Aim. The validation of an artificial intelligent system (AIS) – Ankara System Version 5.0 – for the interpretation of antepartum fetal heart rate (FHR) tracings.
Methodology. This study consisted of 3100 assuring FHR tracings obtained from normal pregnancies and 467 non-assuring FHR tracings (13.09% of all cases) obtained from pregnancies with various types of maternal health risk factors and/or obstetric complications. Assuring tracings from complicated pregnancies and non-assuring tracings from normal pregnancies were not included in the study, in order to have a qualified database. All tracings were evaluated twice by a single expert. The first evaluation took place just after data acquisition and the second occurred two weeks later without knowledge of the clinical characteristics of the patient (unmatched tracing evaluations were not included in the database). A total of 3032 of them were used for the training of the algorithms, while 535 of them were used for testing and validation. A Doppler ultrasound fetal heart rate monitor with autocorrelation (Hewlett Packard, 8040A) was connected to a computer system by a special frame grabber. Ten-minute recordings were kept in a special file for pattern recognition and decision making. Wavelet transformation was used for feature extraction as the first step of pattern recognition. Unsupervised and supervised artificial neural networks (vector quantization and backpropagation learning algorithm, respectively), the second step of pattern recognition, were used as the classification steps of the hybrid AIS.
Results. The testing group consisted of 480 assuring and 55 non-assuring tracings. The sensitivity and specificity of the Ankara System (Version 5.0) were found to be 61.25% and 98.68%, respectively, while the positive predictive value and negative predictive value were calculated to be 89.1% and 93.5%, respectively.
Conclusions. This hybrid AIS (Ankara System Version 5.0) might be an effective alternative decision-making tool in the routine practice for the interpretation of FHR tracings.
Validarea unui sistem de inteligenţă artificială pentru interpretarea traseului antepartum al ritmului cardiac fetal (Ankara System Version 5.0)
Validation of an artificial intelligent system for the interpretation of antepartum fetal heart rate tracings (Ankara System Version 5.0)
First published: 20 decembrie 2021
Editorial Group: MEDICHUB MEDIA
DOI: 10.26416/ObsGin.69.4.2021.5770
Abstract
Rezumat
Aim. The validation of an artificial intelligent system (AIS) – Ankara System Version 5.0 – for the interpretation of antepartum fetal heart rate (FHR) tracings.
Methodology. This study consisted of 3100 assuring FHR tracings obtained from normal pregnancies and 467 non-assuring FHR tracings (13.09% of all cases) obtained from pregnancies with various types of maternal health risk factors and/or obstetric complications. Assuring tracings from complicated pregnancies and non-assuring tracings from normal pregnancies were not included in the study, in order to have a qualified database. All tracings were evaluated twice by a single expert. The first evaluation took place just after data acquisition and the second occurred two weeks later without knowledge of the clinical characteristics of the patient (unmatched tracing evaluations were not included in the database). A total of 3032 of them were used for the training of the algorithms, while 535 of them were used for testing and validation. A Doppler ultrasound fetal heart rate monitor with autocorrelation (Hewlett Packard, 8040A) was connected to a computer system by a special frame grabber. Ten-minute recordings were kept in a special file for pattern recognition and decision making. Wavelet transformation was used for feature extraction as the first step of pattern recognition. Unsupervised and supervised artificial neural networks (vector quantization and backpropagation learning algorithm, respectively), the second step of pattern recognition, were used as the classification steps of the hybrid AIS.
Results. The testing group consisted of 480 assuring and 55 non-assuring tracings. The sensitivity and specificity of the Ankara System (Version 5.0) were found to be 61.25% and 98.68%, respectively, while the positive predictive value and negative predictive value were calculated to be 89.1% and 93.5%, respectively.
Conclusions. This hybrid AIS (Ankara System Version 5.0) might be an effective alternative decision-making tool in the routine practice for the interpretation of FHR tracings.
