Both the classic method of manufacturing the metal infrastructure of fixed metal-ceramic prosthetic restorations, as well as modern digital technologies, such as CAD/CAM, offer the patient a stable, resistant prosthetic work, with superior esthetics. Due to the high cost of fixed prosthetic restorations made by CAD/CAM technology, they address a smaller number of patients, which is a disadvantage. However, the CAD/CAM method requires a smaller number of production steps than the conventional method, and the errors that may occur along the way are considerably fewer than the errors present during the transformation of the wax pattern into the metal part (by casting).
Classic versus digital in the fabrication of the metal infrastructure of fixed prosthetic restoration (Part I)
Clasic versus digital în realizarea infrastructurii metalice a restaurărilor protetice fixe (partea I)
Mihai David,
Dorina-Mihaela Gheciu,
Radu Cătălin Costea,
Viorel Ştefan Perieanu,
Gabriela Tănase,
Mădălina Violeta Perieanu,
Mircea Popescu,
Bogdan Alexandru Dimitriu,
Irina Adriana Beuran,
Mihai Burlibaşa
First published: 28 septembrie 2023
Editorial Group: MEDICHUB MEDIA
DOI: 10.26416/ORL.60.3.2023.8590
Abstract
Rezumat
Atât metoda clasică de confecţionare a infrastructurii metalice a restaurărilor protetice fixe metaloceramice, cât şi tehnologiile digitale moderne de tipul CAD/CAM oferă pacientului o lucrare protetică stabilă, rezistentă şi cu o estetică superioară. Din cauza costului ridicat al restaurărilor protetice fixe realizate prin tehnologia CAD/CAM, acestea se adresează unui număr mai restrâns de pacienţi, ceea ce reprezintă un dezavantaj. Totuşi, metoda CAD/CAM presupune un număr de etape de realizare mai mic decât metoda convenţională, iar erorile ce pot apărea pe parcurs sunt considerabil mai puţine decât erorile prezente pe parcursul transformării machetei în piesa metalică (turnare).
Introduction
Since its beginnings, dental technology has been in a continuous process of innovation and development. Currently, the methods of obtaining prosthetic parts are divided into two categories: analog and digital. In our case, we are actually discussing two methods of obtaining the metal infrastructures of fixed prosthetic restorations: classic and modern(1-4).
Thus, in a first stage, the method of obtaining the metal infrastructures with the help of classic casting technologies, already well-known and which require not only a sequence of well-defined, relatively complicated clinical-technical work stages, but also a generous endowment of the dental laboratory, doubled by a very good training of the dental technicians who perform these operations.
When talking about digital methods of obtaining the metal infrastructures of fixed prosthetic restorations, we are actually talking about modern technologies, namely CAD/CAM technology, which involves not only a considerable financial effort on the part of those who own the dental laboratory, the necessary equipment being very expensive, but also a much more serious financial effort on the part of the patients who will be the beneficiaries of the prosthetic restorations executed with the help of this revolutionary technology (the finished products).
Specifically, this new CAD/CAM technology also appeared in Romania, becoming one of the most used technologies in dentistry, due to the advantages it presents: speed, simplicity and fidelity.
This paper, structured in two parts, aims at revealing the two methods of obtaining the metal infrastructure of metal-ceramic crowns and compare them. Next, we will present several practical aspects regarding obtaining the metal infrastructure of fixed prosthetic restorations by the conventional method, but also by CAD/CAM technology. Basically, we are discussing several cases of fixed metal-ceramic prosthetic restorations in which the metal infrastructure will be made both by the classical method, already established, and by the modern digital method, namely the CAD/CAM method.
Case presentation
A 36-year-old patient came to the dental office with a medical condition located in the maxillary arch. Thus, tooth 1.5 showed increased mobility, requiring extraction. The neighboring teeth of the edentulous space, 1.4 and 1.6, had no carious lesions. Following radiological examination, good implantation of teeth 1.4 and 1.6 was observed. Therefore, the dentist, in agreement with the patient, decided to fabricate a porcelain fused to metal bridge with three elements, using teeth 1.4 and 1.6 as abutments.
The metallic infrastructure of this prosthetic restoration was experimentally realized both by the classical method, but also by the modern CAD/CAM digital technology. The first version of the metal infrastructure was the classic one. Until the stage of making the functional model (the working model), the phases were common. After the moment of obtaining the functional model with removable abutments, the stages became totally different.
