The Romanian guide for the assessment of vitamin D during pregnancy, in infants or preschool children, underlines the personalization of vitamin D therapy in obese children, after measuring the plasma level. Materials and method. It was conducted a study to identify if there were any differences in nutrition, supplemental vitamin D administration and exposure to sunlight of children aged between 3 and 6 years old, from three kindergartens. Results. One hundred sixty children were analyzed. The optimal serum level of vitamin D (25(OH)D) is 40-70 ng/mL, and a level above 30 ng/mL is considered sufficient. This study revealed a low awareness among parents on the necessity of achieving a physiological level of vitamin D. Most children improved their endogenous production during the summer holidays, because in the wintertime they spent an average of 1.66 hour per day outdoor. Fish intake was low, with only three children reaching the recommended level. In 42.9% of the children, the supplementation with vitamin D was missing. No differences were noted regarding any of these lifestyle factors or in vitamin D therapy according to the weight categories. Discussion and conclusions. This study shows a rather good sunlight exposure during summer, however not sufficient to assure the necessary level of vitamin D during the whole year. The personalization of vitamin D therapy in obese children should be better communicated by healthcare providers in order to correspond to the current guidelines recommendations.
Aportul de vitamină D şi starea greutăţii la copiii preşcolari
Vitamin D intake and weight status in preschool children
First published: 03 decembrie 2021
Editorial Group: MEDICHUB MEDIA
DOI: 10.26416/Pedi.64.4.2021.5788
Abstract
Rezumat
Ghidul privind evaluarea şi terapia deficitului de vitamină D la gravide, nou-născuţi şi la copiii preşcolari subliniază importanţa abordării personalizate a copilului obez, prin dozarea vitaminei D. Materiale şi metodă. S-a efectuat un studiu pentru a identifica diferenţele în dietă, suplimentarea cu vitamină D şi expunerea la soare a copiilor în vârstă de 3-6 ani din trei grădiniţe. Rezultate. Au fost analizaţi 160 de copii. Nivelul optim seric ideal al vitaminei D (25(OH)D) este de 40-70 ng/mL, peste 30 ng/mL fiind considerat suficient. Datele obţinute arată un nivel scăzut de conştientizare privind necesitatea de a avea un nivel fiziologic de vitamină D. Majoritatea copiilor îşi îmbunătăţesc sinteza endogenă în timpul vacanţei de vară, în timp ce iarna petrec, în medie, 1,66 ore pe zi afară. Consumul de peşte a fost scăzut în rândul copiilor incluşi în studiu, doar trei dintre ei atingând nivelul recomandat. Suplimentarea cu vitamină D a lipsit la 42,9% dintre copii. Nu s-au constatat diferenţe semnificative statistic pentru niciun element legat de stilul de viaţă şi nici pentru terapia cu vitamina D în funcţie de statusul ponderal. Discuţie şi concluzii. Acest studiu arată o expunere destul de bună la lumina soarelui în timpul verii, însă insuficientă pentru a asigura nivelul necesar de vitamină D pe tot parcursul anului. Personalizarea tratamentului cu vitamină D la copiii obezi trebuie comunicată mai bine de către cadrele medicale aparţinătorilor, pentru a implementa corect ghidul actual.
Introduction
Vitamin D is important for the children’s development and the parents’ awareness regarding the vitamin D sources is important to assure the necessary level for a harmonious growth. The level of vitamin D in the Romanian population is too low and young mothers are the risk category groups(1). This makes infants and children start their life trajectory with an insufficient reserve. The lack of awareness leads not only to a personal intake below the one recommended during pregnancy(2), but prolonged during the postnatal developmental period of their children.
Vitamin D is important for bone metabolism and for a myriad of other immunological and nonimmunological effects. The rapid periods of growth that characterize the pediatric age and the insufficient intake and internal production of vitamin D metabolites can have a significant impact. Vitamin D participates in the defense mechanisms against pathogens, mitigates the inflammatory, allergic and/or autoimmune response, and has a certain role in the reduction of the cancer risk(3). Children with vitamin D insufficiency have a higher risk of allergy(4) and have more severe infections(5), besides the classical skeletal effects on bone health.