Introduction
Non-stress tests (NST) are widely used for the assessment of fetal well-being, mostly after 28 gestational weeks, within the framework of perinatal surveillance programs(1,2). However, the evaluation of this test is full of subjectivities and, therefore, physicians are searching for better approaches and computerized methodologies(3-8).
Various types of computerized systems have been developed for the evaluation of antepartum fetal heart rate (FHR) tracings(3-9). However, there are some discrepancies behind NST that greatly affect its suitability for testing fetal well-being. These discrepancies include: the name of the test, phrases used for defining test results, standardization of applications (duration, timing, frequency etc.), differences in the algorithms of different “fetal monitors/transducers”, distinctions in terms of the manual evaluation of tracings, and the presence of different types of computerized systems that use different algorithms at different steps of the analysis and decision-making procedures, such as data acquisition, waveform analysis, feature extraction, classification and decision making(3-10). Furthermore, the presence of different types of decision-making models, such as knowledge-based systems, supervised or unsupervised artificial intelligent systems, and hybrid systems in various forms, are all making antepartum FHR monitoring more complex and debatable(3-9).
In this work, we have decided to present the validation results of our hybrid artificial intelligent system (version 5.0 prototype) for the interpretation of antepartum FHR tracings.
Patients/materials and method
This study consisted of 3100 assuring FHR tracings obtained from normal pregnancies and 467 non-assuring tracings (13.09% of all cases) obtained from pregnancies with various types of maternal health risk factors and/or obstetric complications. Assuring tracings from complicated pregnancies and non-assuring tracings from normal pregnancies were not included in the study, in order to maintain a qualified set of data. All tracings were evaluated twice by a single expert. The first evaluation took place just after data acquisition and the second occurred two weeks later, without knowledge of the clinical characteristics of the patient (unmatched tracing evaluations were not included in the database). A total of 3032 tracings were used for the training of the algorithms, while 535 were used for testing and validation.
Fetal heart rate tracings were collected during the antepartum period, from the 28th gestational week onwards. A Doppler ultrasound heart rate monitor with autocorrelation (Hewlett Packard 8040A) was used to detect fetal pulse. Perceived fetal movements were recorded by the patient. The fetal monitor was connected to the computer system by a special frame grabber. Ten-minute recordings were kept in a special file for pattern recognition and decision-making.
Wavelet transformation is used for waveform analysis to extract 100 features from each tracing which was the first step of pattern recognition (feature extraction)(11,12). Then, artificial neural network (ANN) was used for the classification of waveforms as the second step of pattern recognition(13-15).
Firstly, unsupervised ANN (clustering by vector quantization) (Step IIa) was used to define six clusters of tracings, using the extracted 100 features(14-16). Then, the medical expert evaluated the member tracings of each cluster in terms of presence of assuring, non-assuring and unidentified waveforms(1,10). Clusters that were dominant in terms of assuring and non-assuring tracings were selected for the next step (Step IIb). Subsequently, tracings of these clusters were reused for the second classification by a supervised ANN (back propagation learning algorithm); the tracings were classified as assuring or non-assuring FHR waveforms as a final decision(17).
This study is supported by the State Planning Organization of Turkey (Project Numbers: DPT 90K 120540 and DPT 96K 120540) and The Scientific and Technological Research Council of Turkey (TAG-595).
