Impactul clasificării moleculare în managementul cancerului de endometru
The impact of molecular classification on endometrial cancer management
Abstract
Introduction. Endometrial cancer is one of the most frequent gynecological cancers. Over the years, there has been more and more interest in the molecular characteristics of endometrial tumors that led to the molecular classification in 2013 of the endometrial cancer, with four molecular subtypes, with specific prognosis and treatment.
Materials and method. We performed a narrative literature review in order to establish the changes that have been brought by the implementation of the molecular classification for endometrial cancer. We used the PubMed database, with a defined timed interval from 2013 to 2023, using the following keywords: “endometrial cancer”, “molecular classification”, “endometrial cancer management”. We selected the most appropriate articles which reflect our topic.
Results. International societies have widely adopted the molecular classification and included it in algorithms in order to determine a risk classification. Further, staging and treatment options are based on these specific risk groups, which has led to shifts and changes to the way certain tumors were treated until now. Also, molecular classification has led the way to personalized treatment concerning adjuvant therapy.
Conclusions. The introduction of molecular classification in clinical practice has made significant changes in endometrial cancer management, and important studies are ongoing, with the purpose of finding more therapeutic resources for every endometrial cancer subtype.
Keywords
endometrial cancermolecular classificationPOLEp53MMRdRezumat
Introducere. Cancerul de endometru este unul dintre cele mai frecvente cancere gincologice. Pe parcursul ultimilor ani, s-a constatat un interes din ce în ce mai mare pentru caracteristicile moleculare ale celulelor tumorale endometriale, interes ce a culminat cu apariţia în anul 2013 a clasificării moleculare a cancerului de endometru. Astfel, tumorile endometriale au fost împărţite în patru grupe, cu prognostic şi opţiuni terapeutice proprii.Materiale şi metodă. Am realizat o revizuire a literaturii de specialitate cu scopul de a sublinia schimbările apărute în managementul cancerului de endometru în urma introducerii clasificării moleculare. Am folosit baza de date PubMed, utilizând următoarele cuvinte-cheie: cancer endometrial, clasificare moleculară, management cancer endometrial. Am selectat cele mai relevante articole publicate între anii 2013 şi 2023.
Rezultate. Societăţile internaţionale au adoptat clasificarea moleculară, introducând-o în algoritmi care au ca scop încadrarea tumorilor de endometru în grupe de risc. Stadializarea propriu-zisă şi opţiunile de tratament se bazează pe această grupare în funcţie de risc, fapt care a condus la schimbări substanţiale în ceea ce priveşte tratamentul anumitor tipuri de cancer de endometru. În acelaşi timp, clasificarea moleculară a permis personalizarea tratamentului adjuvant.
Concluzii. Introducerea clasificării moleculare în practica de zi cu zi a condus la schimbări substanţiale în ceea ce priveşte managementul actual al cancerului de endometru. Studii importante sunt în plină desfăşurare, cu scopul de a găsi noi resurse terapeutice pentru fiecare subtip de cancer endometrial.
Cuvinte Cheie
cancer de endometruclasificare molecularăPOLEp53MMRdIntroduction
Endometrial cancer is one of the most frequent gynecological cancers in the developed countries and the fourth cancer in women worldwide(1). The most important tool for treatment is surgery, incipient cases being treated by surgery alone, while advanced stages are also treated with adjuvant therapy.
Traditionally, endometrial cancer was divided into two categories, according to Bockhman in 1983: a type I estrogen-driven cancer, mostly endometrioid, with a more favorable prognosis, and a type II non-estrogenic cancer, which comprised more aggressive histologies (serous, clear cell), with a poorer prognosis(2). Although this classification was of great use initially, it became clear that endometrial cancer was characterized by more complexity. While for advanced stage disease, the therapeutic decision is pretty straightforward, the main problems were raised by the early stages, where it was difficult to decide which cases needed adjuvant therapy and which not. The situation was further complicated by the fact that histologic grade assignment was not as reliable on the biopsy specimen, being frequently upgraded on the hysterectomy specimen(3).
