Functional constipation is a common problem among the children of all age and generally resolves with changes in diet or behavior or sometimes with specific medication. Functional constipation in children has a pathophysiology that involves many factors. Often, avoiding defecation follows a painful bowel movement or a difficult colonic transit time. Some data showed that functional constipation may be related to genetic factors, low socioeconomic status, affected mobility or poor fiber intake. Regarding diet association, constipation is more frequently seen in children with low fruit, vegetables and cereal daily intake. The present guideline for the management of pediatric patients with functional constipation provides a synthetic opinion upon evaluation and treatment possibilities. Nowadays we cannot manage children’s constipation only by medication, but there is a gap between clinical practice and scientific evidence considering lifestyle and diet benefits.
Constipaţia funcţională – importanţa dietei pentru populaţia pediatrică
Functional constipation – the importance of diet in the pediatric population
First published: 30 septembrie 2021
Editorial Group: MEDICHUB MEDIA
DOI: 10.26416/Pedi.63.3.2021.5480
Abstract
Rezumat
Constipaţia funcţională reprezintă o afecţiune întâlnită frecvent în rândul copiilor de toate vârstele, a cărei evoluţie impune în general modificări ale dietei sau ale stilului de viaţă, utilizând sau nu medicaţie specifică. Fiziopatologia constipaţiei funcţionale pediatrice implică numeroşi factori. Frecvent, evitarea defecaţiei este urmarea unei experienţe anterioare dureroase sau secundară unui timp prelungit de tranzit colonic. Unele studii etiologice au indicat implicarea factorilor de ordin genetic, socioeconomic, privind nivelul de efort fizic şi mobilizare zilnică, dar şi aportul scăzut de fibre. În ceea ce priveşte implicarea dietei, constipaţia este mai frecvent observată la copiii cu un aport zilnic scăzut de fructe, legume şi cereale. Ghidul actual privind managementul pacienţilor pediatrici cu constipaţie funcţională oferă o opinie sintetică asupra posibilităţilor de evaluare şi tratament. În prezent, nu putem controla constipaţia copiilor doar prin medicaţie specifică şi există o diferenţă între practica clinică şi dovezile ştiinţifice cu privire la beneficiile stilului de viaţă şi ale dietei.
Introduction
Functional constipation is one of the most common disorders in Western countries and, in most cases, parents are worried that the child’s stools are too large, too hard, painful or too infrequent. The prevalence is estimated at a rate of 3% worldwide(1) and the very beginning of the symptoms occurs in the first year of life for about 17% to 40% of patients(2).
The normal frequency of bowel movements at different ages has been defined. This frequency gradually declines to a mean average of 1.7 stools per day at 2 years of age and to 1.2 stools per day at 4 years of age. Some normal breastfed babies do not have stools for several days or longer. After 4 years old, the frequency of bowel movements remains unchanged(3). Anal sphincter voluntary control is achieved in 98% of children by the age of 4 years old(4).
Since most constipated pediatric patients do not have an underlying condition, we use the Rome IV criteria to define and classify functional constipation(5) and, thus, the treatment does not require a specific intervention. Functional constipation in children has a pathophysiology that involves many factors. Often, avoiding defecation follows a painful bowel movement or a difficult colonic transit time. Some data showed that functional constipation may be related to genetic factors, low socioeconomic status, affected mobility or to poor fiber intake(6). Regarding diet association, constipation is more frequently seen in children with low fruit, vegetables and cereal daily intake(7,8).
