An important stage in the workflow of obtaining complete dentures for edentulous patients is represented by determining and registering the occlusal vertical dimension (OVD). The dentist has an important role in this clinical stage, and all the data that will be transmitted to dental laboratory must be correctly applied by the dental technician. The data are related to occlusal vertical dimension, smile line, midline and canine line.
INTERDISCIPLINARY
Aspecte practice privind corelaţia dintre dimensiunea verticală de ocluzie şi aspectul facial în edentaţia totală
Practical aspects regarding the correlation between the occlusal vertical dimension and the facial aspect of edentulous patients
Iuliana Babiuc,
Mihai-Alexandru Gărgăianu,
Radu Costea,
Viorel Ştefan Perieanu,
Mircea Popescu,
Mădălina Violeta Perieanu,
Ileana Ionescu,
Mihai Burlibaşa
First published: 03 martie 2023
Editorial Group: MEDICHUB MEDIA
DOI: 10.26416/ORL.58.1.2023.7666
Abstract
Rezumat
După cum bine ştim, munca medicului stomatolog este deosebit de importantă atunci când se realizează o determinare corectă a dimensiunii verticale de ocluzie a pacientului şi reprezintă un element premergător pentru edentaţii totali bimaxilari. Concret, este esenţial ca, ulterior, tehnicianul dentar să respecte toate reperele transmise de cabinetul de stomatologie către laboratorul de tehnică dentară, repere care pot fi contabilizate în felul următor: dimensiunea verticală de ocluzie, linia surâsului, linia mediană, linia caninilor.
Introduction
The topic of this material is a relevant parallel between the work of dentist and that of the dental technician in the process of obtaining complete dentures. The occlusal vertical dimension is an important criterion in designing and manufacturing prosthetic restorations both in classic rehabilitation (complete acrylic dentures) and in modern treatments (implant supported prosthetic restorations)(1-4).
A large number of edentulous patients choose complete dentures as a treatment option. In order to obtain an accurate denture, some rigorous stages must be followed; among those is determining the occlusal vertical dimension. This stage will make the difference between a well-fitting, functional and with a natural look denture and a misplaced, nonfunctional and unesthetic denture. Regardless of the prosthetic treatment option, on the first place there should be the functionality, and secondly, the esthetic aspect given by the prosthetic restoration(1-4).
The approach to such a subject was motivated by the actual trend, which places special emphasis on oral esthetic/facial esthetic. If a decade ago the perception in dentistry was associated with the need or the pain, nowadays things have substantially evolved regarding education (of oral hygiene), the way dental services are promoted, and the perception of patients about beauty and oral esthetics. Patients have become much more demanding and their expectations have grown exponentially, therefore dental treatments performed by dentist together with dental technicians must be as accurate, functional, biocompatible, durable and esthetic as possible(1-4).
This study is based on a clinical case presentation of two edentulous patients who required prosthetic treatment with complete dentures. The informal consent of the patients for using pictures from frontal and lateral view, made during treatment stages, was obtained and attached to the medical file.
Case presentations
Clinical case no. 1
This is a facial analysis of an edentulous, maxillary and mandibular male patient without dentures and different values of occlusal vertical dimension.
A 71-year-old male edentulous patient, who started the prosthetic treatment two months after the last tooth extractions, presented to the dental office for prosthetic treatment.
Following functional and anthropologic measurements, a 64-mm occlusal vertical dimension was established. Occlusal rims were modified to easily observe facial modifications in case of reduction or increase of occlusal vertical dimension.
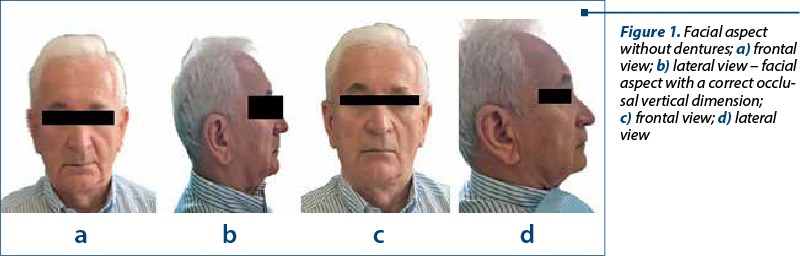
Without dentures, the patient presented a reduction of the lower face zone due to the lack of lips support by teeth. From a frontal view, perioral grooves were deeper and the lip vermilion was less visible. The lower face zone was reduced in relation to the middle face zone, and the facial appearance was aged (Figure 1a). From the lateral view, the nasolabial angle was obtuse and lips were distal from the esthetic plane (E-plane based on Ricketts analysis) – Figure 1b.
