Operative vaginal delivery enables or expedites vaginal delivery by using forceps or vacuum extractor. The prevalence of this type of delivery decreased over time worldwide, because of the concerns regarding the associated risks for both mother and fetus. Although in many services forceps and vacuum delivery are less used, the Filantropia Clinical Hospital of Obstetrics and Gynecology, Bucharest, Romania, maintains good rates of operative vaginal delivery. We evaluated retrospectively the prevalence of operative vaginal delivery over the last 15 years (2003-2007 and 2015-2018) in the Filantropia Clinical Hospital. A total of 25,695 births were assessed. Forceps use has decreased over time from 2.2% in 2003 to 1.2% in 2018, while vacuum delivery increased significantly in prevalence to 3.5% in 2018. Although operative vaginal delivery was often perceived as risky for fetus, the Apgar score at 1 and 5 minutes did not show any significant differences when compared to fetal outcome after spontaneous vaginal delivery. In the Filantropia Clinical Hospital, the profile of operative vaginal delivery changed by increasing the use of vacuum extractor and proportionally decreasing the use of forceps. Concluding, the operative vaginal delivery has its place in modern obstetrics and should be used as a safe alternative to caesarean section in the second stage of labor. Although its prevalence is decreasing, efforts for the training of residents by dedicated mentors should continue as part of obstetrics curricula.
Naşterea vaginală operatorie în Spitalul Clinic Filantropia. Analiză retrospectivă a ultimilor 15 ani
Operative vaginal delivery in the Filantropia Clinical Hospital. A retrospective analysis of the last 15 years
First published: 23 octombrie 2020
Editorial Group: MEDICHUB MEDIA
DOI: 10.26416/ObsGin.68.3.2020.4013
Abstract
Rezumat
Naşterea vaginală operatorie permite sau accelerează naşterea vaginală prin utilizarea forcepsului sau a vid-extractorului. Prevalenţa acestui tip de naştere a scăzut în timp la nivel mondial, din cauza preocupărilor cu privire la reducerea riscurilor la naştere pentru mamă şi făt. Deşi în multe servicii forcepsul şi vid-extractorul sunt mai puţin utilizate, Spitalul Clinic de Obstetrică-Ginecologie Filantropia, Bucureşti, România, menţine o frecvenţă bună a naşterilor operatorii. Am evaluat retrospectiv prevalenţa naşterii vaginale operatorii în ultimii 15 ani (2003-2007 şi 2015-2018), în Spitalul Filantropia. Au fost evaluate 25.695 de naşteri. Utilizarea forcepsului a scăzut în timp de la 2,2% în 2003 la 1,2% în 2018, în timp ce naşterea cu ajutorul vid-extractorului a crescut semnificativ ca prevalenţă, la 3,5% în 2018. Deşi deseori percepute ca metode riscante pentru făt, scorul Apgar la 1 şi 5 minute al nou-născuţilor proveniţi din naşterile vaginale operatorii nu a prezentat diferenţe semnificative în comparaţie cu scorul obţinut după naşterea vaginală spontană. În Spitalul Filantropia, profilul naşterii vaginale operatorii s-a schimbat prin creşterea utilizării vid-extractorului şi scăderea proporţională a utilizării forcepsului. Aşadar, naşterea vaginală operatorie îşi menţine importanţa în obstetrica modernă şi trebuie utilizată în continuare ca o alternativă sigură la naşterea prin operaţie cezariană, în periodul doi al naşterii. Deşi prevalenţa sa scade, efortul de formare a rezidenţilor de către mentori dedicaţi ar trebui continuat ca parte a programului de rezidenţiat în obstetrică-ginecologie.
Background
Operative vaginal delivery comprises vaginal birth with the aid of vacuum or forceps. With current increasing rates of caesarean section, operative vaginal delivery use decreased mainly due to increased concerns about fetal and maternal safety, fear of litigation and malpractice and, last but not least, loss of medical training. Forceps enables and expedites vaginal delivery by applying direct traction on fetal head, while ventouse applies traction on fetal scalp.