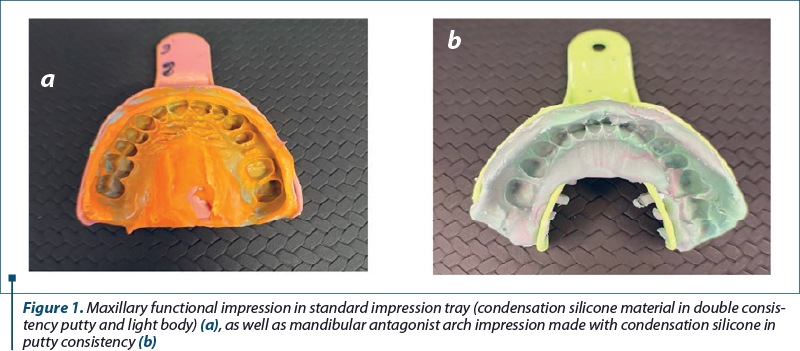
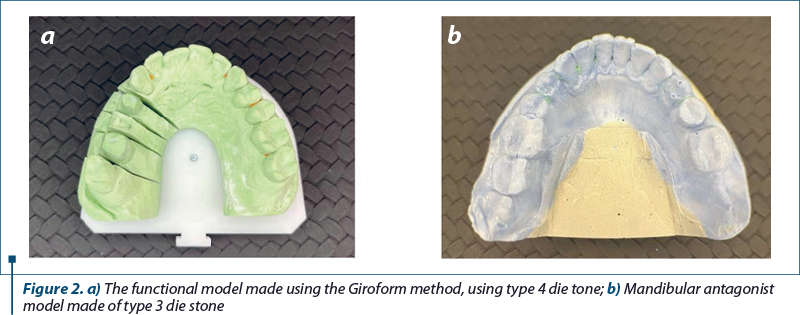
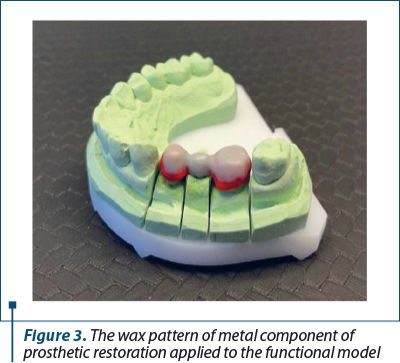
Thus, the dental treatment began by preparing the abutment teeth, root treatment followed by tooth preparation for the future prosthetic restoration. The prosthetic field was imprinted (the functional impression and the impression of the antagonist teeth) and also the interocclusal record was carried out (Figure 1). The impressions were washed under running tap water and then decontaminated by immersion in chemicals with disinfectant potential, according to the manufacturer’s recommended instructions. Next, the impressions were sent to the dental laboratory to obtain the functional and antagonist models (Figure 2). On the functional model, the wax pattern of metallic infrastructure was made respecting the minimum strength dimensions of the dental alloy to be used (Figure 3).