Pathophysiology
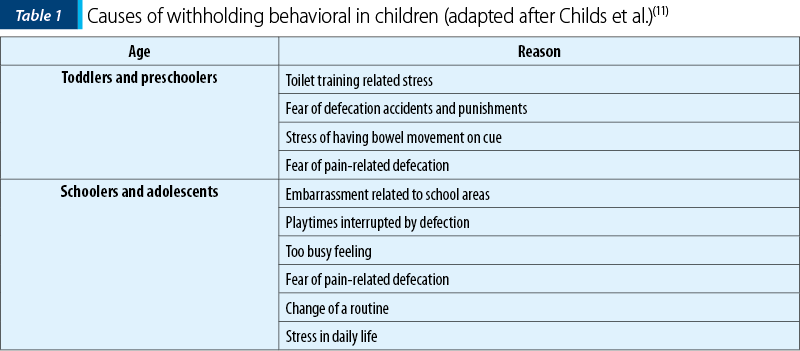
Functional constipation is related to a previous painful defecation, a particular colonic transit with increased orocecal time, infant dyschezia and diet(9). One of the most important causes is a painful event associated with defecation that eventually leads to voluntarily withhold feces in order to avoid unpleasant defecation(10). The most common reasons for withholding are presented in Table 1.
Colonic wall muscles or any disfunction of the nervous system is generally associated with a prolonged transit time from oral cavity to cecum. This event might also be secondary to previous volume masses due to fecal retention or as a consequence of immature Cajal cells in the sigmoid colon that normally stimulate an electrical wave of contraction(12,13).
Rome IV criteria define infant dyschezia as related to immaturity of infant’s coordination between the increased intraabdominal pressure and the relaxation of the pelvic floor(9). This is a normal condition that gradually resolves with age.
Traditionally, diet is regarded as an underlying factor of colonic motility. The initiation of complementary feeding, low liquid intake and inadequate fiber consumption are associated with functional constipation. There is a great concern regarding dietary influence on bowel movements, for both parents and pediatricians. The management classically involves a combination of the three classical “Fs”: fluids, fibers and fruits.
Fibers
The ingested fibers are fermentable but nondigestible carbohydrates. The recommendation regarding children daily needs for those aged over 1 year old consists in adding “5-10 g” to the children age or “0.5 g/kg”(14).
The most important dietary fiber sources are cereals (rice, corn), bread, vegetables, fruits, potatoes and whole grains. They act in the gastrointestinal tract through: a) acceleration of the colon transit, b) increasing the osmotic load of the gastrointestinal tract by production of short chain fatty acids (butyrate, propionate, acetate etc.), c) decreasing intraluminal pH by short chain fatty acids and d) water content(15).
The classification of dietary fibers includes water-soluble and water-insoluble fibers. In the first category, there are gums (fenugreek gum, guar gum, tara gum, locust bean gum, or carob gum), pectin, mucilage, psyllium and glucomannan. The second one includes cellulose, hemicellulose, methylcelluose, lignin and synthetic fibers (calcium polycarbophil). Another classification based on biochemical composition concludes two types of fibers: 1) short-chain carbohydrates are represented by oligosaccharides, 2) long-chain carbohydrates which follow the classification:
A: Soluble, highly fermentable non-starch polysaccharides fibers that include resistant starch, pectin, inulin and guar gum.
B: Intermediate soluble and fermentable fibers that include psyllium, ispaghula and oats.
C: Insoluble, slowly fermentable fibers that include wheat bran, lignin (flax) and fruits and vegetables.
D: Insoluble, nonfermentable fibers that include cellulose, sterculia and methylcellulose(16).
Not all fibers act the same: water insoluble fibers are more indicated in constipation, and some authors empowered intermediated soluble and fermentable fibers in constipation, while water-soluble fibers (psyllium and glucomannan) are considered by the North American Society for Pediatric Gastroenterology, Hepatology and Nutrition (NASPGHAN) and by the European Society for Pediatric Gastroenterology, Hepatology and Nutrition (ESPGHAN) not suitable to use in the treatment of functional constipation(17). Another study showed limited effect of additional fibers in constipation compared to placebo and the effect was anyway far less intense than that of lactulose(18).