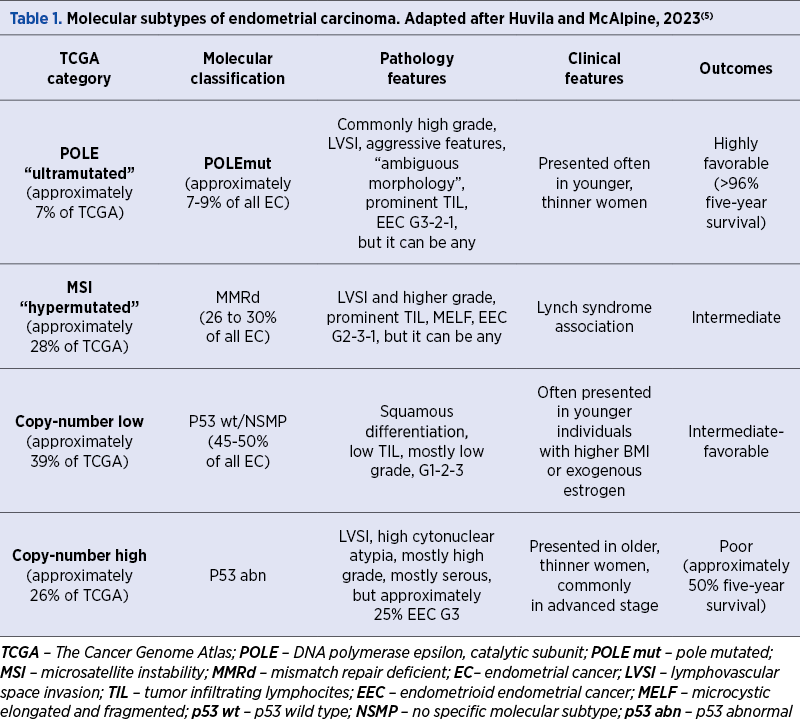
As knowledge of molecular pathogenesis became more and more abundant, it became clear that it could be of use to better categorize and predict endometrial cancer. A turning point was the year 2013, when The Cancer Genome Atlas (TCGA) identified four molecular subtypes (Table 1) of endometrial cancer based on tumor cell genomic characteristics and established for each of them a prognostic outcome and a clinicopathologic feature(4).
Materials and method
We performed a narrative literature review in order to compress the latest abundant information on endometrial cancer classification and the changes it has brought to its management. We used the PubMed database, with a defined timed interval from 2013 to 2023, using the following keywords: “endometrial cancer”, “molecular classification”, “endometrial cancer management”. We selected the articles which related most to our interest.
Results
After the TCGA publication of the molecular classification, a clinical algorithm was published that is designed to diagnose one of the four molecular subtypes, as a surrogate for molecular testing – the PROMISE algorithm (Proactive Molecular Risk Classifier for Endometrial Cancer; Figure 1). The algorithm can be applied to diagnostic biopsies and is highly reproductible(6). Also, it established a consensus on nomenclature which was later adopted by the World Health Organization and characterized a group of rare mutations named “multiple classifier”, were tumors exhibit more than one key molecular characteristic.
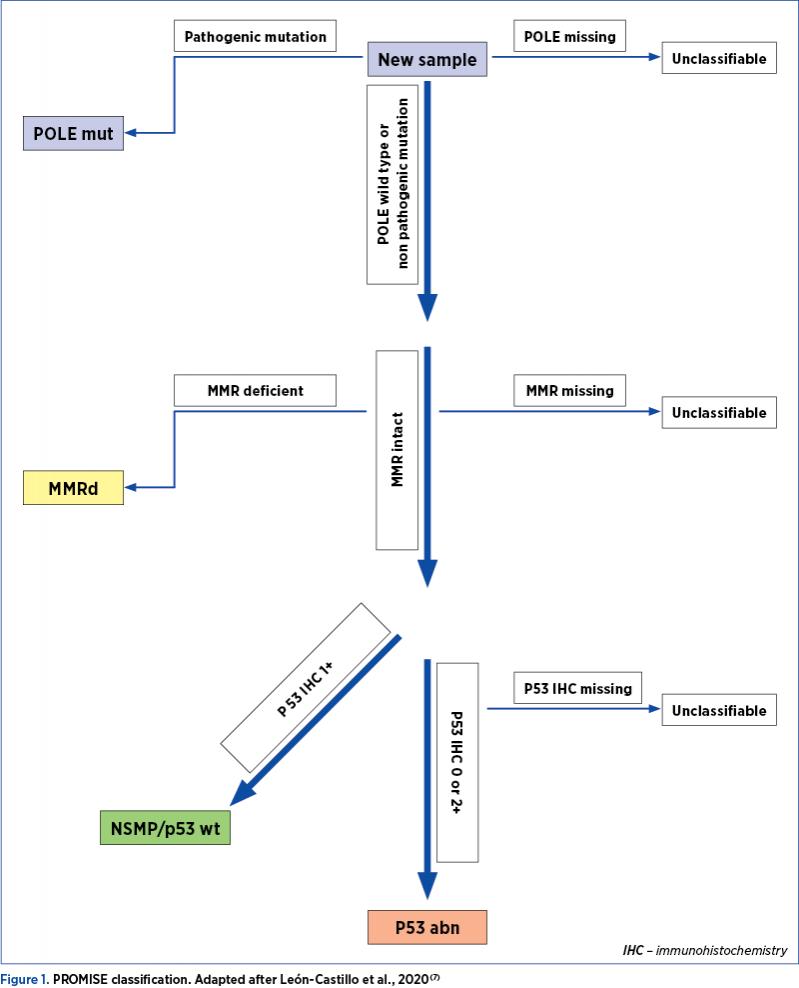
First, the POLE mutated endometrial cancers are pulled out. Next, the mismatch repair deficiency (loss of MMR proteins) cancers are identified, finally diagnosing patients with aberrant versus wild type p53. There is a rare category of “multiple classifier” endometrial carcinomas represented by tumor cells that have more than one key classification feature, and these occur in approximately 3% of cases. The aforementioned method is the correct way to segregate these rare tumors(7). In 2020, the World Health Organization (WHO) published the new terminology in the Classification of Female Genital Tumors.