Several studies have shown that 25-OH vitamin D (25(OH)D) plasma level (the currently accepted method to evaluate the vitamin D status)(6) reflects the balance between production, absorption, transport, distribution, utilization and catabolism. The ideal level of 25(OH)D is 40-70 ng/mL; however, more than 30 ng/mL is considered a sufficient level(7,8). The prevalence of optimal value reaches only 33.7% of children under 6 years old, even in developed countries(9). In a study performed by Voortman et al.(9), which inluded 4167 children, vitamin D was significantly lower in under-weight compared to normal-weight children, even after the adjustment for sociodemographic (e.g., ethnicity, economical status) and lifestyle determinants (e.g., exposure to sunlight, indoor activities). Other studies have found low vitamin D levels in obese children(10), these finding being explained as the result of a poor diet which does not fulfill the micronutrient requirements despite a high caloric intake. Therefore, an adaptation of vitamin D to the weight status is recommended in some countries(11), including in the Romanian legislation(12).
As deficiency was reported in both wasted and obese children, we have conducted an observational cross-sectional study to identify if there are lifestyle factors that influence the vitamin D status which might be different according to the weight categories in preschooler children.
Materials and method
A survey was conducted in three kindergartens from Bucharest and distributed to the parents. The questionnaire was intended to assess the sun exposure and the awareness on vitamin D sources. It included items such as time spent outdoor during different seasons, the intake of vitamin D supplements, or food fortified in vitamin D. There were also some items related to the awareness on the food content of vitamin D.
A section of the questionnaire was dedicated to height and weight data. The Body Mass Index (BMI) was calculated according to the following formula: BMI = weight (kg) ÷ height2 (m). The classification in BMI categories (obese/overweight/normal/wasted/severely wasted) was based on the WHO charts(13). Based on these data, we have estimated if the child was at risk of vitamin D deficiency. Secondly, we checked if there were differences in sun exposure and diet intake according to BMI status.
Data were processed with SPSS software. The numerical data were compared with the Kruskal-Wallis test and the categorical ones were compared using the chi-square test. The statistically significant level was set for a 95% probability.
Results
We received questionnaires from 160 parents out of 500, which represented a 32% rate of responses.
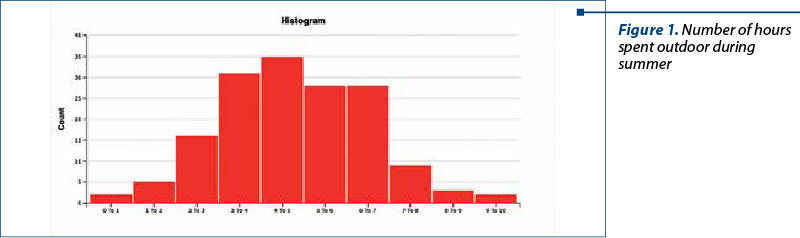
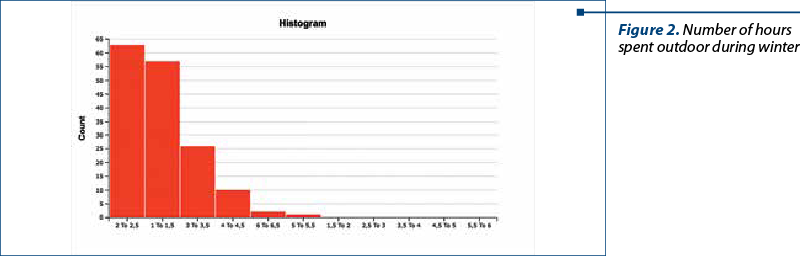
The average child’s age was 4.62 years old. The majority of the children had normal BMI (73%), 5% were severely wasted, 14% were wasted, 6% were overweight, and 2% were obese. On average, children spent outside 4.33 hours per day during the summer and 1.9 hours per day during winter (Figure 1 and Figure 2). There was no statistically significant difference noted among BMI categories, neither in summer (H=0.17, p=0.92), nor during wintertime (H=0.98, p=0.61), although overweight and obese children spent, on average, less time outside (4.16 hours per day during summer and 1.66 hours per day during winter).
The lack of exposure to sunlight in winter was partially compensated in most of the children (90.1%) with an average of 8.9 days per year of holidays at the seaside. The majority (63%) of the children spent between 7 and 13 days per year. Twenty-eight percentage spent less than seven days, and 9% had holidays longer than 14 days per year at the seaside.
Only 135 children ate fat fish at least once a month (average intake = 360 g/month). Apparently, the underweight children ate more fish (average intake = 467 g/month) than normal weight (average intake = 323 g/month) and overweight children (average intake = 368 g/month).
