Over the last two decades, obesity and overweight have increased significantly, becoming public health problems worldwide. Data from literature show a continuous increase in the prevalence of the two entities, which results in an increasing number of overweight or obese patients who reach the reproductive age and become pregnant. Pregnancies in obese or overweight patient are the new challenges that obstetricians have to face. This review is based on publications that were found on PubMed, with a special attention to the review articles, cohort studies and randomized trials. Obesity and overweight can affect both getting and maintaining a pregnancy. The chances of obtaining a pregnancy decrease linearly by 4% for every 1 kg/m² gained, starting from a Body Mass Index (BMI) of 29 kg/m². The prevalence of fetal malformations is also increased in overweight or obese patients, the risk raising proportionally with the severity of obesity. These endemic diseases are also associated with certain maternal complications. A 10% increase in weight during pregnancy compared to pregestational BMI has been shown to be a factor that increases the risk by about 10% for the occurrence of hypertension and gestational diabetes, respectively. Newborns are also affected by these pathologies. Newborns in obese mothers have an increased percentage of adipose tissue, and studies have shown that there is an association between maternal adiposity and fetal weight at birth. The interventions in lifestyle and nutrition during pregnancy did not have an important effect on reducing the incidence of maternal and fetal complications. Therapeutic strategies are needed for normalizing body weight before pregnancy because reducing BMI has benefits for both mother and fetus.
Obezitatea şi sarcina
Obesity and pregnancy
First published: 24 mai 2022
Editorial Group: MEDICHUB MEDIA
DOI: 10.26416/ObsGin.70.1.2022.6510
Abstract
Rezumat
În ultimele două decenii, obezitatea şi supraponderea au crescut semnificativ, devenind probleme de sănătate publică la nivel mondial. Datele din literatură arată o creştere continuă a prevalenţei celor două entităţi, ceea ce are ca rezultat un număr tot mai mare de paciente supraponderale sau obeze care ajung la vârsta reproductivă şi rămân însărcinate. Sarcinile la pacientele obeze sau supraponderale sunt noile provocări cu care se confruntă obstetricienii. Acest articol este bazat pe publicaţiile care au fost identificate în baza de date PubMed, acordând o atenţie deosebită articolelor de tip recenzie, studiilor de cohortă şi studiilor randomizate. Obezitatea şi supraponderea pot afecta atât obţinerea, cât şi menţinerea unei sarcini. Şansele de a obţine o sarcină scad liniar cu 4% pentru fiecare 1 kg/m² dobândit, pornind de la un IMC (indice de masă corporală) de 29 kg/m². Prevalenţa malformaţiilor fetale este crescută la pacientele supraponderale sau obeze, riscul crescând proporţional cu severitatea obezităţii. Aceste boli endemice sunt, de asemenea, asociate cu anumite complicaţii materne. O creştere a greutăţii cu 10% în timpul sarcinii în comparaţie cu IMC-ul pregestaţional s-a dovedit a fi un factor care creşte riscul cu aproximativ 10% pentru apariţia hipertensiunii şi, respectiv, a diabetului gestaţional. Nou-născuţii sunt şi ei afectaţi de aceste patologii. Nou-născuţii mamelor obeze au un procentaj crescut al ţesutului adipos, iar studiile au arătat că există o asociere între adipozitatea maternă şi greutatea fetală la naştere. Intervenţiile în stilul de viaţă şi alimentaţie în timpul sarcinii nu au avut un efect important asupra reducerii incidenţei complicaţiilor materne şi fetale. Sunt necesare strategii terapeutice pentru normalizarea greutăţii corporale înainte de sarcină, deoarece reducerea IMC are beneficii atât pentru mamă, cât şi pentru făt.
Introduction
Obesity and overweight are not newly discovered phenomena; in the last two decades, they had a significant increase in incidence, becoming common worldwide health problems.
Obesity and overweight are endemic diseases of the 21st century, being more frequently discovered among young people. Data from the literature show a continuous increase in the prevalence of the two entities, which result in an increasing number of overweight or obese patients who reach the reproductive age and become pregnant. Statistics show that 50% of patients of reproductive age are overweight or obese, 18% of whom are obese at the beginning of pregnancy(1).