When determining the relationship between maxillary and mandible, a value of 64 mm was established for the occlusal vertical dimension (OVD). For this value, the facial aspect becomes harmonious, the soft tissues have an optimal support, and a correct proportionality of face levels is obtained. Perioral grooves and wrinkles are diminished (Figure 1c). Also, from the lateral view, the nasolabial angle of approximative 90° can be observed. The face profile becomes slightly convex, with a lip placement much normal in relation with the esthetic plane (Figure 1d).
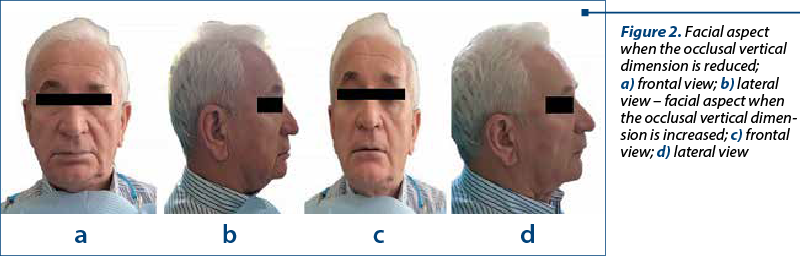
The occlusal vertical dimension was reduced with 3 mm till 61 mm to analyze the induced changes. In this new situation, the facial aspect becomes aged. Some changes of facial elements can be noticed, as follows: the orientation of the oral commissures downward, overexposure of the lower lip, the deepen of mentolabial sulcus, lower third of the face reduced compared to middle third of the face, and the chin closer to tip of the nose (Figure 2a). The decrease of the lower third of the face is more obvious from lateral view and, also, the mentolabial sulcus is more deepen (Figure 2b).
Subsequently, the occlusal rims were modified by increasing the occlusal vertical dimension till 67 mm. The effect was the increase of the lower third of the face, and the patient had an elongated face and a facial expression of fatigue. The patient made an effort to touch the lips when viewed from the front (Figure 2c). The proportion between the middle and lower third of the face was altered, and this aspect can be seen from frontal and lateral view (Figure 2d).
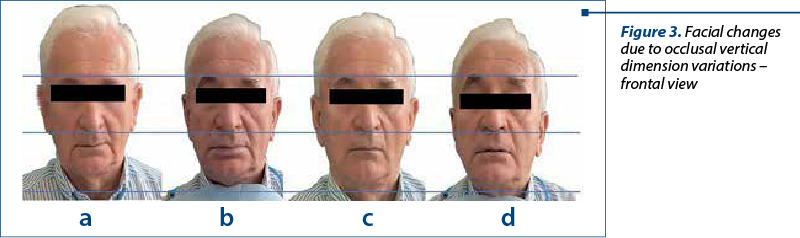
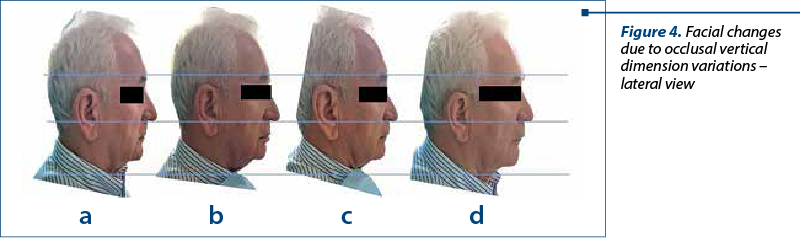
A comparison of the previously described situations shows the facial changes that appear when the occlusal vertical dimension is modified. The calibration of the photos was done relative to the middle third of the face (Figures 3 and 4).
Clinical case no. 2
This is a facial analysis of an edentulous, maxillary and mandibular female patient without dentures and with different values of occlusal vertical dimension.
A 52-year-old female patient, with edentulous maxillary arch for approximate five years and edentulous mandibular arch for approximate two years, presented to the dental office for prosthetic treatment.
As in the first clinical case, using functional and anthropologic measurements, a 58-mm occlusal vertical dimension was established, a value at which the facial harmony can be noticed, a well-balanced proportion between facial levels and a normal arrangement of soft tissues (Figure 5a). From the lateral view, a normal profile is noticed, with lips correctly placed in relation to the esthetic plane (E-plane) – Figure 5b.
Without maxillary denture, the lower level of the face is reduced, the upper lip is collapsed, perioral wrinkles and nasolabial grooves are deepened due to the lack of lips support from natural teeth. The chin becomes protrusive, the oral commissures are orientated downwards, and the upper lip vermilion is reduced (Figure 5c). From the lateral view, the decrease of the lower level of the face can be noticed, and the profile of the face becomes concave (Figure 5d).
When using the occlusal rims with a lower occlusal vertical dimension, with the value of 55 mm, changes were found compared to a normal lower level of the face. The noticed things were: oral commissures oriented further more downwards, deepened nasolabial grooves, reduced visibility of lip vermilion, reduced proportion of the lower level of the face compared to the middle third of the face, and chin closer to the tip of the nose (Figures 6a and 6b).