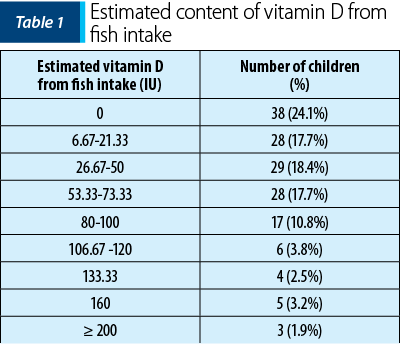
However, the difference was not statistically significant (H=2.17, p=0.34). The distribution and the estimated vitamin D intake are presented in Table 3. The total recommended dietary intake of vitamin D for children aged 1-17 years old is 600 UI/day(14). Unfortunately, natural foods are not very rich in these micronutrients. Fatty fish has the highest natural content of vitamin D(15). If we estimate that one-third of the total intake of vitamin D comes from fish, only three children have a sufficient level in their diet.
The distribution and the estimated vitamin D intake are presented in Table 1. As noticed, only three children had fish intake as recommended; one child had normal weight and the other two were overweight. Only 12 parents correctly identified a food that contains vitamin D and five others mentioned cereals as food with a high content of vitamin D, most probably referring to breakfast cereals that are supplemented with vitamin D.
In total, 73 children received vitamin D as a supplement. There was a high heterogeneity in the administration of the vitamin D, ranging from daily (15 children) to 10 days per month (one child), 6-8 months per year (28 children), four months per year (two children), three months per year (seven children), and two months/year (two children). Eleven parents did not specify the length of the administration. This might reflect a lack of communication with the healthcare professionals, but also some ambiguity and no consensus inside the medical community.
Even though the dosage were correct, 42.9% of the children would be at risk of not achieving the target for vitamin D and for becoming deficient in this essential element for growth and development. Worth mentioning, the three children who had a recommended intake of fish also received vitamin D as a supplement during winter.
Comparing according to BMI the children who received vitamin D as a supplement, 38.09% were underweight, 45.6% had a normal weight, and 33.33% were overweight. This distribution was also statistically insignificant (chi2=0.96, p=0.62).
Discussion
The prevalence of vitamin D insufficiency or even deficiency in the first decade of life is around 35% in Romania(16). Our figures show a rather good sunlight exposure during summer, however not sufficient to assure the necessary level of vitamin D during the whole year. In winter, the levels of vitamin D decrease significantly(17) and less than 2 hours per day (as found by us) of exposure of the face to sunlight would definitely not be enough for endogenous production. The direct relation between playing outdoor and the vitamin D levels, and the inverse relationship between the number of hours of watching television and the vitamin D levels were found in other studies(9) and should be subject to appropriate messages to parents, in order to improve as much as possible the sunlight exposure from June to September.
Diet and supplements were also insufficient to meet the requirements of vitamin D intake. The therapy was administered in very different schemes by the parents and most of them did not follow a clear medical recommendation. The awareness about foods with high content of vitamin D was very low and so was the fish consumption.
The most important finding of this study is that obese and overweight children do not benefit from a special approach, as recommended by the Romanian guideline. No statistical differences were recorded regarding sunlight exposure, fish intake and vitamin D therapy which makes the guideline recommendation inefficient in terms of implementation. Of course, this is not a study representative for the whole Romanian population and in other communities the personalized approach might be better. It is, however, a signal that not all children receive the proper treatment and this treatment does not follow a plasma measurement of 25(OH) vitamin D.
In terms of clinical attitude, it is to underline that the lower level of vitamin D in obese children is also a consequence of a volumetric dilution and of its liposolubility which produces adipose tissue sequestration(18), and the plasma level would not reflect as accurately the body content of vitamin D as it does for the normoponderal subjects. On the other hand, bone metabolism seems to be more impaired in obese girls than in obese boys(19). Therefore, the optimal solution would be to first restore the normal body weight, and only if there is no improvement in the vitamin D level, to correct it therapeutically.
In conclusion, there is no differentiation regarding the vitamin D intake (either from diet, or from therapy) and the exposure to sunlight according to the BMI status. A personalized recommendation of vitamin D for different BMI categories provides benefits for children’s growth and development. The implementation of the national guideline needs a better partnership between healthcare providers and parents in order to achieve the recommendations for obese children.
Conflict of interests: The authors declare no conflict of interests.
Bibliografie
-
Zugravu C, Tarcea M, Soptica F, Cucu A. Pertinence of Vitamin D supplementation in the adult Romanian population. Farmacia. 2016;64:467-720
-
Zugravu C, Raşcu A, Oţelea MR, Macri A. Vitamin D from food and supplement intake in pregnancy. A pilot study. Farmacia. 2020;68:150-154.