1. POLE mutated subtype (POLEmut; TCGA “POLE ultramutated”)
These tumors are characterized by a very high number of somatic mutations. Most of them are endometrioid cancers, and patients with this mutation are often thin and young. They have a favorable outcome, even though the tumor has aggressive characteristics, such as high grading or lymphovascular space invasion (LVSI)(8,9). POLE mutated cancer has no advantages after adjuvant therapy. The tendency is to de-escalate treatment in these cases, and there are studies ongoing which will decide the best management for these patients(10).
2. Mismatch repair deficiency subtype (MMRd; TCCGA “MSI hypermutated”)
Tumors in this group have dysfunctional mismatch repair (MMR) proteins represented by MLH1, PMS2, MSH2 and MSH6. This group is also characterized by germline mutations, and 2% to 5% of endometrial cancers with MMR deficiency are associated with Lynch syndrome (hereditary non-polyposis colorectal cancer – HNPCC). Patients with this condition are predisposed to a variety of cancers, especially colorectal, endometrial and/or ovarian cancer. An important aspect when diagnosing a patient with this type of tumor is to establish strategies for cancer risk reduction. There has been no evident disease outcome characteristics found in this group. The treatment with immune checkpoint inhibitors is being used in metastatic disease in this group(11).
3. No specific molecular profile (NSMP; TCGA copy number-low; previously p53 wild type)
These tumors have a stable genome, and the disease outcome is usually intermediate to favorable. The majority of endometrioid cancers with hormonal receptors are included in this category(12).
4. p53 abnormal (p53abn; TCCGA copy-number high [serous-like])
Tumors in this group are similar to high-grade serous ovarian carcinoma and basal-like breast carcinoma, all of them having TP 53 mutations.
The prognosis is poor for these patients. Most of the cancers included in this group are serous carcinoma, carcinosarcoma and clear cell carcinoma. Patients in this group might benefit from chemotherapy alongside radiation therapy(13).
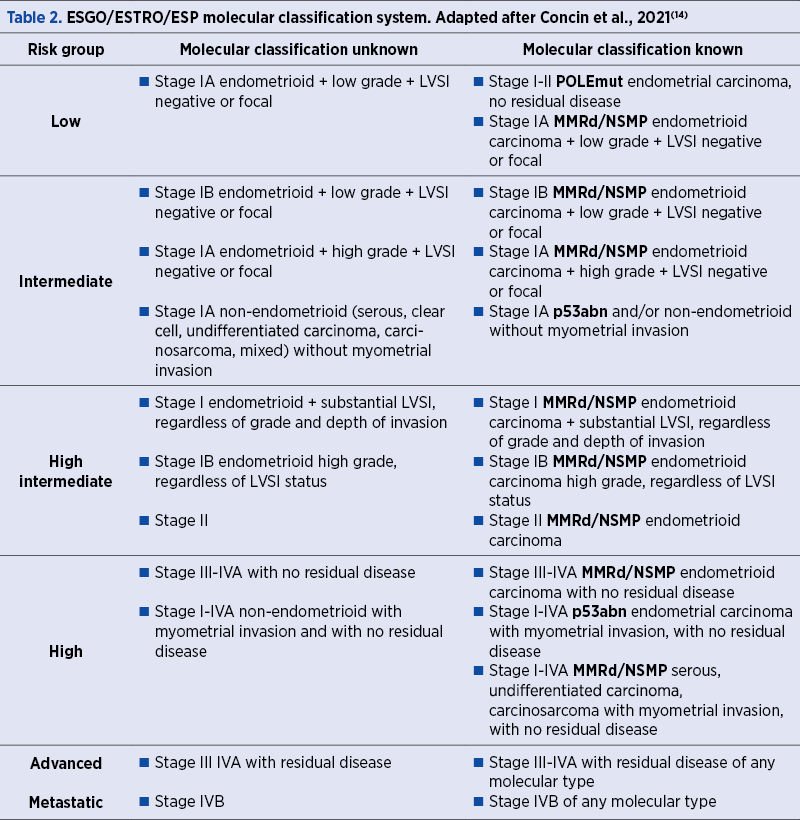
In 2021, the European Society of Gynecological Oncology (ESGO), the European Society for Radiotherapy and Oncology (ESTRO) and the European Society of Pathology (ESP) published guidelines which integrated the molecular features into assignment of the risk groups. Until then, endometrial cancers were classified into risk groups based on the traditional clinicopathologic system (tumor histology, stage of disease, grade and lymphovascular space invasion). From 2021, mainly all early-stage (I and II) POLE mutated cancers were assigned as “low risk”, with no adjuvant therapy recommended and staging p53abn stage IA endometrial cancer as “high risk”, with a recommendation for chemotherapy(14).