Results
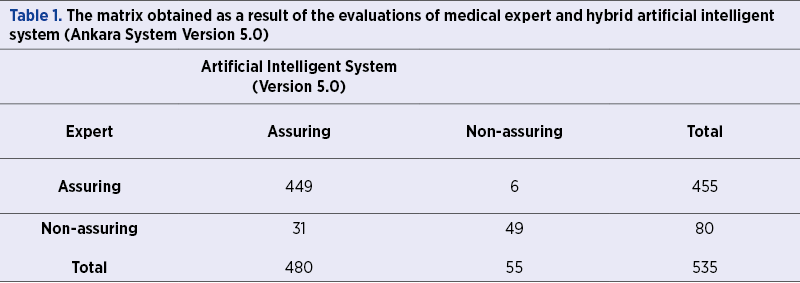
The testing group consisted of 480 assuring and 55 non-assuring tracings. Table 1 shows the matrix related to the validation and statistical measures of this version of the system. The sensitivity and specificity of Ankara System (Version 5.0) were found to be 61.25% and 98.68%, respectively. The positive and negative predictive values of the system were 89.1% and 93.5%, respectively. Table 2 shows the validation and the statistical measures of this version of hybrid ANN.

Discussion
Antepartum FHR tracing is used in different forms in perinatal surveillance, such as the use of the NST(1,2,9). However, the NST or however it is referred to (even as “antepartum FHR testing”) has some disadvantages in terms of standardization problems. The factors that make NST more complex include the variable duration of recordings, the presence of different fetal monitors with different algorithms, and autocorrelation-related differences. In classical manual and observational practice, various indices and parameters are used for the evaluation of the test; these include baseline, variability, FHR acceleration, FHR deceleration and perceived fetal movement(18-20). However, we do not know the exact biological rationales behind the condition-related changes of these variables. It might be concluded that manual interpretation of the tracing (NST) is subjective and consists of various types of heuristic approaches. The sensitivity and specificity of NST are reported to be around 50% and 98%, respectively(1,2,9).
Various computerized systems have been developed to overcome the problems inherent in manual evaluations of FHR tracings (NST)(3-8). Then, however, we face the standardization problems of these computerized systems. In our institution, we have started with rule-based automated systems and used various types of algorithms for baseline, variability and other parameters(3-5). However, a lack of sufficient information behind the condition-related changes of these parameters has directed us to develop an artificial intelligent system.
Artificial intelligence systems are widely used in different fields of medicine for a variety of purposes(21-27). In this study, we have used pattern recognition (feature extraction and classification) and decision-making algorithms to develop our hybrid artificial intelligent system (Ankara System Version 5.0). Wavelet transformation is used for feature extraction(12,13). Then, the extracted 100 features were used for the classification steps(16,17). In the first step of classification, an unsupervised ANN (vector quantization) was used for clustering. In the second step of the classification, we used a supervised ANN (backpropagation learning algorithm) and thus classified the tracings as either assuring or non-assuring. The sensitivity and specificity of the Ankara System (version 5.0) were found to be 61.25% and 98.68%, respectively. We believe the statistical measures of this version are sufficient enough and may be used, as well as classical NST, which is especially important in the perinatal surveillance of high-risk pregnancies.
Caron et al. developed a system for the computerized assessment of fetal behavioral states in order to guide the physicians objectively for the management of pregnancies, with promising results(8). Similarly, Hiett et al. used the Oxford Sonicaid System 8000 for comparing visual versus computerized analysis of non-stress tests(6). Non-stress tests of 575 high-risk patients were analyzed by two experts and the computerized system, without knowledge of the pregnancy outcomes. Similar rates of sensitivity, specificity, and positive and negative predictive values were found in both approaches. Thus, the authors concluded that automated fetal heart rate testing might become an acceptable alternative to conventional visual analysis(6).
Furthermore, Joana Lopes-Pereira et al. conducted a retrospective cohort study including 38,466 deliveries to evaluate the performance of the Omniview-SisPorto system in assisting physicians for the interpretation of intrapartum cardiotocography traces(7). A significant reduction in the incidence of hypoxic-ischemic encephalopathy and a modest reduction in caesarean deliveries were observed(7). However, there are some studies in the literature with conflicting results(9,28). Two recent examples of meta-analyses did not report favorable outcomes with the application of computerized systems. However, these studies had some limitations due to inclusion criteria, risk of bias and study design(9,28).