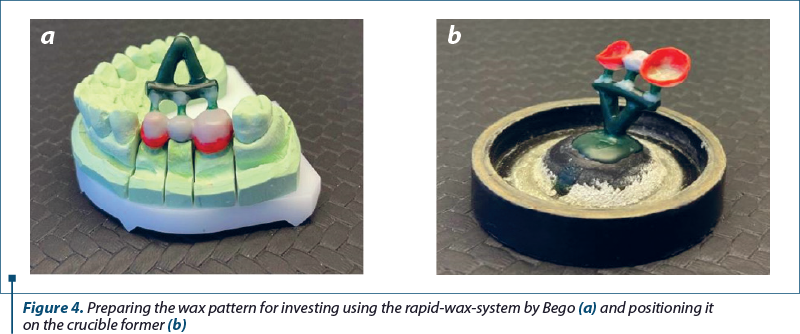
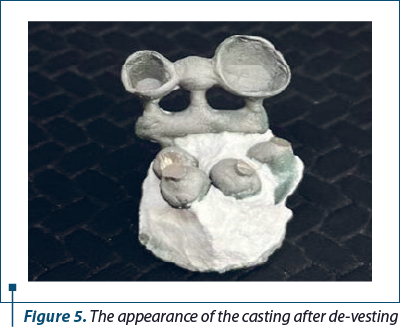
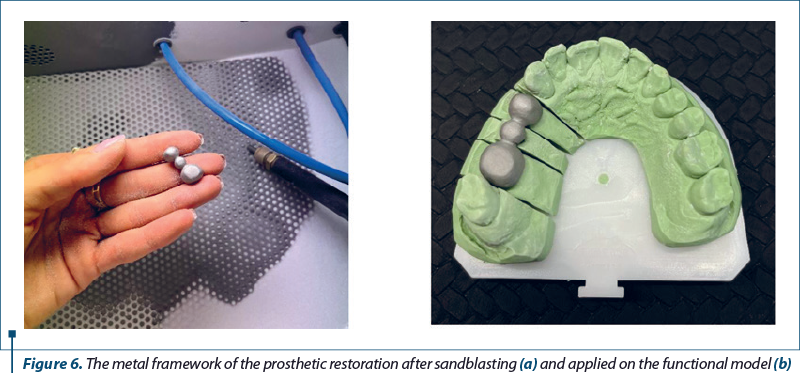
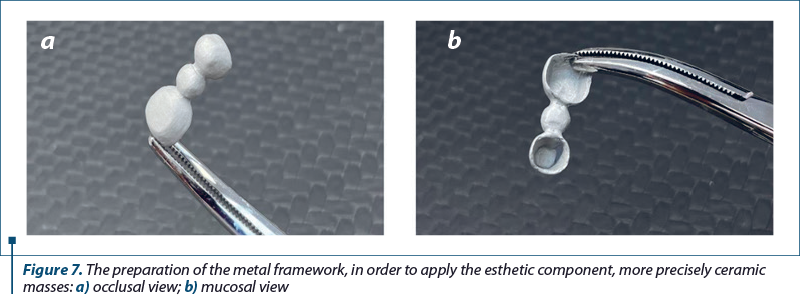
The wax pattern was prepared to be invested by applying a special sprue, rapid-wax-system (Bego-Heraeus) – Figure 4. After investing the wax pattern and setting of the material, the mould was obtained using a thermal treatment. At the end of the thermal conditioning of the mould, the metal was melted and inserted inside the mould using centrifugal force of an automatic casting machine. When the casting has cooled, it is de-vested, the investment material being removed from the surface of the casting piece (Figure 5). Any remaining investment material on the surface of the casting is removed using a sandblasting machine (Figure 6a). In the end, the metal framework obtained by casting is cut from the sprue and finished (Figure 6b, Figure 7).
Next, the same clinical case, but the metal infrastructure for the dental bridge supported on 1.4 and 1.6 was obtained by the CAD/CAM technology. Concretely, using the existing maxillary functional model, as well as the mandibular antagonist model, another method of making the metal infrastructure was chosen.
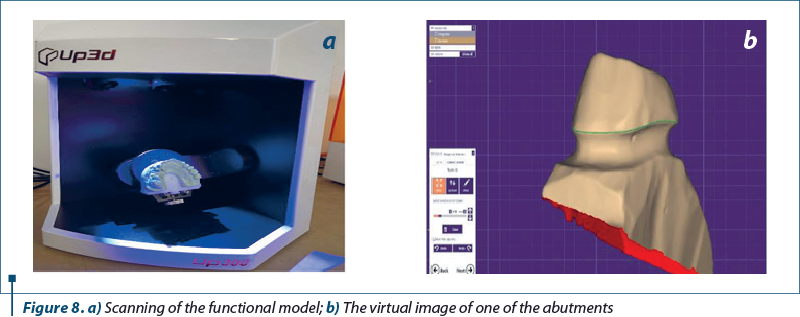
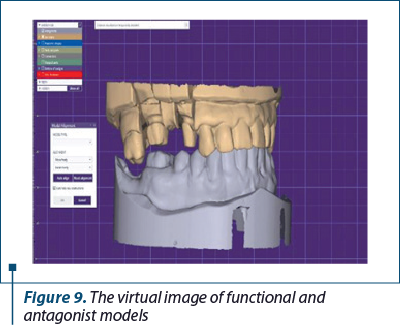
The removable abutments were coated with a thin layer of special wax for scanning. A dental laboratory scanner with automatic calibration and fast processing was used. The models were fixed in the scanner’s clamping system and the scanning process began (Figure 8a). The abutments were individually scanned with a higher resolution for a correct registration (Figure 8b). The virtual images of the functional and antagonist models were thus obtained (Figure 9).