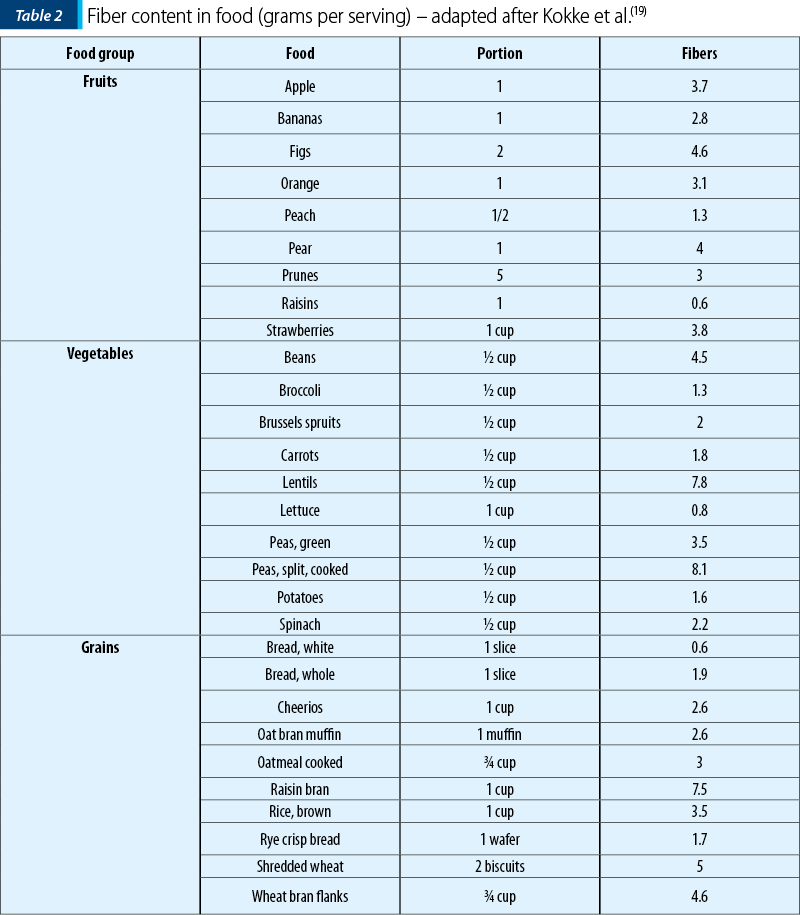
The amount of non-starch polysaccharide content of food should be considered in order to prescribe a diet (Table 2).
Several epidemiological and clinical studies have been conducted to demonstrate the effectiveness of fiber consumption in chronic constipation. Epidemiologic studies have reported a negative correlation between the incidence of chronic constipation and the per capita fiber intake in various countries, but another clinical study has reported a successful management of chronic constipation with fiber supplementation(3). In this case control study, the possibility of the correlation of idiopathic chronic constipation in children and the dietary intake – particularly, fiber intake – was evaluated.
A randomized sample of children aged 2 to 14 years old was taken from 3 of the 52 counties of Greece(20). The stratification was performed on the basis of urban, rural or suburban location and socioeconomic status(20). Two hundred ninety-one children were considered to be chronically constipated, who had three or fewer bowel movements per week or hand stools with painful defecation (even with more than three bowel movements per week) at least during the past two months, and the remaining 1602 children were the control subjects(20).
Also, the relation of fiber components to chronic constipation was studied. It was found that constipated children had lower cellulose, uronic acid, pentose and exose intake. The conclusion was that the lack of fiber plays an important role in the etiology of chronic idiopathic constipation in children and it should be supplemented to these patients.
Fluids
The total amount of liquids manipulated by the adult gastrointestinal tract is around 10 L per day, out of which 2 L come from the diet, and the rest of 8.5 L are absorbed by the small intestine. In children, the gastrointestinal fluid load is about 5 L per 24 hours. The absorptive capacity of the small bowel and colon is an evolving age-dependent process(21). The aforementioned guideline concluded that there is no evidence to support the use of extra fluid intake to treat functional constipation(17).