We believe that these types of decision-making technologies and models are important in order to produce better results and increased objectivity in the evaluation of FHR tracings(3-9). Another advantage of “expert and the artificial intelligent systems” is the possibility of producing institute-based versions (in terms of expert physicians and hardware). However, there are still standardization problems related to methodological and technological differences. In this version, we chose to use single expert FHR evaluations at the training phase, in order to maintain uniformity for the final interpretations. We believe that our approach will stimulate further studies in this field.
In conclusion, the methodologies used in the creation of a hybrid artificial intelligent system (Ankara System Version 5.0) might be an alternative for future computerized systems to be used in the interpretation of FHR tracings.
Acknowledgments: Special thanks to all perinatology staff who work with devotion for improving the health standards of the patients.
Funding: No funding was used for this study.
Conflict of interests: The authors declare no conflict of interests.
Bibliografie
- Practice bulletin no. 145: antepartum fetal surveillance. Obstet Gynecol. 2014;124(1):182-92.
- Grivell RM, Alfirevic Z, Gyte GM, Devane D. Antenatal cardiotocography for fetal assessment. Cochrane Database Syst Rev. 2015(9):Cd007863.
- Beksaç MS, Karakaş Ü, Yalçin S, Özdemir K, Şanlitürk E. Computerized analysis of antepartum fetal heart rate tracings in normal pregnancies (version 88/2.29). Eur J Obstet Gynecol. 1990;37(2):121-32.
- Beksaç MS, Özdemir K, Karakaş Ü, Yalçin S, Karaağaoğlu E. Development and application of a simple expert system for the interpretation of the antepartum fetal heart rate tracings (version 88/2.29). Eur J Obstet Gynecol. 1990;37(2):133-41.
- Beksaç MS, Önderoğlu L, Özdemir K, Karakaş Ü. The validation of a computerized system for the interpretation of the antepartum fetal heart rate tracings (version 89/2.34). Eur J Obstet Gynecol. 1991;42(1):9-14.
- Hiett AK, Devoe LD, Youssef A, Gardner P, Black M. A comparison of visual and automated methods of analyzing fetal heart rate tests. Am J Obstet Gynecol. 1993;168(5):1517-21.
- Lopes-Pereira J, Costa A, Ayres-De-Campos D, Costa-Santos C, Amaral J, Bernardes J. Computerized analysis of cardiotocograms and ST signals is associated with significant reductions in hypoxic-ischemic encephalopathy and cesarean delivery: an observational study in 38,466 deliveries. Am J Obstet Gynecol. 2019;220(3):269.e1-.e8.
- Caron FJ, van Geijn HP, van Woerden EE, Swartjes JM, Mantel R. Computerized assessment of fetal behavioral states. J Perinat Med. 1988;16(4):365-72.
- Balayla J, Shrem G. Use of artificial intelligence (AI) in the interpretation of intrapartum fetal heart rate (FHR) tracings: a systematic review and meta-analysis. Arch Gynecol Obstet. 2019;300(1):7-14.
- Macones GA, Hankins GD, Spong CY, Hauth J, Moore T. The 2008 National Institute of Child Health and Human Development workshop report on electronic fetal monitoring: update on definitions, interpretation, and research guidelines. Obstet Gynecol. 2008;112(3):661-6.
- Daubechies I. The wavelet transform, time-frequency localization and signal analysis. IEEE Trans Inf Theory. 1990;36(5):961-1005.
- Qu G, Zhang D, Yan P. Medical image fusion by wavelet transform modulus maxima. Optics Express. 2001;9(4):184-90.
- Antonini M, Barlaud M, Mathieu P, Daubechies I. Image coding using wavelet transform. IEEE Trans Inf Theory. 1992;1(2):205-20.
- Yao X. Evolving artificial neural networks. Proc IEEE Inst Electr Electron Eng. 1999;87(9):1423-47.
- Sarle WS. Neural networks and statistical models. 1994.