Vacuum extractor has a much recent history(1). The appropriate use of vacuum extractor delivery was perfected years after, when evidence-based guidelines limited the use of vacuum delivery to similar prerequisite conditions as for forceps(2). Various design of the vacuum instrument and traction system have been developed over time(3); one of the successful designs is the Kiwi Omnicup® (2001), used worldwide on a large basis, including in our unit(4). The global trends of operative vaginal delivery use show overall a steady decrease in USA from 7.2% in 2005 to 5% in 2013 (5.8% vacuum and 1.4% forceps in 2005 to 4.1% vacuum and 0.9% forceps in 2013)(5). In an US epidemiological study from 2017, the rate of operative vaginal delivery was estimated at 3% of all deliveries(6). The rate of operative vaginal delivery in UK showed stable rates of 10-13% of all deliveries, with good outcomes. The operative vaginal delivery rate in Scotland in 2017 was 9.1% for vacuum delivery and 2.8% for forceps delivery(7,8).
The increased potential morbidity for both mother and child associated with the use of forceps is well known. The use of forceps should be accompanied by increased awareness and operator experience; with careful practice, the complications rates appear to be low(9).
Materials and method
We underwent a retrospective analysis evaluating over 20,000 deliveries from the Filantropia Clinical Hospital of Obstetrics and Gynecology, Bucharest, Romania, over two intervals of time, namely 2003-2007 and 2015-2018 (17,047 live deliveries). The following data were collected from the Filantropia Hospital birth registries: date of delivery, maternal age, parity, gestational age, mode of delivery, type of instrument used, mode of delivery indication, fetal birth weight, Apgar score at 1 and at 5 minutes, episiotomy rates.
Vacuum deliveries were accomplished using hand held, silicone cup Kiwi (OmniCup instruments®), while the type of forceps used varied depending on the obstetrician’s choice and experience: with parallel branches (Lazarevici, Suzor, Thierry spatulas) or crossing branches (Tarnier, Naegele).
Before starting the operative vaginal delivery procedure, the prerequisite conditions were fulfilled: the cervix was fully dilated, membranes ruptured, fetal head engaged, adequate maternal pelvis, certain fetal head position, adequate anesthesia and empty maternal bladder. On admission patients were informed – and consented – about a possible rare event of operative vaginal delivery which may occur as an obstetric emergency.
Vacuum delivery was performed for engaged presentation, most frequently at station +2 or lower. Forceps delivery was usually outlet and low-forceps, and in a minority of cases mid-cavity forceps. High forceps has been excluded from our medical practice because of the high rate of complications, according to national and international guidelines.
Results
The total number of births increased overall in the Filantropia Clinical Hospital from 2,044 in 2003 to 2,250 in 2007, and from 3,599 in 2015 to 5,162 in 2018.
The total number of deliveries was 8,648 between 2003 and 2007, and 17,047 between 2015 and 2018.
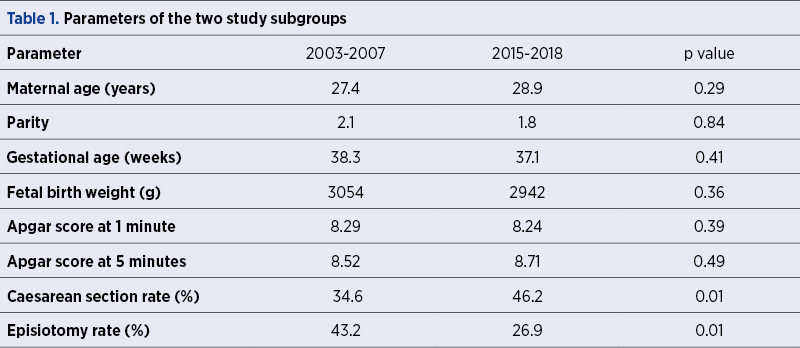
For the 2003-2007 subgroup, the average maternal age at birth was 27.4 years old and the average gestational age was 38.3 weeks, while for the 2015-2018 subgroup, the average maternal age at birth was 28.9 years old and the average gestational age was 37.1 weeks. There were no significant differences between the demographic subgroup characteristics for the two time periods, excepting caesarean section rate that increased over time and episiotomy rate in the vaginal birth subgroup, which decreased significantly over time (Table 1).