Studies with polyethylene glycol showed that bowel movement frequencies and consistency can be improved by adding fluid supplements because osmosis process needs water(22). Adding small amounts of fruit juices, like apple, prune and pears, helps due to their fiber content.
In a Japanese study aimed to correlate the diet with functional constipation (FC), the univariate analysis revealed that water intake, meal weight/100 kcal, water content per meal/100 kcal, magnesium intake/100 kcal, dietary fiber intake/100 kcal and sodium chloride intake/100 kcal were all significantly lower in the FC group compared to the non-FC group, whereas the intake of juice was significantly higher(23).
Probiotics and prebiotics
Probiotics are live microorganisms that confer a health benefit on the host when administered in adequate amounts. As most studies involving probiotics, the results have opposite findings sometimes. For example, Bifidobacteria species (B. bifidum, B. infantis and B. longum) and Lactobacillus species (L. casei, L. plantarum and L. rhamnosus) were showed to decrease the fecal incontinence, increase bowel movement frequency and reduce the abdominal pain in children with the age of 4-16 years old, but stool consistency was not improved(24). Most studies used the probiotic Lactobacillus reuteri (DSM 17938) once per day for eight weeks. Infants treated with L. reuteri had a significantly higher defecation frequency than placebo after two, four and eight weeks of treatment. This was the strain used in the ESPGHAN guideline and the experts concluded that the evidence does not support the use of prebiotics or probiotics in the treatment of childhood constipation(17). Nevertheless, considering the pathology of constipation in children with documented dysbiosis, future investigational processes should reconsider using special strains for children constipation.
There are many potential mechanisms involved in probiotics action in constipation: a) the capacity of decreasing the luminal pH by Bifidobacteria and lactobacilli production of lactic acid, acetic acid and other acids; 2) the motility enhance due to the antiinflammatory effect and immunomodulation effect; 3) the metabolic effect of probiotics induces gas production. We nowadays use some probiotic strains for constipation and some for various types of diarrhea, but the actual 2014 NASPGHAN and ESPGHAN guideline does not support the use of probiotics, nor prebiotics, in the treatment of children constipation(17).
Fruits
Prokinetic fruits effect is explained by its content in water, sorbitol, fructose, fiber and phytochemicals. With classical diet recommendation, that bring a supplementation of fibers and fruits, the total amount of carbohydrates also rises in these children. Green kiwi fruit has a high concentration of fibers (2-3 g of dietary fiber per 100 g), it is rich in enzyme (actinidine – a protease that stimulates upper gastrointestinal tract motility) and it contains anion selective peptides(25). Other ancestral fruits used in constipation are plums, due to their fiber content (6.1 g/100 g), fructose composition (fructan), sorbitol amount (14.7 g/100 g) and phenolic structure (184 mg/100 g). Prune juice is less rich in these nutrients(26).
Diary and milk
In infancy, stool consistency depends mostly on the milk intake. For breastfed infants, stools are more frequent and loose due to human milk fat content, to prebiotic oligosaccharides that serve as a substrate for gut bacteria, improving osmotic balance and stool consistency, due to low phosphorous content, and due to optimal whey protein composition(27). Additionally, in formula fed infants, there is a higher level of gastric inhibitory peptide, neurotensin, and vasoactive intestinal peptide.
Special diets
Constipation can occur during infancy and the patients frequently use natural remedies before going to a specialist. These remedies are designed to ease the act of defecation. For example, in infants we can use, after six months, high-fiber foods (plums, beans, peas, broccoli, apricots, sweet potatoes, pears) in the form of purees or mixed with cereals.