Currently, histologic type, grade, myometrial invasion and LVSI should be recorded in all patients, and molecular classification is encouraged in all cases(14). The ESGO/ESTRO/ESP guidelines mention that POLE mutation may be omitted in cases of low-risk and intermediate-risk endometrial carcinoma with low-grade histology(14). Then, patients can be assigned to one of the following risk groups, as presented in Table 2.
Endometrial cancer is surgically staged using the International Federation of Gynecology and Obstetrics (FIGO) classification. In 2023, a new classification was published which included the molecular classification, various histological types and tumor patterns in addition to the previous one (Tables 3 and 4)(15).
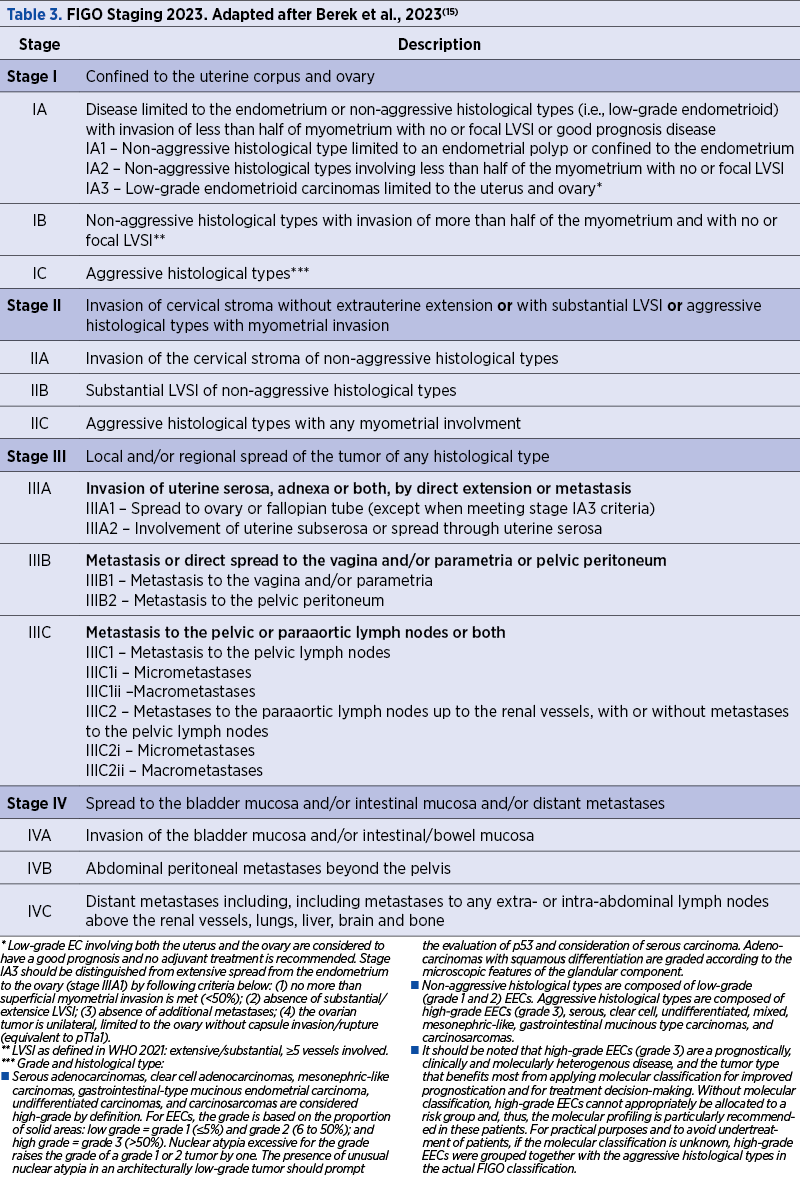
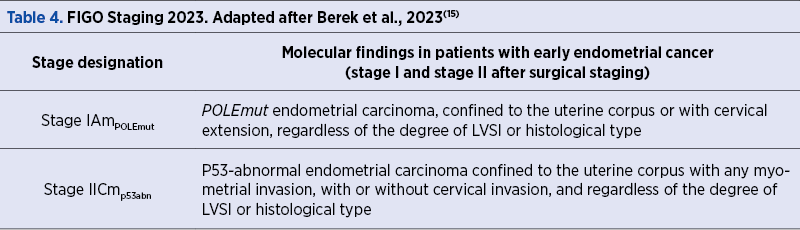
In the current FIGO classification, if the POLE mutation is present, the tumor is staged as IAmPOLEmut if it is confined to the uterus or has cervical extension, regardless of the degree of LVSI or of the histological type(15). On the opposite, if p53abn is present, the tumor, regardless of LVSI, with any myometrial invasion, with or without cervical extension, is classified as IICmp53abn(15).