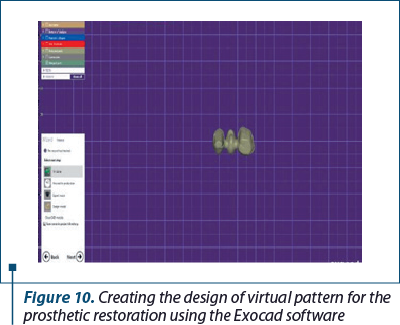
The design of the future metal infrastructure for the metal-ceramic prosthetic restoration that was made at the level of teeth 1.4-1.6 was created using the Exocad software.
Afterwards, the virtual pattern was sent in STL format to a milling center, the metal infrastructure being obtained following the complex milling process of the CAD/CAM system. After milling, the metal framework required less processing than copings or other type of prosthetic restorations obtained by conventional cast techniques (Figure 10).
Discussion
The process of obtaining metallic prosthetic restorations began with the studies carried out by Dr. Barnaba Frederick Philbrook (Denison, Iowa), who in 1897 published and delivered a lecture at the Thirty-Fourth Annual Meeting of Iowa State Dental Society (Des Moines, Iowa), an article titled “Cast Fillings”, a paper describing the process of obtaining gold inlays using the lost-wax casting technique by melting/casting(5). The technological evolution has allowed the creation of new devices that allow the creation of metallic prosthetic components by melting dental alloys and their insertion in preheated mould, technology widely used at the moment.
The development of new dental alloys, especially Ti-based ones, with a superior biocompatibility to those existing on the market, has raised new technological problems regarding the devices used to melt and cast alloys(6). Ti alloys, for dentistry, require equipment and special processing conditions to prevent contamination with various chemical elements, especially oxygen and nitrogen(6). This led to the emergence of new processing technologies (laser sintering, milling) which can also be applied to existing dental alloys.
The differences between the classic lost-wax technology and the modern CAD/CAM milling technology can be found throughout the technological flow. In the classic technique, the dental technician must allocate more time, the number of technological stages being higher, and it requires more equipment and materials in the stages of preparation, processing and finishing(7).
CAD/CAM technology based on milling has a reduced number of steps, it uses a smaller amount of materials, but has as its main drawback the increased cost of the necessary equipment(7-9).
As recent studies on the accuracy of works made both conventionally and by milling technique show a superior accuracy of components made by CAD/CAM technology, it is very possible that, in the medium and long term, the classic technology for obtaining metal components will be replaced almost completely in the technological flow(7-16).
Conclusions
The CAD/CAM method requires a smaller number of production steps than the conventional method, and the errors that may occur along the way are considerably fewer than the errors present during the transformation of the model into the metal part (casting). Casting defects, unlike milling defects, are much more visible and require more intensive, time-consuming processing.
But what must be mentioned is the fact that both methods of obtaining fixed prosthetic restorations offer the patient a stable, resistant prosthetic work with superior esthetics. Due to the high cost of fixed prosthetic restorations made by CAD/CAM technology, they are addressed to a smaller number of patients, which is a big disadvantage.
Acknowledgement: Viorel Ştefan Perieanu and Gabriela Tănase are corresponding authors (Viorel Ştefan Perieanu: viorelperieanu@yahoo.com; Gabriela Tănase: tanasegabriela2@gmail.com); Bogdan Alexandru Dimitriu and Irina-Adriana Beuran have equally contribution with the first author.

Conflict of interest: none declared
Financial support: none declared
This work is permanently accessible online free of charge and published under the CC-BY.

Bibliografie
- Bereşescu G. Dinţii umani permanenţi. Ed. University Press, Târgu-Mureş, 2011.
- Nelson SJ, Ash MM. Wheeler’s Dental Anatomy, Physiology and Occlusion. 9th Ed. Saunders Elsevier, St. Louis, 2010.
- Bratu D, Nussbaum R. Bazele clinice şi tehnice ale protezării fixe. Ediţia a 3-a. Ed. Medicală, Bucureşti, 2011.
