The management of pregnancy associated with gestational hypertension is performed depending on the severity of the hypertension, according to gestational age and the presence or absence of complications. The early identification of worsening preeclampsia involves the prevention of maternal complications (eclampsia, HELLP syndrome, uteroplacental apoplexy) and of foetal complications (IUGR, foetal intrauterine death). The monitoring of the maternal-foetal evolution and the early identification of the worsening of preeclampsia determine the improvement of the vital and functional maternal-foetal prognosis in pregnancy-induced hypertension.
OBSTETRICS
Complicaţiile hipertensiunii arteriale induse de sarcină – management terapeutic şi prognostic
Complications of pregnancy-induced hypertension – therapeutic management and prognosis
First published: 04 decembrie 2020
Editorial Group: MEDICHUB MEDIA
DOI: 10.26416/Gine.30.4.2020.3943
Abstract
Rezumat
Managementul sarcinii asociate cu hipertensiune gestaţională se realizează în funcţie de severitatea hipertensiunii arteriale, de vârsta gestaţională şi de prezenţa sau absenţa complicaţiilor. Identificarea precoce a agravării preeclampsiei implică prevenirea complicaţiilor materne (eclampsia, sindromul HELLP, apoplexia utero-placentară) şi a complicaţiilor fetale (IUGR, moartea fetală intrauterină). Monitorizarea evoluţiei materno-fetale şi identificarea precoce a agravării preeclampsiei duc la îmbunătăţirea prognosticului vital şi funcţional materno-fetal în hipertensiunea arterială indusă de sarcină.
Introduction
Pregnancy-induced hypertension (PIH) is a complex condition which appears in the first weeks of gestation, the initial site being the area of impact between the placental trophoblast and the endothelium of spiral arterioles in the decidual maternal endometrium.
In addition, in the spiral arterioles there were significant destructions in the distal third with fibrin deposits and thrombi in their lumen, arterial wall infarctions, ruptures of vessels, aspects that confirm the conflict between vasoconstrictor substances (thromboxane A2, endothelin ET1) and vasodilators (nitric oxide, prostacyclin PG I2), a conflict that leads to vasospasm, initially in the uteroplacental territory, later extended throughout the maternal body(1,2).
This vasospasm leads to hypertension, proteinuria and generalized oedema. The kidney, liver, lung, heart and the maternal brain are affected.
PIH occurs only in gestation and disappears without sequelae in the first 12 weeks postpartum.
Regarding PIH, J.A. Pritchard (1984) considers that any of the cases must meet four requirements: the condition occurs in women exposed for the first time to chorionic villi, it manifests in women who have pregnancy with an abundance of chorionic villi (hydatidiform mole, twin or multiple pregnancy), it occurs in women with preexisting hypertensive disease, it is specific to overweight or obese women, genetically predisposed to the development of hypertension in pregnancy(3).
The pregnancy-induced hypertension may develop alone or in combination with generalized oedema and proteinuria (preeclampsia). Untreated, it can lead to complications: tonic-clonic seizures (eclampsia), severe uterine haemorrhages (uteroplacental apoplexy), intrahepatic hematoma with liver rupture (HELLP syndrome), cerebral haemorrhage, large vulvovaginal hematoma.
Pregnancy management associated with gestational hypertension is performed depending on the severity of hypertension, according to gestational age and the presence or absence of complications. The management of preeclampsia depends on the severity of endothelial injury and multiorgan dysfunction. The American College of Obstetricians and Gynecologists (ACOG) recommends more frequent prenatal monitoring of suspected cases of preeclampsia(4). The careful monitoring allows for the recognition of minor changes in blood pressure, critical laboratory investigations, and clinical signs and symptoms(5,6).
It was found that PIH can be found in 5-17% of nulliparous cases and in 2-5% of multiparous cases. Approximately 10-15% of the cases of maternal mortality in pregnancy are the consequence of hypertensive complications in pregnancy, these being among the first four causes of maternal mortality, after haemorrhage, cardiovascular diseases and thromboembolism(7-9).
The aim of this paper consists in the importance of monitoring the maternal-foetal evolution in case of pregnancies with associated hypertensive pathology, for the early identification of the aggravation of preeclampsia, the prevention of its complications and the improvement of the vital and functional maternal-foetal prognosis.
Method
The research was performed for a period of two years, between 2017 and 2018, in the 2nd Obstetrics-Gynaecology Clinic of the County Emergency Clinical Hospital of Craiova. A total of 122 cases were studied, of which: 93 cases of preeclampsia, 11 cases of eclampsia, 8 cases of uteroplacental apoplexy, 3 cases of HELLP syndrome, and 7 cases of voluminous vulvovaginal hematoma. There were 28 cases of IUGR and 11 cases of foetal death in utero.
All these cases were reported in a number of 1637 births in 2017 and 1629 births in 2018. The patients came from the territory of five counties: Dolj, Mehedinţi, Gorj, Olt and Vâlcea.
The pregnant women were in the third trimester of pregnancy and presented for a polymorphic symptomatology: painful uterine contractions, headache, vertigo, oedema in the last two weeks and exacerbated in the last 24-48 hours, vaginal bleeding, epigastric pain or in the upper abdominal floor.