It is well known that obesity and overweight can affect both fertility and pregnancy. Both entities may contribute to pregnancy-related pathologies such as pregnancy-induced hypertension, preeclampsia or gestational diabetes. The association between these conditions is a risk factor for maternal and neonatal adverse outcomes, such as post-term pregnancies with the need of induced labor, fetal macrosomia, fetal intrauterine demise, increased duration of labor and its slow progression (often resulting in termination of labor through caesarean section). These issues are often real challenges that obstetricians have to face(1,2,4,9).
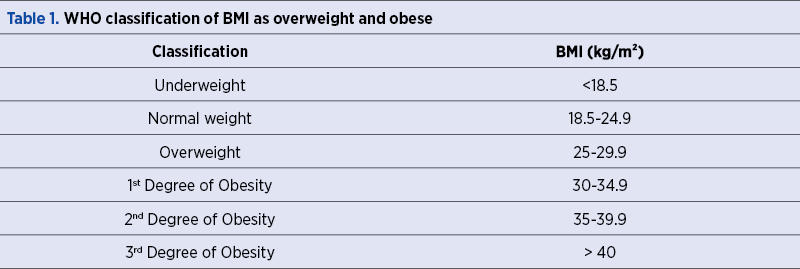
The classification of overweight and obesity is based on the Body Mass Index (BMI), calculated by dividing the weight (kg) by the square of the height (m). Thus, the following classes are distinguished: underweight, normal weight, overweight and obesity (which is also classified into three degrees) – Table 1.
Adipose tissue has many cells in its composition, including adipocytes, macrophages and fibroblasts. The main function of adipocytes, also known as fat cells, is the storage of triglycerides (the basic form under which the body stores fatty acids). Aside from storing fatty acids, adipocytes also produce substances (adipokines) involved in energy metabolism, heart contractility, angiogenesis, carbohydrate metabolism, insulin secretion, and so on. Adipose tissue is considered a large endocrine organ(10,11).
Materials and method
A selective search was conducted in the PubMed database using the following search terms: “pregnancy”, “obesity”, “maternal” and “fetal”, “pregnancy complications”. We found a number of 927 studies in the last 15 years.
We gave a special attention to the cohort studies, randomized controlled trials and systematic reviews. Relevant older papers identified in references or by targeted keyword search were also included.
Results
Obesity can affect both getting pregnant and maintaining a pregnancy through hyperinsulinemia followed by hyperandrogenemia. These phenomena are associated with the occurrence of anovulatory cycles and, thus, the time of obtaining a pregnancy has been shown to be longer in patients with high BMI compared to the ones with normal weight(1,2,4). However, the decrease in fertility associated with obesity cannot be attributed only to anovulatory and irregular menstrual cycles(4,12). A study of a group of 3029 obese patients with regular menstruation (after excluding fallopian pathologies and androgenic abnormalities) showed that, during one year, 17% of the subjects included in the study spontaneously obtained a pregnancy that did not end by miscarriage(12). It has been shown that the probability of conception decreases linearly by 4% for every 1 kg/m² gained, starting from a BMI of 29 kg/m²(1,4,5,12).
Obese patients have a higher risk of spontaneous pregnancy loss compared to normal weight patients. The risk of recurrent miscarriage is also increased. The causes that lead to a higher rate of pregnancy loss in obese patients are not fully known. Obesity seems to affect the quality of oocytes, but nevertheless obese patients have a higher risk of pregnancy loss even in the case of a pregnancy obtained through donated oocytes. Overweight and obesity affect the endometrium and its receptivity, phenomena that may be the cause of higher rates of miscarriage(4,7).
Overweight and obesity are also associated with certain maternal complications. The risks of pregnancy-related pathologies increase proportionally with the severity of obesity. Among the most common pathologies that can affect obese patients are: gestational diabetes, pregnancy-associated hypertension, preeclampsia, eclampsia, thromboembolic events, respiratory complications, and so on. A 10% increase in weight during pregnancy compared to pregestational BMI has also been shown to be a factor that increases the risk for occurrence of hypertension and gestational diabetes by about 10%(4,7,8,13).
