Angiosarcoma of the seminal vesicle is a rare malignancy. We present the case of a 33-year-old male patient with nonspecific symptoms and recent pelvic pain aggravation. CT and MRI evaluations revealed a right seminal vesicle tumoral mass. The histopathological exam after transrectal biopsy of the right seminal vesicle mass was in favor of an epithelioid angiosarcoma. Surgical resection of the right seminal vesicle was performed, followed by neoadjuvant chemotherapy. Imaging is important to evaluate the tumoral local extension and the metastatic spread.
IMAGING IN ONCOLOGY
Imaging of seminal vesicle angiosarcoma – a rare entity
Imagistica angiosarcomului de veziculă seminală – o entitate rară
First published: 23 martie 2023
Editorial Group: MEDICHUB MEDIA
DOI: 10.26416/OnHe.62.1.2023.7751
Abstract
Rezumat
Angiosarcomul veziculei seminale este o malignitate rară. Prezentăm cazul unui pacient de sex masculin, în vârstă de 33 de ani, cu simptome nespecifice şi cu agravarea recentă a durerilor pelviene. Evaluările CT şi IRM au evidenţiat o masă tumorală la nivelul veziculei seminale drepte. Examenul histopatologic efectuat după biopsia transrectală a masei tumorale a fost în favoarea unui angiosarcom epitelioid. A fost efectuată rezecţia chirurgicală a veziculei seminale drepte, urmată de chimioterapie neoadjuvantă. Imagistica este importantă pentru bilanţul local al extensiei tumorale şi pentru evaluarea metastazelor la distanţă.
Introduction
Usually, tumors of the seminal vesicles represent a contiguous invasion of malignancies involving adjacent organs, most commonly located into the prostate tissue. Tumors originating de novo in the seminal vesicles are much rarer. Imaging is important to make a pre-therapeutic locoregional tumoral extension and, also, for distant metastases.
Clinical history
A 33-year-old male with no significant past medical history presented to our hospital with mild and nonspecific pelvic pain for the last two months, with recent aggravation.
Imaging findings
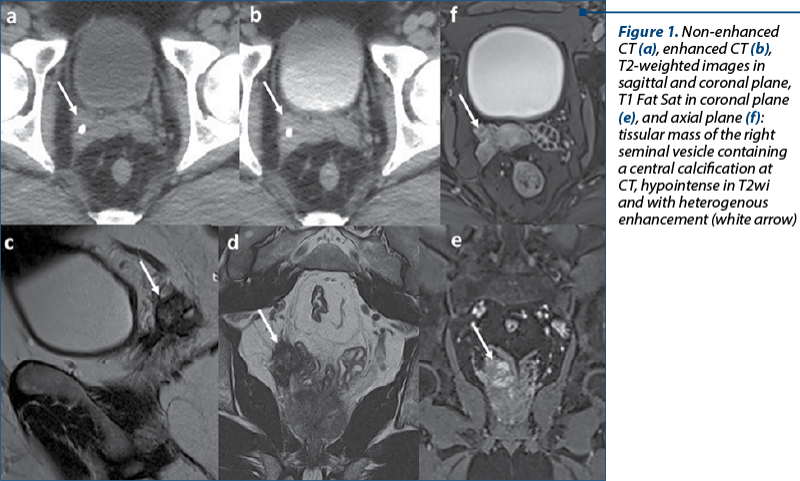
A contrast-enhanced CT was performed which revealed a heterogeneous lesion involving the right seminal vesicle, with moderate enhancing and microcalcifications included. A pelvic magnetic resonance imaging (MRI) was performed to further characterize this mass. It showed a right vesicle lesion with hypointense signal on T2 weighted images and STIR. In diffusion-weighted images, the lesion presented areas with diffusion restriction and, after intravenous injection of extracellular paramagnetic gadolinium-based contrast, fat saturated T1-weighted images revealed early enhancement of the lesion. The mass was adjacent to the posterior-inferior wall of the urinary bladder and the ipsilateral mesorectal fascia (Figure 1). A transrectal biopsy of the right seminal vesicle soft tissue mass was performed which was reviewed at our institution and found to be a grade 2 (of 4) epithelioid angiosarcoma. Cystoscopy was negative, and the surgical excision of the right seminal vesicle was performed followed by neoadjuvant chemotherapy.
Discussion
Soft tissue sarcomas can develop in any type of the connective tissue throughout the body, representing 1-2% of all cancers(1). Vascular sarcomas are uncommon vasoformative soft tissue tumors and include angiosarcomas, hemangioendotheliomas and hemangiopericytomas. Angiosarcomas comprise less than 1% of all sarcomas, with a similar distribution between genders, and they can occur at any ages. Epithelioid angiosarcoma refers to a variant of angiosarcoma composed of neoplastic cells that have an epithelioid appearance.