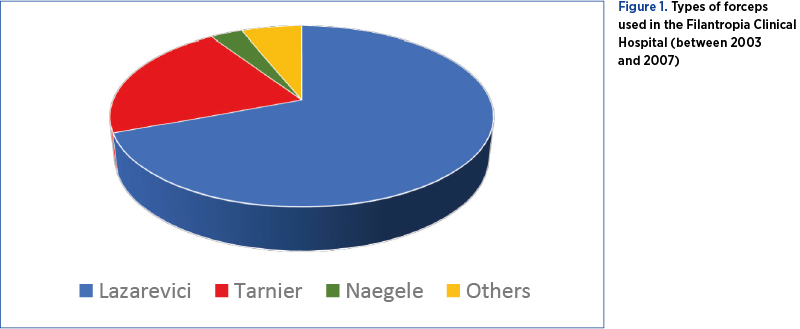
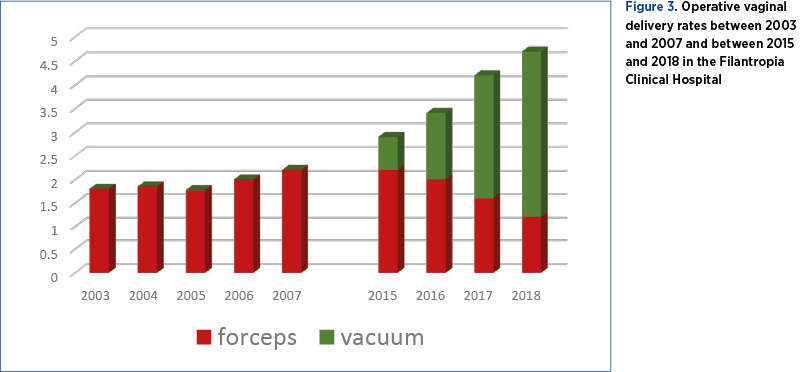
During the first interval analyzed (2003-2007), vacuum delivery was not practised in the Filantropia Clinical Hospital. A continuous increase in caesarean section rate was observed between 2003 and 2007, from 31.6% to 38%, respectively. The operative vaginal delivery during the aforementioned period consisted in forceps delivery, with a rate of 1.8% in 2003 up to 2.2% in 2007. The type of forceps used varied depending on the preference of the obstetrician. Most often, Lazarevici forceps was used, mainly for outlet and low types of delivery (Figure 1)(10).
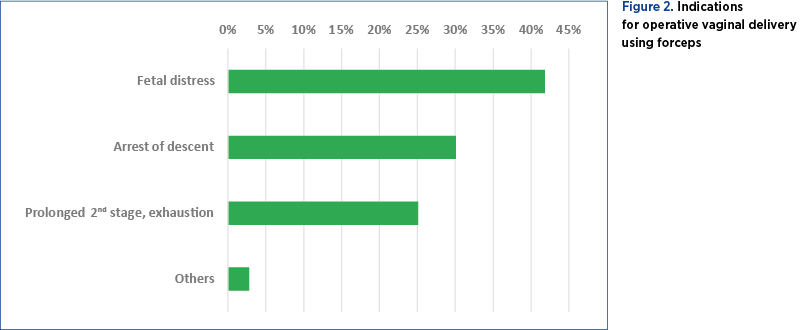
The most frequent indications for operative vaginal deliveries, between 2003 and 2007, were fetal distress (41.8%), arrest of descent (30.1%), prolonged second stage and maternal exhaustion (25.1%) – Figure 2.
For the caesarean section subgroup, the most frequent indications were: fetal distress (54.4%), previous caesarean section (18.1%), pregnancy-induced hypertension and preeclampsia (9.8%), failure of induction of labor (7.8%), breech presentation (4.2%), low-lying placenta (2.6%), and others.
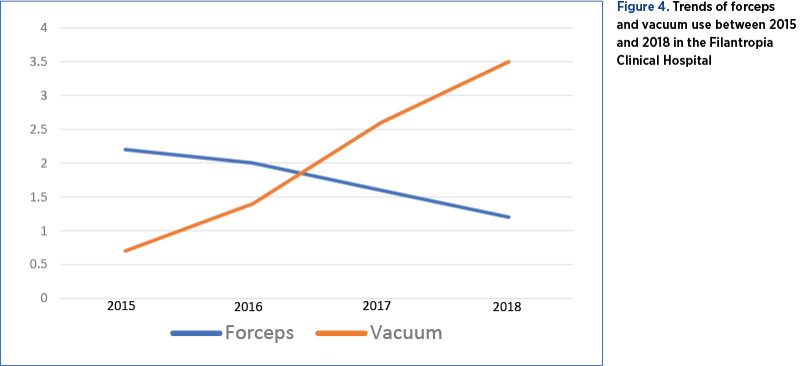
After the introduction of vacuum delivery system in the Filantropia Clinical Hospital, between 2015 and 2018 the operative vaginal delivery profile changed significantly, with a constant increase of vacuum deliveries and a decrease in the use of forceps. Vacuum delivery system use increased from 0.7% in 2015 up to 3.5% in 2018, while forceps was less used (2.2% in 2015 versus 1.2% in 2018). Overall, the operative vaginal delivery rate increased, mainly due to vacuum use, from 2.9% in 2015 to 4.7% in 2018. However, caesarean section rate followed a rising trend over the years, despite increasing rates of operative vaginal delivery (45.8% in 2015, and remained stable at 45.6% in 2018).