Discussion
Endometrial cancer management has changed in many ways since the introduction of molecular classification. Staging of tumors has changed, therefore the treatment has been downstaged for POLE mutated cancer, while cases considered priorly as low risk have been upgraded to high risk, even in the case of small tumors. Survival has been shown to be considerably different with this new staging for stages I and II, but not for advanced stages(15).
The surgical management has also changed due to the different risk group classification. Surgical lymph node staging is recommended for high-intermediate risk and high-risk groups, while sentinel lymph node is an acceptable method for stages I and II(14). In low-risk and intermediate-risk disease, sentinel lymph node biopsy can be considered, but systemic lymphadenectomy is discouraged(14). Consequently, higher stages with POLE mutation can now skip systemic lymphadenectomy, which is known for its important complications associated with lymph node drainage issues(16). On the contrary, some of the p53abn cancers which would have not had necessarily a sentinel lymph node biopsy are now more prone to have a biopsy, which leads to better staging(14).
Nonsurgical treatment has also changed significantly, since personalized therapy is now possible when molecular characteristics are present. Elimination of adjuvant treatment for POLE mutations, addition of immune checkpoint inhibitors, the benefits of radiotherapy for MMRd tumors and the use of chemotherapy in p53abn tumors are all due to the new information regarding the molecular characteristics(17). Studies are ongoing to determine the best approach in each of these groups(18).
There is great interest nowadays towards fertility preserving treatment for endometrial cancer, due to a higher incidence in women of childbearing age(19). This is mainly explained by the western lifestyle which includes an accumulation of risk factors such as excess weight gain, diabetes mellitus, hypertension and high serum triglycerides, combined with an increase in the age when women decide to conceive(20). At present, fertility preserving management in reserved only for cancers confined to the endometrium, grade I with endometrioid histology(14). Molecular classification may have an important place in the future, because it may include more cases in the fertility preserving group.
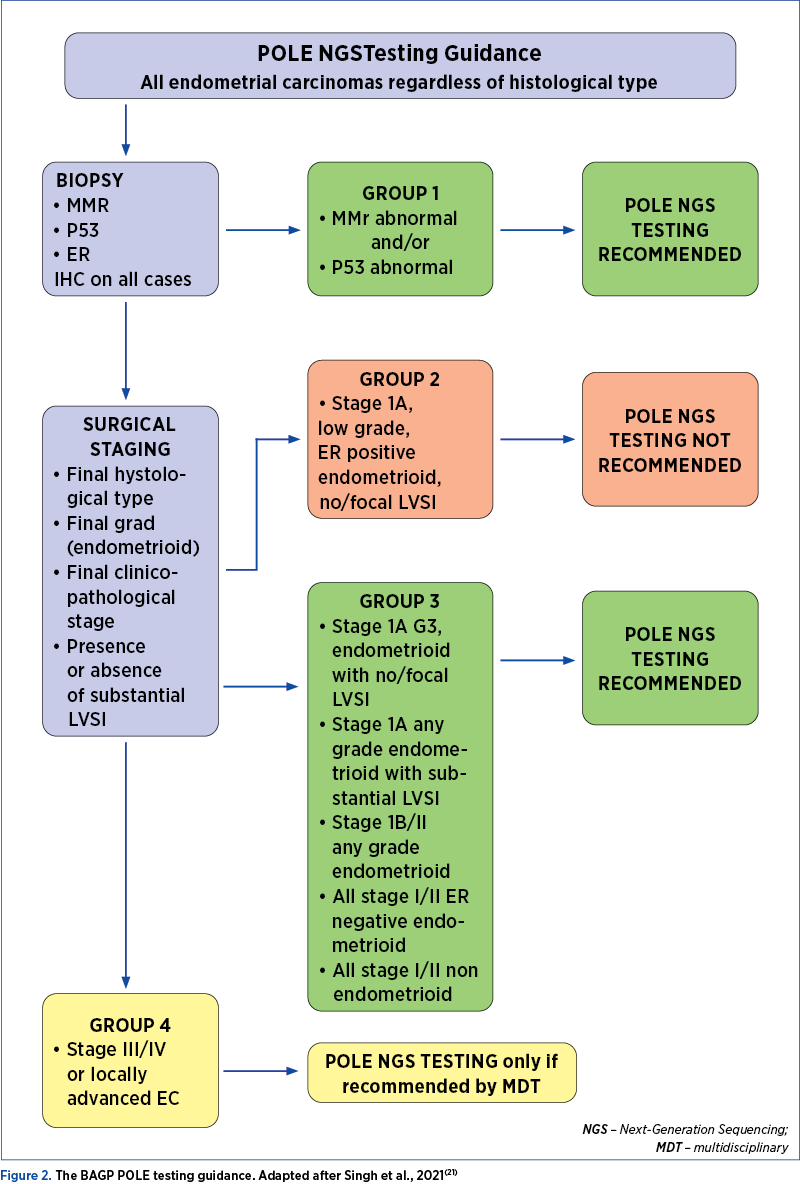
A problem concerning the molecular classification is the ability to perform it. Resources for molecular testing are not widely available, even in developed countries. The ESGO/ESTRO/ESP guidelines mention that POLE mutation may be omitted in low-risk and intermediate-risk endometrial carcinoma with low-grade histology(14). Also, it is mentioned that when resources are scarce, some cases should be prioritized such as high-risk cases, where adjuvant therapy is greatly influenced by the classification(14). Nevertheless, if molecular classification tools are not available, endometrial carcinoma classification should be based on traditional pathologic characteristics(14). The British Association of Gynecological Pathologists has published a guideline in 2022 which proposed testing for POLE mutation only in selected cases, in order to improve cost efficiency (Figure 2)(21).