- Forna N, de Baat C, Bratu D, Mercut V, Petre A, Popşor S, et al. Protetică dentară. Ed. I, Vol. II. Ed. Enciclopedică, Bucureşti, 2011.
- Philbrook BF. Cast fillings. Transactions of the Iowa State Dental Society, 1897, p. 277-279. (Paper read before the Iowa State Dental Society, Thirty-fourth Annual Meeting, Des Moines, Iowa) Cedar Rapids, Iowa: T.S. Metcalf.
- Okabe T, Hero H. The use of titanium in dentistry. Cells and Materials. 1995;5(2):211-230.
- Mello CC, Lemos CAA, de Luna Gomes JM, Verri FR, Pellizzer EP. CAD/CAM vs Conventional technique for fabrication of implant-supported frameworks: A systematic review and meta-analysis of in vitro studies. Int J Prosthodont. 2019;32(2):182-192.
- Batson ER, Cooper LF, Duqum I, Mendonça G. Clinical outcomes of three different crown systems with CAD/CAM technology. J Prosthet Dent. 2014;112(4):770-7.
- Rekow ED. A review of the developments in dental CAD/CAM systems. Curr Opin Dent. 1992;2:25-33.
- Al-Fadda SA, Zarb GA, Finer Y. A comparison of the accuracy of fit of 2 methods for fabricating implant-prosthodontic frameworks. Int J Prosthodont. 2007;20(2):125-131.
- Burlibaşa M, Cernuşcă-Miţariu M, Cernuşcă-Miţariu S, Miţariu M, Maliţa M. Theoretical and practical aspects related to biomaterials decontamination in dental medicine (with reference to dental prosthetics). Metalurgia International. 2013;18(4):261-267.
- Mocuta D, Popovici LR, Dumitriu AS, Burlibaşa L, Ionescu CA, Sfeatcu R. Life quality-condition of social welfare. Metalurgia International. 2009;14:62-64.
- Burlibaşa M, Muntianu L, Tănase G, Bucur MB, Comes CA, Ionescu CA. Study on microbial contamination of biomaterials in medical practice. Metalurgia International. 2010;15(Spec. Issue No. 2):163-166.
- Ispas DC, Eftene OA, Burlibaşa M, Bucur MB, Tănase G, Cristache CM. Implications of titanium in orthodontics and dental facial orthopedics. Metalurgia International. 2011;16(10):72-74.
- Tănase G, Burlibaşa M, Muntianu L, Simion I, Bucur MB, Ionescu CA. Testing the antibacterial potential of biomaterials in medical practice. Metalurgia International. 2010;15(Spec. Issue No. 2):160-162.
- Burlibaşa M, Tănase G, Muntianu L, Murgu AI, Teodorescu E, Maliţa C. Quality of life, a multidisciplinary concept with economic and social impacts in medical practice. Metalurgia International. 2010;15(Spec. Issue No. 4):88-90.
Articole din ediţiile anterioare
INTERDISCIPLINARY | Ediţia 2 59 / 2023
Technological aspects in the reconstruction of the dental abutment with post and core restoration using the indirect method: modern versus digital
Camelia Ionescu, Andreea-Elena Vrabie, Radu Cătălin Costea, Viorel Ştefan Perieanu, Manuela Popescu, Mădălina Violeta Perieanu, Liliana Burlibaşa, Ileana Ionescu, Mihai Burlibaşa
Pierderea unei cantităţi semnificative de ţesuturi dure dentare de la nivel coronar impune utilizarea unui dispozitiv coronoradicular pentr...
30 mai 2023
INTERDISCIPLINARY | Ediţia 1 62 / 2024
Clasic versus digital în realizarea infrastructurii metalice a restaurărilor protetice fixe (Partea a II-a)
Mihai David, Dorina-Mihaela Gheciu, Radu Cătălin Costea, Viorel Ştefan Perieanu, Daniela‑Aurelia Pîrvu, Mircea Popescu, Irina Adriana Beuran, Florentina Căminişteanu, Bogdan Alexandru Dimitriu, Mihai Burlibaşa
Atât metoda clasică de confecţionare a instrastructurii metalice a restaurărilor protetice fixe metaloceramice, cât şi tehnologiile digitale mod...
20 februarie 2024