Obesity also has repercussions on the embryo and its development. The prevalence of fetal malformations is significantly higher in overweight or obese patients, the increase in this risk being proportional to the severity of obesity(4,8) – Table 2.
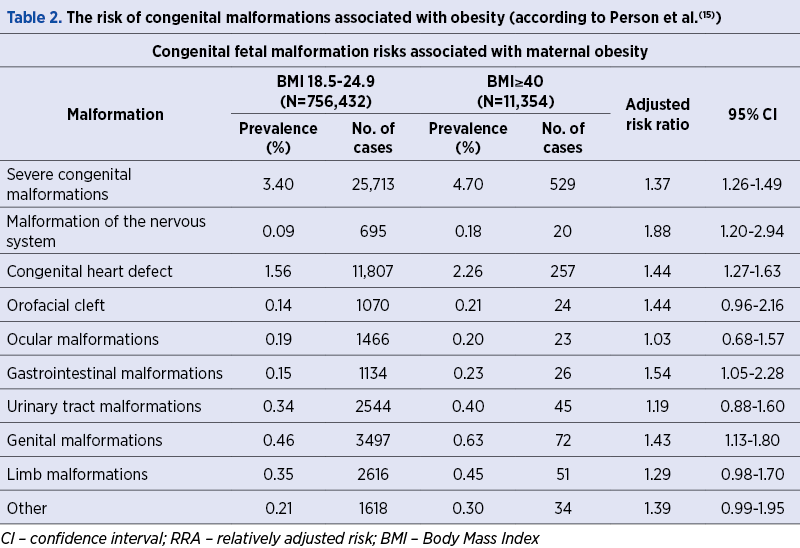
A meta-analysis (which included 18 studies) reported specific malformations associated with obesity. These are: spina bifida, septal heart defects, anorectal atresia, hydrocephalus and eye abnormalities. Regarding gastroschisis, obesity has been shown to have a protective effect(4,9,14).
Another important risk associated with an increased Body Mass Index is fetal intrauterine death. The literature shows a 0.4% risk of intrauterine fetal death in patients with a BMI of 20 kg/m2 and 0.59% in patients with a BMI greater than 30 kg/m2. Intrauterine fetal death is most often due to the association of several factors, such as impaired placental function, high blood pressure, and so on(4,6).
Obesity and overweight during pregnancy are independent risk factors for the appearance of large for gestational age fetuses, as well as for the macrosome fetuses. Newborns from obese mothers have an increased percentage of adipose tissue, and studies have shown that there is an association between maternal adiposity and fetal weight at birth(4). The percentage of macrosomic fetuses increases with increasing maternal BMI. A study that included 112,309 births showed a percentage of 17% macrosomic fetuses in patients with BMI ≥40 kg/m2 compared to only 8% in patients with normal BMI(16). The pathogenesis of fetal macrosomia is a complex one. Increased levels of maternal blood glucose are involved in obesity-induced insulin resistance. Also, the growth of fetal adipose tissue can be explained by the existence of an increased availability of metabolic substrates(3,4,9).
Obese and overweight patients have an increased risk of labor abnormalities and birth complications. The data found in the literature show a lower rate of spontaneous onset of labor in this category of patients compared to the ones with normal weight and, as a consequence, an increased risk of post-term pregnancies and an increase in the incidence of birth through caesarean section. Maternal weight gain is associated with an increased risk of caesarean delivery. For every additional 1 kg/m2 in BMI, the risk of caesarean delivery increases by 4%(4,5,7). Another reason for an increased rate of caesarean births in obese and overweight patients is represented by pathologies that complicate the normal course of pregnancy, such as preeclampsia, gestational diabetes, fetal heart abnormalities, cephalopelvic disproportion and the lack of labor progression(7). Obesity and overweight also lead to difficult wound healing and wound infections. A large study on 11,752 obese patients showed that they had lower rates of spontaneous onset of labor after 37 weeks of gestation(17). The chances of spontaneous onset of labor decrease proportionally with the increase in BMI(4,7,8,17).