These tumors are usually poorly differentiated and biologically aggressive(2,3). Angiosarcoma may arise from any anatomic site, but they occur more frequently in the skin or superficial soft tissues, predominantly in the scalp, face, neck, extremities or breast. Angiosarcoma of the liver, lungs, heart, pelvis and retroperitoneum has also been reported. In particular, extremely few cases of angiosarcoma of the prostate or seminal vesicle have been reported in literature(1,4). For angiosarcoma of the seminal vesicle, the most common presenting symptom is represented by testicular/perineal pain or discomfort(4). This was also the case of our patient, because at admission his only complaint was a mild pelvic pain for the last two months with recent aggravation. The etiology of angiosarcoma is not fully understood, but there are several reported risk factors, including prior exposure to ionizing radiation or toxic chemicals, chronic lymphedema (Stewart-Treves syndrome) and venous stasis, although most patients diagnosed with angiosarcoma have no noticeable risk factors, as it was the case of this patient(1).
Ultrasound, CT and MRI are diagnostic tools, but the final diagnosis requires pathological and immunohistochemical confirmation(1,4). Immunohistochemical stains showed that the tumor cells reacted diffusely with antibodies to CD31 and vimentin, but did not react with antibodies to S-100, oct4, CK7, CK20, EMA, NKX3.1, WT1 and calretinin. In our case, positive immunostaining for CD31 and vimentin were consistent with a diagnosis of angiosarcoma and, at the same time, the absence of immunoreactivity for other tissular markers excluded other tumoral entities, such as carcinoma/adenocarcinoma (urothelial, prostatic, seminal or intestinal – CK7, CK20, EMA and NKX3.1 negative), germ cell tumors (oct4 negative), metastatic melanoma (S100 negative), Müllerian carcinoma (WT1 negative), sex cord-gonadal stromal tumor (calretinin negative)(1,2). Due to the uncommonness of these tumors, the optimal therapeutic strategy is still argued. Radical surgery remains the cornerstone of all treatments for angiosarcoma. Consequent to the extensive nature and the rapid progression of the disease, positive surgical margins are common in resection and adjuvant chemotherapy or radiation should also be considered(1,4). Our case meets the requirements for a primary seminal vesicle tumor confined to the right seminal vesicle, and no other primary tumor was found(5). Even with an appropriate treatment, surgical resection followed by neoadjuvant chemotherapy, the prognosis is poor, with rapid widespread metastases and fatal outcome(3).
Conflict of interest: none declared
Financial support: none declared
This work is permanently accessible online free of charge and published under the CC-BY.

Bibliografie
-
Cao J, Wang J, He C, Fang M. Angiosarcoma: a review of diagnosis and current treatment. Am J Cancer Res. 2019;9(11):2303-2313.
-
Koch M, Nielsen GP, Yoon SS. Malignant tumors of blood vessels: Angiosarcomas, hemangioendotheliomas, and hemangiopericytomas. J Surg Oncol. 2008;97(4):321-329. doi: 10.1002/jso.20973.
-
Espat NJ, Lewis JJ, Woodruff JM, et al. Confirmed angiosarcoma: prognostic factors and outcome in 50 prospectively followed patients. Sarcoma. 2000;4:173-177. doi: 10.1080/13577140020025896.
-
Chang K, Sio TT, Chandan VS, Iott MJ, Hallemeier CL. Angiosarcoma of the seminal vesicle: a case report of long-term survival following multimodality therapy. Rare Tumors. 2014;6(1):5202. doi: 10.4081/rt.2014.5202.
-
Lamont JS, Hesketh PJ, de las Morenas A, Babayan RK. Primary Angiosarcoma of the Seminal Vesicle. Journal of Urology. 1991;146(1):165-167. doi: 10.1016/S0022-5347(17)37743-1.
Articole din ediţiile anterioare
IMAGING IN ONCOLOGY | Ediţia 1 66 / 2024
Nontraumatic splenic emergencies in onco-hematological pathology: what is important to know in CT evaluation?
Ioana G. Lupescu, Cristian Anghel, Dumitru Radu-Lucian , Cristina Dumitrescu, Dijmărescu Adrian , Mugur C. Grasu
Scopul acestui articol este de a prezenta şi ilustra aspectele computer-tomografice (CT) înâlnite în urgenţele splenice – vasculare şi infecţioase ...
27 martie 2024
BREAST CANCER | Ediţia 3 / 2015
Terapia anti HER-2 în cancerul sânului, o scurtă privire asupra opţiunilor terapeutice disponibile
Dan Ilie-Damboiu
În această prezentare voi detalia noile terapii disponibile pentru tratarea cancerului de sân cu supraexpresie HER-2 (o oncogenă a familiei EGFR - ...
24 octombrie 2015
HEMATO-ONCOLOGY | Ediţia 2 47 / 2019
Urgenţele neurologice în leucemiile acute: ce este important să ştim?
Ioana G. Lupescu
La pacienţii cu leucemie acută, urgenţele neurologice reprezintă complicaţii redutabile care pot agrava cursul bolii de bază sau pot produce d...
16 mai 2019