Conclusions
The management of endometrial cancer has changed greatly since the introduction of molecular classification. Surgical staging is different from the past, and tumors thought to be aggressive are now known to have an excellent prognosis, while some of them need multiple treatment methods. The decision to add or not adjuvant treatment is now based on molecular classification for specific cases. Also, personalized treatment is now possible and will be further adjusted according to ongoing studies.
Conflict of interest: none declared
Financial support: none declared
This work is permanently accessible online free of charge and published under the CC-BY.

Bibliografie
- World Fact Sheets. The Global Cancer Observatory. [2021.10.10]. https://gco.iarc.fr/today/data/factsheets/populations/900-world-fact-sheets.pdf.
- Bokhman JV. Two pathogenetic types of endometrial carcinoma. Gynecol Oncol. 1983;15(1):10-7.
- Batista TP, Cavalcanti CL, Tejo AA, Bezerra AL. Accuracy of preoperative endometrial sampling diagnosis for predicting the final pathology grading in uterine endometrioid carcinoma. Eur J Surg Oncol. 2016 Sep;42(9):1367-71.
- Cancer Genome Atlas Research Network; Kandoth C, Schultz N, Cherniack AD, Akbani R, Liu Y, Shen H, Robertson AG, Pashtan I, Shen R, Benz CC, Yau C, Laird PW, Ding L, Zhang W, Mills GB, Kucherlapati R, Mardis ER, Levine DA. Integrated genomic characterization of endometrial carcinoma [Erratum in: Nature. 2013;500(7461):242]. Nature. 2013;497(7447):67-73.
- Huvila J, McAlpine N. Endometrial cancer: Pathology and classification. UpToDate. 2023 Oct.
- Kommoss S, McConechy MK, Kommoss F, Leung S, Bunz A, Magrill J, Britton H, Kommoss F, Grevenkamp F, Karnezis A, Yang W, Lum A, Krämer B, Taran F, Staebler A, Lax S, Brucker SY, Huntsman DG, Gilks CB, McAlpine JN, Talhouk A. Final validation of the ProMisE molecular classifier for endometrial carcinoma in a large population-based case series. Ann Oncol. 2018;29(5):1180-1188.
- León-Castillo A, Gilvazquez E, Nout R, Smit VT, McAlpine JN, McConechy M, Kommoss S, Brucker SY, Carlson JW, Epstein E, Rau TT, Soslow RA, Ganesan R, Matias-Guiu X, Oliva E, Harrison BT, Church DN, Gilks CB, Bosse T. Clinicopathological and molecular characterisation of ‘multiple-classifier’ endometrial carcinomas. J Pathol. 2020;250(3):312-322.
- Stasenko M, Tunnage I, Ashley CW, Rubinstein MM, Latham AJ, Da Cruz Paula A, Mueller JJ, Leitao MM Jr, Friedman CF, Makker V, Soslow RA, DeLair DF, Hyman DM, Zamarin D, Alektiar KM, Aghajanian CA, Abu-Rustum NR, Weigelt B, Cadoo KA. Clinical outcomes of patients with POLE mutated endometrioid endometrial cancer. Gynecol Oncol. 2020;156(1):194-202.