The Mediterranean diet is regarded as a dietary model in the scientific literature(28). Its benefits upon a healthy life are due to a preventative effect on some diseases such as cardiovascular conditions, metabolic diseases and various types of cancers(29). It was stipulated that the Mediterranean diet may prevent and improve some functional gastrointestinal symptoms due to its high fiber and antioxidant levels and to low saturated fatty acids and oligosaccharides. A Greek study revealed important data regarding the lower prevalence of constipation in children with a high adherence to the Mediterranean diet, consuming large amount of cereals, olive oil, fruits and vegetables, along with water and milk products(30).
Conclusions
Functional constipation is often an embarrassing condition for both pediatric patients and parents. The adherence to a healthy lifestyle in terms of physical activity, encouraging water intake, and fulfill the normal amount of dietary fibers may be the key to assure compliance. Nowadays, we cannot manage children constipation only by medication, but there is a gap between clinical practice and scientific evidence considering lifestyle and diet benefits.
Conflicts of interests: The authors declare no conflict of interests.
Bibliografie
-
van den Berg MM, Benninga MA, Di Lorenzo C. Epidemiology of childhood constipation: a systematic review. Am J Gastroenterol. 2006;101:2401-9.
-
Loening-Baucke V. Constipation in early childhood: patient characteristics, treatment, and long-term follow up. Gut. 1993;34:1400–4.
-
Baker S, Liptak G, Colletti R, et al. Constipation in Infants and Children: Evaluation and Treatment. JPGN. 1999;29(5): 612-26.
-
Xinias I, Mavroudi A. Constipation in Childhood. An update on evaluation and management. Hippokratia. 2015;19(1):11–19.
-
Hyams JS, Di Lorenzo C, Saps M, Shulman RJ, Staiano A, van Tilburg M. Functional disorders: children and adolescents. Gastroenterology. 2016;S0016-5085(16)00181-5.
-
Mugie SM, Di Lorenzo C, Benninga MA. Constipation in childhood. Nat Rev Gastroenterol Hepatol. 2011;8(9):502–11.
-
Morais MB, Vitolo MR, Aguirre AN, Fagundes-Neto U. Measurement of low dietary fiber intake as a risk factor for chronic constipation in children. J Pediatr Gastroenterol Nutr. 1999;29(2):132–5.
-
Butte NF, Fox MK, Briefel RR, Siege-Riz AM, Dwyer JT, Deming DM, et al. Nutrient intakes of US infants, toddlers, and preschoolers meet or exceed dietary reference intakes. J Am Diet Assoc. 2010;110(Suppl. 12):S27–37.
-
Philichi L. When the going gets tough – pediatric constipation and encopresis. Gastroenterol Nurs. 2008;31:121-130.
-
Nurko S, Zimmerman LA. Evaluation and treatment of constipation in children and adolescents. Am Fam Physician. 2014;90:82-90.
-
Childs AA, John RM. Pooping Shouldn’t Be This Hard: Using Nutrition to Address Constipation in Primary Care. Infant, Child & Adolescent Nutrition. 2015;7(5):287-302.
-
Benninga MA, Voskuijl WP, Taminiau JA. Childhood constipation: is there new light in the tunnel? J Pediatr Gastroenterol Nutr. 2004;39:448-64.
-
He CL, Burgart L, Wang LN. Decreased interstitial cell of Cajal volume in patients with slow-transit constipation. Gastroenterology. 2000;118:14-21.
-
Food and Nutrition Board, Institute of Medicine. Dietary reference intakes for energy, carbohydrates, fiber, fat, fatty acids, cholesterol, protein, and amino acids. Washington, DC: National Academies Press, 2005.
-
Makki K, Deehan EC, Walter J, Bäckhed F. The Impact of Dietary Fiber on Gut Microbiota in Host Health and Disease. Cell Host Microbe. 2018;23(6):705-15.
-
Eswaran S, Muir J, Chey WD. Fiber and functional gastrointestinal disorders. Am J Gastroenterol. 2013;108:718-27.
-
Tabbers MM, DiLorenzo C, Berger MY, Faure C, Langendam MW, Nurko S, et al. Evaluation and treatment of functional constipation in infants and children: evidence-based recommendations from ESPGHAN and NASPGHAN. J Pediatr Gastroenterol Nutr. 2014; 58:258-74.