Occlusal rims were subsequently modified by increasing the occlusal vertical dimension up to 61 mm. The increase of the lower level of the face gave the patient a facial expression of fatigue, the upper lip was slightly tensioned and the phonetic test was altered. From the frontal view, it can be noticed that the patient struggles to contact the upper lip with the lower lip (Figure 6c). From the lateral view, the profile of the face is flattened (Figure 6d).
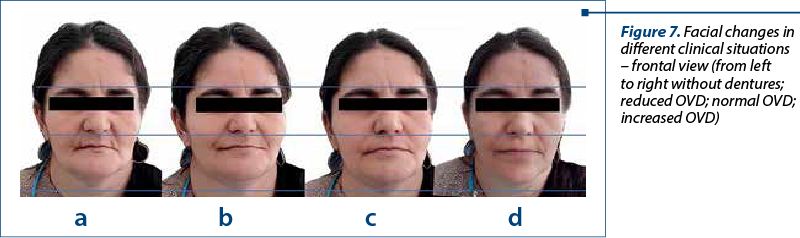
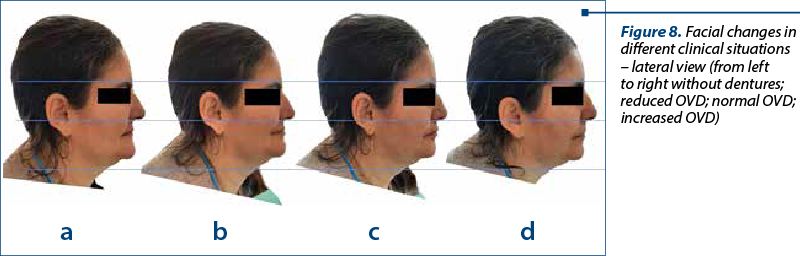
A much more natural aspect can be observed when using the OVD established as a reference compared with the first image where the OVD is reduced, wrinkles are deepened, and a reduced value of the lower level of the face can be noticed.
Even though in the last picture the patient had a balanced esthetic look, performing phonetic test revealed that speech and pronunciation of phonemes were done with difficulty.
Figures 7 and 8 compares the facial changes induced by modifying the occlusal vertical dimension. The calibration of pictures was made using for reference the dimension of the middle third of the face.


Discussion
Determining the occlusal vertical dimension is an important stage in the treatment of edentulous patients, with complete dentures or implant supported restorations. In literature, numerous methods of determining OVD are described, from pre-extraction photographs to different functional tests(5,6).
Edentulous arches (maxillary and/or mandibular) combined with the lack of prosthetic treatment generate esthetic and/or functional changes. Esthetically, there can be noticed deeper wrinkles and grooves around mouth, collapse of upper lip, and lower facial third reduced compared to middle facial third, creating an aged aspect of the patient(7-10).
From a functional point of view, the most frequent ailments are related to mastication, deglutition, speaking, temporomandibular dysfunctions, and masticatory muscle pain. Those ailments are caused by the decrease of occlusal vertical dimension due to the lack of teeth on one or both arches(11-16).
The esthetic changes can have psychological implications on the patient, creating feelings of anxiety and difficulties of integrating into society(17).
The purpose of dental treatment with complete acrylic dentures is to restore the morphology and functionality of edentulous arches. Thus, all esthetic and functional imbalances caused by edentulism should be remedied with the help of dentures. However, there are situations in which prosthetic treatment does not provide adequate results, the problem being generated by an occlusal vertical dimension inadequate to the clinical case.
A reduced value of OVD keeps the aged facial aspect and overloads the masticatory muscles, while an increased value of OVD determines an elongate aspect of the face and temporomandibular joint problems.
Conclusions
Even though for de edentulous patient dentures are a compromise solution, they can become viable long-term solutions.
Complete acrylic dentures ensure the restoration of mastication, deglutition, phonation, facial esthetics, the balance function of the cranio-cervico-mandibular system and of the temporomandibular joint. Furthermore, complete acrylic dentures help patients to regain an emotional balance.
From an esthetic point of view, using complete dentures, the treatment can correct or diminish some pathological defects, such as: reverse overjet, dental crowding, open occlusion frontal or lateral, overbite etc.
A reduced occlusal vertical dimension will determine an aged facial aspect, with deepening of perioral grooves and wrinkles, oral commissures orientated downward, and a reduced lower level of the face.
An increased occlusal vertical dimension determines an elongated face and a facial expression of fatigue. The patient develops difficulties in phonation and in maintaining his lips in contact. During speech, dentures make contact, producing a specific noise, a castanets sound.