The reason for the occurrence of post-term pregnancies in obese patients is not fully understood, but it is assumed that metabolic and endocrine dysfunctions involving the onset of labor are involved(4,5,7,10). In this category of patients, higher concentrations of estrogen in adipose tissue are detected, which can disturb the hormonal balance and which can induce a dysfunction of the mechanisms involved in the regulation of labor(7,13). Obese and overweight patients are more likely to experience a labor induction compared to normal-weight patients, but the risk of failure of this procedure is higher in overweight patients(5,7). A large, retrospective study on 80,887 patients who underwent the induction of labor showed that 13% of normal-weight patients had a failed induction, while the failure rate was more than twice as high (29%) for those with a BMI greater than or equal to 40 kg/m2(18).
Among the theories that try to explain the mechanisms through which maternal obesity is associated with the lack of onset of labor and with labor abnormalities is the one that involves affecting the uterine contractility in this group of patients. Uterine contractility is lower in these patients, even after oxytocin stimulation. Biopsies taken from the myometrium showed a lower expression of calcium channels and also reduced signals between them in patients with high BMI and diabetes. There are also differences between myometrial masses in normal and obese patients(7,8,11).
Obesity and overweight involve both maternal and fetal risks that reach their peak during labor and delivery. These maternal risks include emergency caesarean delivery, premature detachment of the normally inserted placenta, grade III/IV perineal ruptures, fever and puerperal infections, difficult wound healing, anesthetic complications, significant postpartum hemorrhage, sepsis, thromboembolism and venous thrombosis(4,7).
Various methods for reducing BMI of this group of patients have been studied. Lifestyle interventions include dietary changes and increased levels of physical activity. In the case of women who want children, these lifestyle changes will result in ovulation and in an increased rate of spontaneous conception(7,15). Lifestyle interventions can result in a 10% to 15% reduction in body weight over the course of a year. A weight loss of 30% to 40% is often achieved in the first year after bariatric surgery(4,7). The largest published case-control study evaluating the effect of bariatric surgery found a significant reduction in the prevalence of gestational diabetes and fetal macrosomia, as well as an increased risk of fetal hypotrophy(19). Other studies on the effect of bariatric surgery on the progress of pregnancy have shown an increased risk of premature birth after 32 weeks of gestation(4,7,15).
Weight loss during pregnancy is associated with an increased risk of low birth weight. For this reason, weight reduction during pregnancy is not recommended(4,7,9). Weight loss between two pregnancies has a positive effect on neonatal outcomes and on pregnancy progression(20).
Conclusions
The increase in maternal and fetal morbidity during pregnancy in relation to obesity is well documented in studies. Obesity is an independent risk factor for maternal comorbidities such as diabetes and pregnancy hypertension. The same risks exist in excess of weight gain during pregnancy. Also, obesity has a negative impact on the fetal development, increasing the risk for fetal anomalies or excessive fetal growth. Therapeutic strategies that have been developed appear to work in compliant patients who adhere to lifestyle changes prior to pregnancy(4,7).
Normalizing body weight before pregnancy has benefits for both mother and fetus. Reduction of maternal and fetal morbidity and mortality can be achieved through lifestyle changes and dietary changes maintained not only during pregnancy but also outside it(4). Nonetheless, guidelines for the management of pregnancy in obese patients are also needed to reduce complications and help obstetricians in the management of this category of patients and to prevent complications that may occur during pregnancy, delivery or in the postpartum period.
Conflict of interests: The authors declare no conflict of interests.
Bibliografie
-
Thangaratinam S, Rogozińska E, Jolly K, Glinkowski S, Duda W, Borowiack E, et al. Interventions to reduce or prevent obesity in pregnant women: A systematic review. Health Technol Assess (Rockv). 2012;16 (31):1–191.
-
Bazzano MV, Sarrible GB, Martinez N, Berón de Astrada M, Elia EM. Obesity alters the uterine environment before pregnancy. J Nutr Biochem. 2018;62:181–91.
-
Grieger JA, Hutchesson MJ, Cooray SD, Bahri Khomami M, Zaman S, Segan L, et al. A review of maternal overweight and obesity and its impact on cardiometabolic outcomes during pregnancy and postpartum. Ther Adv Reprod Heal. 2021;15: 263349412098654.
-
Stubert J, Reister F, Hartmann S, Janni W. Risiken bei Adipositas in der Schwangerschaft. Dtsch Arztebl Int. 2018;115(16):276–83.