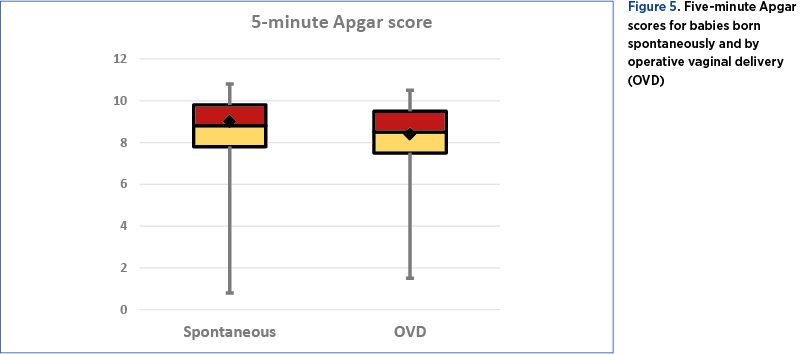
For the immediate outcome of spontaneous and operative vaginal deliveries evaluation, Apgar scores at 1 and at 5 minutes were compared. There were no significant differences regarding Apgar scores between spontaneous delivery and operative vaginal delivery (average 5-minute Apgar score 8.66 versus 8.07, respectively; p>0.05) – Figure 5. The Apgar scores were similar between forceps group and vacuum group as well (8.07 versus 8.44 respectively; p>0.05). The caesarean section born babies had an average Apgar score of 8.55.
Discussion
The rate of operative vaginal delivery in Romania is rapidly declining, following the worldwide trends. Fear for the safety of mother and baby and of litigation, and the significant decrease in training and training opportunities have led operative vaginal delivery to become an art about to be forgotten. There are currently very scarce publications that evaluate the institutional experience about operative vaginal delivery in our country. One of the few papers on the subject is a retrospective study by Tîrnovanu et al., analyzing data between 2009 and 2015 from one of the largest maternity in Romania. According to the authors, forceps delivery was replaced by vacuum, and the rate of operative vaginal delivery using vacuum delivery was estimated at 0.7%. The indications were prolonged second stage, fetal distress and, less frequently, shortening of the second stage of labor, with low maternal and fetal complication rates(11). Data regarding operative vaginal delivery from our institution were published by Botezatu et al. in 2015, citing rates of 3% of all deliveries between 2012 and 2015, of which 2% were forceps deliveries and 1% were vacuum deliveries(12). As already mentioned, the forceps use decreased in our unit over time, while vacuum delivery rate increased, mainly probably due to the perception of obstetricians of increased safety with vacuum delivery for both mother and fetus when compared to forceps.
A national survey in Germany on the experience and self-reported competency regarding operative vaginal delivery, assessing over 600 obstetricians, reported significant lower rates of self-perceived experience and confidence with forceps deliveries when compared with vacuum-assisted vaginal deliveries. When physicians were asked to choose between forceps and vacuum extractor for a case with indication for any of the two methods, most of them (92%) chose vacuum delivery, irrespective of professional level, the level of training or the volume of deliveries performed(13).
The worldwide trends are similar, with a significant decrease of rate of forceps and vacuum deliveries. A large US study that assessed over 22,000,000 of vaginal deliveries from US birth records, between 2005 and 2013, revealed a decreasing vacuum and forceps use, with rates around 4-5% for vacuum use and 0.9-1.4% for forceps use(5), while in the UK there were reported rates of 10-11%(14). The operative vaginal delivery is less used in low- and middle-income countries as well. A population-based study that evaluated over 350,000 deliveries between 2010 and 2016 reported a decrease of the rate of operative vaginal delivery from 1.6% to 0.3%, while caesarean section rates increased from 6.4% to 14.4%(15).
Conclusions
The operative vaginal delivery is indicated for both maternal and fetal reasons. Despite notable progress in obstetrics and labor management, the operative vaginal delivery still represents an important part of the modern management of labor. The use of obstetric forceps and vacuum extractor must be part of the obstetric curricula, taught by dedicated mentors and trained under supervision. Practicing operative vaginal delivery, using forceps or vacuum extractor, requires being familiar with these instruments, using them responsibly and professionally, knowing the indications and risks.