-
Tabbers MM, Boluyt N, Berger MY, et al. Constipation in children. BMJ Clin Evid. 2010;2010:0303.
-
Kokke FTM, Taminiau AJM, Benninga MA. The Role of Dietary Fiber in Childhood and Its Applications in Pediatric Gastroenterology. Nestlé Nutr Workshop Ser Pediatr Program. 2005;56:111-26, discussion 120-6.
-
Roma E, Adamidis D, Nikolara R, Constantopoulos A, Messaritakis J. Diet and Chronic Constipation in Children: The Role of Fiber. JPGN. 1999;28(2):169-74.
-
Bae SH. Diets for Constipation. Pediatr Gastroenterol Hepatol Nutr. 2014;17(4):203-8.
-
Bae SH, Son JS, Lee R. Effect of fluid intake on the outcome of constipation in children: PEG 4000 versus lactulose. Pediatr Int. 2010;52:594-7.
-
Asakura K, Masayasu S, Sasaki S. Dietary intake, physical activity, and time management are associated with constipation in preschool children in Japan. Asia Pac J Clin Nutr. 2017;26(1):118-29.
-
Bekkali NL, Bongers ME, Van den Berg MM, Liem O, Benninga MA. The role of a probiotics mixture in the treatment of childhood constipation: a pilot study. Nutr J. 2007;6:17.
-
Drummond L, Gearry RB. Kiwifruit modulation of gastrointestinal motility. Adv Food Nutr Res. 2013; 68:219-32.
-
Na JR, Oh KN, Park SU, Bae D, Choi EJ, Jung MA, et al. The laxative effects of Maesil (Prunus mume Siebold & Zucc.) on constipation induced by a low-fibre diet in a rat model. Int J Food Sci Nutr. 2013;64:333-45.
-
Quinlan PT, Lockton S, Irwin J, Lucas AL. The relationship between stool hardness and stool composition in breast- and formula-fed infants. J Pediatr Gastroenterol Nutr. 1995; 20:81-90.
-
Bach-Faig A, Berry EM, Lairon D, Reguant J, Trichopoulou A, Dernini S, et al. Mediterranean diet pyramid today. Science and cultural updates. Public Health Nutr. 2011;14(12A):2274–84.
-
Ramezan M, Asghari G, Mirmiran P, Tahmasebinejad Z, Azizi F. Mediterranean dietary patterns and risk of type 2 diabetes in the Islamic Republic of Iran. East Mediterr Health J. 2019;25(12):896–904.
-
Agakidis C, Kotzakioulafi E, Petridis D, Apostolidou K, Karagiozoglou-Lampoudi T. Mediterranean diet adherence is associated with lower prevalence of functional gastrointestinal disorders in children and adolescents. Nutrients. 2019;11(6):1283.
Articole din ediţiile anterioare
The impact of postnatal depression on the health and development of the newborn
Depresia prenatală şi postnatală reprezintă un factor de risc pentru buna dezvoltare a sugarului şi nou-născutului, cu repercusiuni care se întind ...
Incontinenţa fecală asociată constipaţiei – cum o putem evita?
Introducere. Incontinenţa fecală asociată constipaţiei (incontinenţă fecală funcţională retentivă – IFFR) reprezintă o problemă majoră, afectân...
Evaluarea funcţională a tractului digestiv inferior la copii – manometria anorectală
Manometria anorectală este o metodă obiectivă utilizată pentru examinarea funcţiei anorectale şi a sensibilităţii rectale. Scopul acestui studiu ...
Utilizarea suplimentelor cu vitamine în copilărie – necesitate sau abuz?
De-a lungul timpului, suplimentele cu vitamine au fost administrate copiilor de toate vârstele atât în scop profilactic, cât şi curativ. Din cauz...