-
Heslehurst N, Scallop R, Hayes L, Crowe L, Jones D, Robalino S, et al. Maternal body mass index and post-term birth: a systematic review and meta-analysis. Obes Rev. 2017;18 (3):293–308.
-
Edwards P, Wright G. Obesity in pregnancy. Obstet Gynaecol Reprod Med. 2020;30(10):315–20.
-
Dolin CD, Kominiarek MA. Pregnancy in Women with Obesity. Obstet Gynecol Clin North Am. 2018; 45(2):217–32.
-
Ramachenderan J, Bradford J, McLean M. Maternal obesity and pregnancy complications: A review. Aust New Zeal J Obstet Gynaecol. 2008;48(3):228–35.
-
Marchi J, Berg M, Dencker A, Olander EK, Begley C. Risks associated with obesity in pregnancy, for the mother and baby: A systematic review of reviews. Obes Rev. 2015;16(8):621–38.
-
Azaïs H, Leroy A, Ghesquiere L, Deruelle P, Hanssens S. Effects of adipokines and obesity on uterine contractility. Cytokine and Growth Factor Reviews. 2017;34: 59–66.
-
Alsaif S, Mumtaz S, Wray S. A short review of adipokines, smooth muscle and uterine contractility. Life Sci. 2015 Mar 15;125: 2–8.
-
van der Steeg JW, Steures P, Eijkemans MJ, et al. Obesity affects spontaneous pregnancy chances in subfertile, ovulatory women. Hum Reprod. 2008;23:324–8.
-
Schummers L, Hutcheon JA, Bodnar LM, Lieberman E, Himes KP. Risk of adverse pregnancy outcomes by prepregnancy body mass index: a population-based study to inform prepregnancy weight loss counseling. Obstet Gynecol. 2015;125:133–43.
-
Stothard KJ, Tennant PW, Bell R, Rankin J. Maternal overweight and obesity and the risk of congenital anomalies: a systematic review and meta-analysis. JAMA. 2009;301:636–50.
-
Mutsaerts MA, van Oers AM, Groen H, et al. Randomized trial of a lifestyle program in obese infertile women. N Engl J Med. 2016;374:1942–53.
-
Kim SS, Zhu Y, Grantz KL, et al. Obstetric and neonatal risks among obese women without chronic disease. Obstet Gynecol. 2016;128:104–12.
-
Frolova AI, Wang JJ, Conner SN, et al. Spontaneous labor onset and outcomes in obese women at term. Am J Perinatol. 2018; 35(1):59–64.
-
Wolfe KB, Rossi RA, Warshak CR. The effect of maternal obesity on the rate of failed induction of labor. Am J Obstet Gynecol. 2011; 205(2):128.e1-7.
-
Johansson K, Cnattingius S, Naslund I, et al. Outcomes of pregnancy after bariatric surgery. N Engl J Med. 2015;372:814–24
-
McBain RD, Dekker GA, Clifton VL, Mol BW, Grzeskowiak LE: Impact of interpregnancy BMI change on perinatal outcomes: a retrospective cohort study. Eur J Obstet Gynecol Reprod Biol. 2016;205:98–104.
Articole din ediţiile anterioare
Incidence of hereditary thrombophilia in women with history of obstetrical complications
Trombofilia este o anomalie a procesului de coagulare, care constă în starea de hipercoagulabilitate a sângelui, o afecţiune eterogenă, multifactor...
Prevenirea paraliziei cerebrale la sugarii prematuri - rolul potenţial al sulfatului de magneziu
Profilaxia deficienţei neurologice a nou-născuţilor prematuri rămâne o provocare pentru neonatologi. Administrarea medicamentelor cu efect neuropro...
COVID-19 în sarcină – dificultăţi şi progrese
The newly emerging coronavirus disease 2019 (COVID-19), caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), is spreading gl...
Cât de des recomandaţi suplimentarea cu vitamină D în sarcină? Ce trebuie să ştie obstetricienii despre vitamina D şi sarcină
Vitamina D (calciferolul), măsurată prin 1,25-dihidroxivitamina D în serul matern, este importantă pentru dezvoltarea unităţii fetoplacentare. Celu...