- McAlpine JN, Chiu DS, Nout RA, Church DN, Schmidt P, Lam S, Leung S, Bellone S, Wong A, Brucker SY, Lee CH, Clarke BA, Huntsman DG, Bernardini MQ, Ngeow J, Santin AD, Goodfellow P, Levine DA, Köbel M, Kommoss S, Bosse T, Gilks CB, Talhouk A. Evaluation of treatment effects in patients with endometrial cancer and POLE mutations: An individual patient data meta-analysis. Cancer. 2021;127(14):2409-2422.
- van den Heerik ASVM, Horeweg N, Nout RA, Lutgens LCHW, van der Steen-Banasik EM, Westerveld GH, van den Berg HA, Slot A, Koppe FLA, Kommoss S, Mens JWM, Nowee ME, Bijmolt S, Cibula D, Stam TC, Jurgenliemk-Schulz IM, Snyers A, Hamann M, Zwanenburg AG, Coen VLMA, Vandecasteele K, Gillham C, Chargari C, Verhoeven-Adema KW, Putter H, van den Hout WB, Wortman BG, Nijman HW, Bosse T, Creutzberg CL. PORTEC-4a: international randomized trial of molecular profile-based adjuvant treatment for women with high-intermediate risk endometrial cancer. Int J Gynecol Cancer. 2020;30(12):2002-2007.
- Le DT, Uram JN, Wang H, Bartlett BR, Kemberling H, Eyring AD, Skora AD, Luber BS, Azad NS, Laheru D, Biedrzycki B, Donehower RC, Zaheer A, Fisher GA, Crocenzi TS, Lee JJ, Duffy SM, Goldberg RM, de la Chapelle A, Koshiji M, Bhaijee F, Huebner T, Hruban RH, Wood LD, Cuka N, Pardoll DM, Papadopoulos N, Kinzler KW, Zhou S, Cornish TC, Taube JM, Anders RA, Eshleman JR, Vogelstein B, Diaz LA Jr. PD-1 Blockade in Tumors with Mismatch-Repair Deficiency. N Engl J Med. 2015;372(26):2509-20.
- Jamieson A, Huvila J, Chiu D, Thompson EF, Scott S, Salvador S, Vicus D, Helpman L, Gotlieb W, Kean S, Samouelian V, Köbel M, Kinloch M, Parra-Harran C, Offman S, Grondin K, Irving J, Lum A, Senz J, Leung S, McConechy MK, Plante M, Kommoss S, Huntsman DG, Talhouk A, Gilks CB, McAlpine JN. Grade and Estrogen Receptor Expression Identify a Subset of No Specific Molecular Profile Endometrial Carcinomas at a Very Low Risk of Disease-Specific Death. [Erratum in: Mod Pathol. 2023;36(6):100212]. Mod Pathol. 2023;36(4):100085.
- León-Castillo A, de Boer SM, Powell ME, Mileshkin LR, Mackay HJ, Leary A, Nijman HW, Singh N, Pollock PM, Bessette P, Fyles A, Haie-Meder C, Smit VTHBM, Edmondson RJ, Putter H, Kitchener HC, Crosbie EJ, de Bruyn M, Nout RA, Horeweg N, Creutzberg CL, Bosse T; TransPORTEC Consortium. Molecular Classification of the PORTEC-3 Trial for High-Risk Endometrial Cancer: Impact on Prognosis and Benefit from Adjuvant Therapy. J Clin Oncol. 2020;38(29):3388-3397.
- Concin N, Matias-Guiu X, Vergote I, Cibula D, Mirza MR, Marnitz S, Ledermann J, Bosse T, Chargari C, Fagotti A, Fotopoulou C, Gonzalez Martin A, Lax S, Lorusso D, Marth C, Morice P, Nout RA, O’Donnell D, Querleu D, Raspollini MR, Sehouli J, Sturdza A, Taylor A, Westermann A, Wimberger P, Colombo N, Planchamp F, Creutzberg CL. ESGO/ESTRO/ESP guidelines for the management of patients with endometrial carcinoma. Int J Gynecol Cancer. 2021;31(1):12-39.
- Berek JS, Matias-Guiu X, Creutzberg C, Fotopoulou C, Gaffney D, Kehoe S, Lindemann K, Mutch D, Concin N; Endometrial Cancer Staging Subcommittee, FIGO Women’s Cancer Committee. FIGO staging of endometrial cancer: 2023. Int J Gynaecol Obstet. 2023;162(2):383-394.
- Carlson JW, Kauderer J, Hutson A, Carter J, Armer J, Lockwood S, Nolte S, Stewart BR, Wenzel L, Walker J, Fleury A, Bonebrake A, Soper J, Mathews C, Zivanovic O, Richards WE, Tan A, Alberts DS, Barakat RR. GOG 244 – The lymphedema and gynecologic cancer (LEG) study: Incidence and risk factors in newly diagnosed patients. Gynecol Oncol. 2020;156(2):467-474.