The operative vaginal delivery maintained a slightly increasing rate in our unit, mainly due to the increasing use of vacuum extractor, while the incidence of forceps decreased over time. While during the first interval analyzed (2003-2007) forceps was the only alternative for operative vaginal delivery, counting for about 2% of all deliveries, after 2015 vacuum-assisted delivery increased constantly, being perceived as a safer method by the obstetricians and pregnant women as well. In 2018, forceps delivery was performed in 1.2% of the total number of deliveries, while vacuum-assisted delivery accounted for 4.7% of all deliveries.
The Filantropia Clinical Hospital continues to practise operative vaginal delivery as an effort to offer complete medical services to its patients and preserve and transmit the art of operative vaginal delivery through the residency program. The best care of our patients and the best training opportunities for obstetrics and gynecology residents have always been our priorities. However, the less and less use of forceps should stimulate senior obstetricians to continue using it for appropriate indications and to spread the art of forceps use to younger colleagues. The standardized training with focus on operative vaginal delivery techniques, mainly forceps delivery, is recommended and should be prioritized. Training through medical simulation in operative vaginal delivery is an important step to keep this art about to be forgotten.
Bibliografie
-
1. Malmstrom T. The Vacuum Extractor an Obstetrical Instrument and the Parturiometer a Tokographic Device. Acta Obst Gynec Scandinav. 1957;36(S3):5-87.
-
2. Vacca A. Reducing the Risks of a Vacuum Delivery. Fetal and Maternal Medicine Review. 2007;17(04):301-315.
-
3. Andrewartha K, Wilkinson C. The evolution of the obstetric vacuum extractor. O&G Magazine. Tools of the trade. 2015;17(4):71-3.
-
4. Vacca A. Operative vaginal delivery: clinical appraisal of a new vacuum extraction device. ANZJOG. 2001;41(2):156-60.
-
5. Merriam AA, Ananth CV, Wright JD, Siddiq Z, D’Alton ME, Friedman AM. Trends in operative vaginal delivery, 2005-2013: a population-based study. BJOG. 2017;124(9):1365-1372.
-
6. Martin JA, Hamilton BE, Osterman MJK, Driscoll AK, Drake P. Births: Final Data for 2017. Natl Vital Stat Rep. 2018;67(8):1-50.
-
7. Royal College of Obstetricians and Gynaecologists Clinical Effectiveness Support Unit. National Sentinel Caesarean Section Audit Report. London: RCOG Press; 2001. Available at http://www.rcog.org.uk/files/rcog-corp/uploaded- files/nscs_audit.pdf.
-
8. Information and Statistics Division, Scottish Health Statistics. Births in Scottish Hospitals; Year ending 31 March 2017; Publication date – 28 November 2017. Available at: https://www.isdscotland.org/Health-Topics/Maternity-and-Births/Publications/2017-11-28/2017-11-28-Births-Report.pdf
-
9. Demissie K, Rhoads GG, Smulian JC, Balasubramanian BA, Gandhi K, Joseph KS, et al. Operative vaginal delivery and neonatal and infant adverse outcomes: population based retrospective analysis. BMJ. 2004 Jul 3;329(7456):24–9.
-
10. ACOG Practice Bulletin No. 154: Operative vaginal delivery. Obstet Gynecol. 2015 Nov;126(5):e56-65.
-
11. Tîrnovanu MC, Nemescu D, Mătrescu AC, Cozoreanu AM, Cara A, Pasat S, Tîrnovanu SD, Onofriescu M. The vacuum extractor delivery. Our experience. Ginecologia.ro. 2015;3(10):10-12.
-
12. Botezatu R, Dobre T, Dumitrasi L, Peltecu G. Operative vaginal delivery in modern era. Ginecologia.ro. 2015;3(7):23-28 (Supplement).
-
13. Hamza A, Lavin JP, Radosa JC, et al. Vaginal operative delivery in Germany: a national survey about experience and self-reported competency.
-
J Matern Fetal Neonatal Med. 2020 Apr 20;1-7.
-
14. Department of Health. Maternity matters: choice, access, and continuity of care in a safe service. London: HMSO, 2007.
-
15. Harrison MS, Saleem S, Ali S, Pasha O, Chomba E, Carlo WA, et al. A Prospective, Population-Based Study of Trends in Operative Vaginal Delivery Compared to Cesarean Delivery Rates in Low- and Middle-Income Countries, 2010-2016. Am J Perinatol. 2019 Jun;36(7):730-736.