- Krishnamurthy AK, Ahalt SC, Melton DE, Chen P. Neural networks for vector quantization of speech and images. IEEE J Sel Areas Commun. 1990;8(8):1449-57.
- Riedmiller M. Advanced supervised learning in multi-layer perceptrons – from backpropagation to adaptive learning algorithms. Computer Standards & Interfaces. 1994;16(3):265-78.
- Pillai M, James D. The development of fetal heart rate patterns during normal pregnancy. Obstet Gynecol. 1990;76(5 Pt 1):812-6.
- Electronic fetal heart rate monitoring: research guidelines for interpretation. National Institute of Child Health and Human Development Research Planning Workshop. Am J Obstet Gynecol. 1997;177(6):1385-90.
- Fetal Assessment. In: Cunningham F, Leveno KJ, Bloom SL, Dashe JS, Hoffman BL, Casey BM, Spong CY. eds. Williams Obstetrics, 25th edition. McGraw Hill; 2018.
- Beksac M, Beksac MS, Tipi VB, Duru HA, Karakaş MÜ, Çakar AN. An artificial intelligent diagnostic system on differential recognition of hematopoietic cells from microscopic images. Cytometry Part A. 1997;30(3):145-50.
- Beksac MS, Başaran F, Eskiizmirliler S, Erkmen AM, Yörükan S. A computerized diagnostic system for the interpretation of umbilical artery blood flow velocity waveforms. Eur J Obstet Gynecol. 1996;64(1):37-42.
- Beksaç MS, Durak B, Özkan Ö, Çakar AN, Balci S, Karakaş Ü, et al. An artificial intelligent diagnostic system with neural networks to determine genetical disorders and fetal health by using maternal serum markers. Eur J Obstet Gynecol. 1995;59(2):131-6.
- Beksaç MS, Tanacan A, Bacak HO, Leblebicioglu K. Computerized prediction system for the route of delivery (vaginal birth versus cesarean section).
- J Perinat Med. 2018;25(46):881-884.
- Beksaç MS, Eskiizmirliler S, Çakar AN, Erkmen AM, Dağdeviren A, Lundsteen C. An expert diagnostic system based on neural networks and image analysis techniques in the field of automated cytogenetics. Technol Health Care. 1996;3(4):217-29.
- Beksaç MS, Egemena A, Karakaş Ü. An intelligent diagnostic system for the assessment of gestational age based on ultrasonic fetal head measurements. Technol Health Care. 1996;4(2):223-31.
- Bacak HO, Leblebicioglu K, Tanacan A, Sinan Beksac M. Computerized hybrid decision-making system for hormone replacement therapy in menopausal women. Technol Health Care. 2019;27(1):49-59.
- Campanile M, D’Alessandro P, Della Corte L, Saccone G, Tagliaferri S, Arduino B, et al. Intrapartum cardiotocography with and without computer analysis: a systematic review and meta-analysis of randomized controlled trials. J Matern Fetal Neonatal Med. 2020;33(13):2284-2290.
Articole din ediţiile anterioare
Teenage pregnancy – an unsolved problem of the 21st century. Populational register-based study in the County Clinical Hospital Constanţa
Studies regarding pregnant teenagers were carried out at the beginning of the 1950s, attracting the attention of both the medical community and var...
Disseminated intravascular coagulation in obstetrics: mini-review
Obstetric hemorrhage is a major cause of maternal morbidity and mortality. Acquired coagulopathy can develop rapidly in severe obstetric hemorrhage...
Spontaneous heterotopic pregnancy with ampullar location of the ectopic pregnancy – case report and literature review
The coexistence of ectopic and eutopic pregnancy has different clinical forms, the ectopic pregnancy having various locations: tubal, interstitial,...
What do we know about imaging in pregnancy?
Many conditions in pregnancy require noninvasive paraclinical examinations. These kinds of tests should never replace a good clinical examination, ...