- Corr B, Cosgrove C, Spinosa D, et al. Endometrial cancer: molecular classification and future treatments. BMJ Medicine. 2022;1:e00152.
- RAINBO Research Consortium. Refining adjuvant treatment in endometrial cancer based on molecular features: the RAINBO clinical trial program. Int J Gynecol Cancer. 2022;33(1):109–17.
- Roh HJ, Yoon HJ, Jeong DH, Lee TH, Kwon BS, Suh DS, Kim KH. Prognostic factors of oncologic outcomes after fertility-preservative management with progestin in early-stage of endometrial cancer. J Res Med Sci. 2021;26:48.
- Makker V, MacKay H, Ray-Coquard I, Levine DA, Westin SN, Aoki D, Oaknin A. Endometrial cancer. Nat Rev Dis Primers. 2021;7(1):88.
- Singh N, Jamieson A, Morrison J, Taylor A, Ganesan R. BAGP POLE NGS testing guidance, v1.2, dated 26 July 2022. https://www.thebagp.org/wp-content/uploads/download-manager-files/BAGP-POLE-testing-in-Endometrial-cancer-v1.2-July-2022.pdf.

Omfalocel, scrot bifid, hipospadias şi micropenis: rezultate clinice în cazuri cu cariotip normal
Cătălina Iovoaica-Rămescu, Maria Cristina Comănescu, Roxana Cristina Drăguşin, Anca-Maria Istrate-Ofiţeru, George Lucian Zorilă, Elena-Iuliana-Anamaria Berbecaru, Iuliana-Alina Enache, Ileana Drocaş, Ştefan Ciobanu, Daniel Băluţă, Andreea Vochin, Rodica Daniela Nagy, Dominic-Gabriel Iliescu
Acest studiu îşi propune să descrie caracteristicile, monitorizarea şi managementul unei malformaţii complexe: omfalocel, hipospad...
Sarcina cicatricială după operaţia cezariană – o continuă dilemă terapeutică. Serie de cazuri şi review al literaturii
Ştefan-Gabriel Ciobanu, Iuliana-Alina Enache, Laurenţiu-Mihai Dîră, Elena-Iuliana-Anamaria Berbecaru, Cătălina Iovoaica-Rămescu, Andreea Vochin, Ionuţ-Daniel Băluţă, Anca-Maria Istrate-Ofiţeru, Rodica Nagy, Maria Cristina Comănescu, Ileana Drocaş, George Lucian Zorilă, Cristian Constantin, Roxana Cristina Drăguşin, Dominic-Gabriel Iliescu
Sarcina cicatricială după operaţie cezariană (CSP) este o tulburare iatrogenă care pune viaţa în pericol, cu o incidenţă tot mai m...
Managementul histeroscopic al subfertilităţii în cazurile cu suspiciune de polipi endometriali
Iuliana-Alina Enache, Ştefan Ciobanu, Elena-Iuliana-Anamaria Berbecaru, Cătălina Iovoaica-Rămescu, Anca-Maria Istrate-Ofiţeru, Rodica Daniela Nagy, Maria Cristina Comănescu, Ileana Drocaş, George Lucian Zorilă, Roxana Cristina Drăguşin, Laurenţiu-Mihai Dîră, Dominic-Gabriel Iliescu
Polipii endometriali reprezintă o afecţiune ginecologică benignă asociată cu sângerări uterine anormale, infertilitate şi pierderi...
Care este rolul histerectomiei în tratamentul prolapsului organelor pelviene?
Ioana Cristina Rotar, Corina Costea, Adelina Staicu, Dan Boitor, Mihai Surcel, Iulian Goidescu, Georgiana Nemeti, Daniel Mureşan
Prolapsul organelor pelviene (POP) este o afecţiune cu o rată de incidenţă în creştere, afectând mai mult de 40% din femeile de peste 50 de ani. Există trei niveluri de susţinere a planşeului pelvian,...
Fibroamele uterine asociate sarcinii – este fezabilă miomectomia în sarcină? Review şi prezentare de caz
George Lucian Zorilă, Elena-Iuliana-Anamaria Berbecaru, Anca-Maria Istrate-Ofiţeru, Iuliana-Alina Enache, Ileana Drocaş, Maria Cristina Comănescu, Ştefan-Gabriel Ciobanu, Daniel Băluţă, Cătălina Iovoaica-Rămescu, Andreea Vochin, Rodica Daniela Nagy, Gabriel Dominic Iliescu
Mioamele uterine afectează 2-10% dintre femeile însărcinate. Sunt tumori dependente hormonal şi, în consecinţă, 30% dintre ele vor...