-
Bischoff-Ferrari HA, Giovannucci E, Willett WC, Dietrich T, Dawson-Hughes B. Estimation of optimal serum concentrations of 25-hydroxyvitamin D for multiple health outcomes. Am J Clin Nutr. 2006;84(1):18-28.
-
Neeland MR, Tursi AR, Perrett KP, Saffery R, Koplin JJ, Nadeau KC, Andorf S. Vitamin D insufficiency is associated with reduced regulatory T cell frequency in food-allergic infants. Pediatr Allergy Immunol. 2021;32(4):771-775.
-
Shah K, Varna VP, Pandya A, Saxena D. Low vitamin D levels and prognosis in a COVID-19 pediatric population: a systematic review. QJM. 2021;114(7):447-453.
-
Holick MF. Vitamin D status: measurement, interpretation, and clinical application. Ann Epidemiol. 2009;19(2):73-78.
-
Vasquez A, Manso G, Cannell J. The clinical importance of vitamin D (cholecalciferol): a paradigm shift with implications for all healthcare providers. Altern Ther Health Med. 2004 Sep-Oct;10(5):28-36; quiz 37, 94.
-
Weydert JA. Vitamin D in Children’s Health. Children (Basel). 2014 Sep 12;1(2):208-26.
-
Voortman T, van den Hooven EH, Heijboer AC, Hofman A, Jaddoe VW, Franco OH. Vitamin D deficiency in school-age children is associated with sociodemographic and lifestyle factors. J Nutr. 2015;145(4):791-798.
-
Bindayel IA. Effect of age and body mass index on vitamin D level in children with asthma in Riyadh. Sci Rep. 2021;11(1):11522.
-
Zakharova I, Klimov L, Kuryaninova V, et al. Vitamin D Insufficiency in Overweight and Obese Children and Adolescents. Front Endocrinol (Lausanne). 2019 Mar 1;10:103.
-
Ministerul Sănătăţii. Ghid privind evaluarea şi terapia deficitului de vitamină D la gravidă, nou-născut şi copil. Monitorul Oficial, nr. 773 din 24 septembrie 2019.
-
de Onis M (coord.). WHO child growth standards. Available at: https://www.who.int/publications/i/item/924154693X).
-
EFSA Panel on Dietetic Products, Nutrition and Allergies), 2016. Scientific opinion on dietary reference values for vitamin D. EFSA Journal. 2016;14(10):4547.
-
Schmid A, Walther B. Natural vitamin D content in animal products. Adv Nutr. 2013 Jul 1;4(4):453-62.
-
Chiriţă-Emandi A, Socolov D, Haivas C, Calapiş A, Gheorghiu C, Puiu M. Vitamin D Status: A Different Story in the Very Young versus the Very Old Romanian Patients. PLoS One. 2015;10:e0128010.
-
Ene MC, Tertiu O, Vrâncianu O, Chifiriu MC. Vitamin D status in adult and pediatric romanian population. Roum Arch Microbiol Immunol. 2018;77:198-212.
-
Vranić L, Mikolašević I, Milić S. Vitamin D Deficiency: Consequence or Cause of Obesity?. Medicina (Kaunas). 2019;55(9):541.
-
Pimentel D, Suttkus A, Vogel M, Lacher M, Jurkutat A, Poulain T, Ceglarek U, Kratzsch J, Kiess W, Körner A, Mayer S. Effect of physical activity and BMI SDS on bone metabolism in children and adolescents. Bone. 2021;153:116131.
Articole din ediţiile anterioare
Abordare practică în sindromul de apnee de somn de tip obstructiv la copil
Sindromul de apnee de somn de tip obstructiv (SASO) aparţine grupului de patologii respiratorii legate de somn, cu o prevalenţă în pediatrie...
Intervenţii actuale eficiente în imunitatea copilului
Sistemul imunitar este confruntat cu multiple provocări infecţioase la vârstă mică. De cele mai multe ori ineficient, în timp se dobândeşte imunita...
Factori legaţi de stilul de viaţă pentru obezitatea infantilă în preadolescenţă
Supraponderalitatea şi obezitatea sunt definite ca acumularea anormală sau excesivă de grăsime, care prezintă un risc pentru sănătate. Obezitatea a...
The importance of microbiome in pediatric obesity
Copilăria implică aspecte privind intervenţii ce configurează microbiomul pentru a atenua tulburările legate de obezitate.