As the mandible has an important role in the balance of the head, its position in relation with the base of the skull influences the cranio-cervico-mandibular system and modifies the position of the head, especially the cranio-cervical angle.
Some incorrect relationships between maxillary and mandible can be hiden by patients wearing mustache or beard. Changes that appear due to a tainted occlusal vertical dimension can be easily hidden when the thickness of soft tissues is higher.
Thus, this article highlights the importance of an accurate determination of occlusal vertical dimension regarding the esthetic and facial changes that appear, and from the point of view of functionally. A proper occlusal vertical dimension ensures an efficient mastication, a correct phonation, optimum deglutition, the prophylaxis of temporomandibular joint and, finally, a good functioning of the cranio-cervical-mandibular system. n
Acknowledgement: Viorel Ştefan Perieanu is the corresponding author and has equally contributed to this paper with the first author.
Conflict of interest: none declared
Financial support: none declared
This work is permanently accessible online free of charge and published under the CC-BY.

Bibliografie
-
Săbăduş I. Proteza totală, ştiinţă, artă şi tehnică. Cluj-Napoca: Ed. Dacia, 1995.
-
Ioniţă S, Petre A. Ocluzia dentară, noţiuni de morfologie, fiziologie, patologie şi tratament. Bucharest, Ed. Didactică şi Pedagogică, 1996.
-
Pancă A, Bechir A, Damian I, Moldoveanu L. Tehnologia protezei totale. Constanţa, Ed. Ovidius University Press, 2004.
-
Hutu E, Păuna M, Bodnar V. Edentaţia totală. Bucureşti, Ed. Naţional, 2005.
-
Fayz F, Eslami A. Determination of occlusal vertical dimension: a literature review. J Prosthet Dent. 1988 Mar; 59(3): 321-3. doi: 10.1016/0022-3913(88)90182-5.
-
Lechner SK. Vertical dimension for the older patient. Ann R Australas Coll Dent Surg. 1989 Oct;10:91-100.
-
Toyoshima GHL, Pucciarelli MGR, Neppelenbroek KH, Sforza C, Menezes M, Oliveira TM, Soares S. Evaluation by 3D stereophotogrammetry of facial changes in edentulous patients after rehabilitation. J Appl Oral Sci. 2021 Dec;30:e20210462. doi: 10.1590/1678-7757-2021-0462.
-
Yuan F, Cheng C, Dai N, Sun Y. Prediction of aesthetic reconstruction effects in edentulous patients. Sci Rep. 2017;7(1):18077. doi: 10.1038/s41598-017-17065-y.
-
The Academy of Prosthodontics. The glossary of prosthodontic terms: ninth edition. J Prosthet Dent. 2017;117(5S):e1-e105. doi:10.1016/j.prosdent.2016.12.001.
-
Raschke GF, Eberl P, Thompson GA, Güntsch A, Peisker A, Schultze-Mosgau S, Gomez-Dammeier M, Djedovic G, Rieger UM, Beuer F. Wearing complete dental prostheses - Effects on perioral morphology. Med Oral Patol Oral Cir Bucal. 2016 Jul;21(4):e413-9. doi: 10.4317/medoral.21102.
-
Sierpinska T, Golebiewska M, Kuc J, Lapuc M. The influence of the occlusal vertical dimension on masticatory muscle activities and hyoid bone position in complete denture wearers. Adv Med Sci. 2009;54(1):104-8. doi: 10.2478/v10039-009-0018-3.
-
Rodrigues Garcia RC, Oliveira VM, Del Bel Cury AA. Effect of new dentures on interocclusal distance during speech. Int J Prosthodont. 2003 Sep-Oct;16(5):533-7.
-
Tallgren A, Tryde G, Mizutani H. Changes in jaw relations and activity of masticatory muscles in patients with immediate complete upper dentures.
-
J Oral Rehabil. 1986 Jul;13(4):311-24. doi: 10.1111/j.1365-2842.1986.tb00665.x.
-
Battistuzzi PG, Favero GA, Cordioli PG. L’edentulia parziale: Eziologia ed alterazioni funzionali [Partially edentulous patients: etiology and functional changes]. G Stomatol Ortognatodonzia. 1983 Jan-Mar;2(1):65-9.
-
de Souza RF, Marra J, Pero AC, Compagnoni MA. Effect of denture fabrication and wear on closest speaking space and interocclusal distance during deglutition. J Prosthet Dent. 2007 Jun; 97(6):381-8. doi: 10.1016/S0022-3913(07)60027-4.
-
Jeanmonod A. The diagnosis and treatment of temporomandibular dysfunctions in older, partially or totally edentulous patients. Int Dent J. 1982 Dec;32(4):339-44.
-
Parker HM. Psychological implications of provisional prostheses. Dent Clin North Am. 1989 Jul; 33(3):343-53.