
4. Herghelegiu CG, Bacalbaşa N, Oprescu ND. Differential Diagnosis between Double Outlet Right Ventricle and Transposition of Great Arteries. 5th Congr Rom Soc Ultrasound Obstet Gynecol. 2017; 294–297.
5. Vaidyanathan B, Kumar S, Sudhakar A, Kumar RK. Conotruncal anomalies in the fetus: Referral patterns and pregnancy outcomes in a dedicated fetal cardiology unit in South India. Ann Pediatr Cardiol. 2013; 6:15–20.
6. Gelehrter S, Owens ST, Russell MW, van der Velde ME, Gomez-Fifer C. Accuracy of the Fetal Echocardiogram in Double-outlet Right Ventricle. Congenit Heart Dis. 2007; 2:32–37.
7. Forbus GA, Atz AM, Shirali GS. Implications and limitations of an abnormal fetal echocardiogram. Am J Cardiol. 2004; 94:688–689.
8. Campbell S, Allan L, Benacerraf B, Copel JA, Carvalho JS, Chaoui R, Eik-Nes SH, Tegnander E, Gembruch U, Huhta JC, Pilu G, Wladimiroff J, Yagel S. Isolated major congenital heart disease. Ultrasound Obstet Gynecol. 2001; 17:370–379.
9. Pinto NM, Keenan HT, Minich LL, Puchalski MD, Heywood M, Botto LD. Barriers to prenatal detection of congenital heart disease: a population-based study. Ultrasound Obstet Gynecol. 2012; 40:418–425.
10. Van Velzen CL, Clur SA, Rijlaarsdam MEB, Bax CJ, Pajkrt E, Heymans MW, Bekker MN, Hruda J, De Groot CJM, Blom NA, Haak MC. Prenatal detection of congenital heart disease - Results of a national screening programme. BJOG An Int J Obstet Gynaecol. 2016; 123:400–407.
11. Herghelegiu CG, Drăgan I, Suciu N, Oprescu ND. A Simplified Protocol for Congenital Heart Disease. 5th Congr Rom Soc Ultrasound Obstet Gynecol. 2017; 298–302.
12. Yoo SJ, Lee Y-H, Kim ES, Ryu HM, Kim MY, Choi H-K, Cho KS, Kim A. Three-vessel view of the fetal upper mediastinum: an easy means of detecting abnormalities of the ventricular outflow tracts and great arteries during obstetric screening. Ultrasound Obstet Gynecol. 1997; 9:173–182.
13. Yagel S, Arbel R, Anteby EY, Raveh D, Achiron R. The three vessels and trachea view (3VT) in fetal cardiac scanning. Ultrasound Obstet Gynecol. 2002; 20:340–345.
14. Perde F, Herghelegiu CG, Iosifescu AG, Crîngu I, Luca L, Dragu M. Pulmonary artery aneurysm in a marfanoid adult patient with unoperated functional single ventricle and levo-transposition of the great arteries. Rom J Leg Med. 2018; 26:363–368.