The patients with preeclampsia (PE) and eclampsia (E) were hospitalized, investigated, monitored and the appropriate treatment was administered, particularly for the respective cases, having as objectives the prevention, respectively the treatment of convulsions, intracranial haemorrhages, severe injury of other vital organs and the birth of a healthy child.
The patients with HELLP syndrome and those with uteroplacental apoplexy were hospitalized, the therapeutic attitude and emergency investigations coming to the fore, in order to save the mother’s life.
The 122 patients investigated were studied regarding several parameters: age, environment, marital status, profession, obstetric and gynaecological history, investigations performed at the present pregnancy (haematological, urinary), explorations performed, such as maternal-foetal ultrasound and Doppler velocimetry, completion of pregnancy, the Apgar index, birth weight of the foetuses.
Results
During the two years included in the study, 3266 births were registered. Of the 3266 births, the 122 cases of complicated PIH analyzed represented a percentage of 3.7%
In our research, the complications induced by PIH were: PE – 93 cases (76.2%), E – 11 cases (9%), UPA – 8 cases (6.5%), HELLP syndrome – 3 cases (2.5%), voluminous vulvovaginal hematoma – 7 cases (5.8%).
By age groups, we found: 15-25 years old – 72 cases (59%), 26-35 years old – 34 cases (27.9%), 36-45 years old – 16 cases (13.1%). By residence, the patients were registered as follows: pregnant women from urban areas – 87 cases (71.3%), pregnant women from rural areas – 35 cases (28.7%). By marital status, we noticed: married patients – 81 cases (66.4%), unmarried patients – 41 cases (33.6%). By profession, 56 patients had a job (45.8%), and 66 were housewives (54.2%).
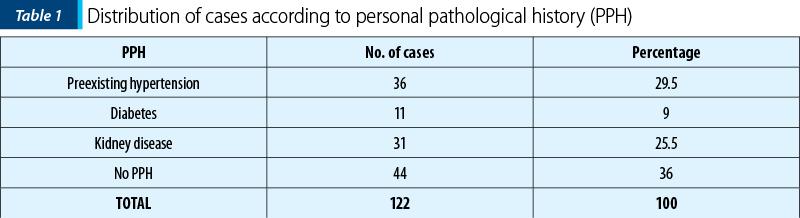
According to the personal pathological antecedents, we found: 36 cases (29.5%) with preexisting hypertensive disease; 11 cases (9%) with diabetes; 31 cases (25.5%) with kidney diseases such as glomerulonephritis, polycystic kidney, pyelonephritis, kidney stones or urinary tract infections (Table 1, Figure 1). Depending on the obstetric history, we found that 86 patients (77.1%) were nulliparous, and 36 cases (22.9%) had two or more births.
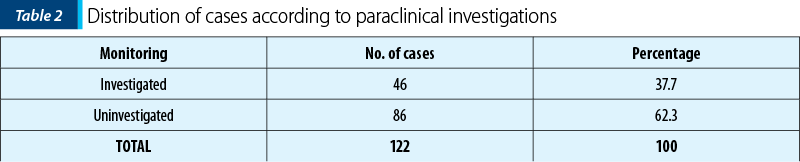
Regarding the outpatient investigations, 46 pregnant women (37.7%) had performed haematological, urinary or ultrasound investigations, 86 patients (62.3%) being uninvestigated (Table 2, Figure 2).
Upon admission to the County Emergency Clinical Hospital of Craiova maternity, the objective examination showed mild, moderate or severe oedema, facial or limb (Image 1). Blood pressure had values above 140/90 mmHg. The patients with severe preeclampsia showed an increase in systolic and diastolic blood pressure over 160/110 mmHg, proteinuria over 300 mg/24 hours, an increase in serum creatinine over 1.1 mg/dl, uricemia over 5.5 mg/dl, and an increase in liver transaminases over 70 UI/it. In three severe cases, we found massive proteinuria, from 5 g/l/24 hours to 11 g/l/24 hours. The coagulogram showed thrombocytopenia below 100,000/mm3, prothrombin time increased over 15 seconds, and haemolysis. The fibrinogen level below 300 mg/dl has been associated with increased fibrin degradation products and fibrin monomers.
The foetal biophysical score had special importance when PE was associated with IUGR, due to vasospasm in the uterine artery that causes chronic fetal distress and IUGR. In patients with PE and E, the foetal biophysical score was 8 in 86 cases (77.2%) and 6 in 25 cases (22.8%).

Doppler velocity in umbilical artery was suggestive. In cases of severe PE, the pulsatility and resistance indexes remain high due to UA spasm. Doppler velocity in uterine artery confirmed the foetal status in utero by increased pulsatility and resistance indexes. The abnormal flow consisted of a decrease in the end-diastolic component. The presence of notching (protodiastolic incision) means an increase in vascular resistance in the placenta. We found it rarely, especially when the severe PE with high blood pressure values was associated with IUGR (22.9%). Doppler velocimetry in MCA is important because it reveals foetal status in utero, the decreased indices of pulsatility and resistance meaning foetal hypoxia. The cerebroplacental ratio, the ratio between PI in MCA and PI in UA, was greater than 1.

The ophthalmological consultation highlighted retinal changes, such as: vasospasm, oedema, haemorrhage and retinal detachment in one case, changes that were remitted after the end of gestation. The neurological symptoms such as headache, vertigo, visual, speech, hearing disorders and vomiting of the central type required the specialized neurological consultation.
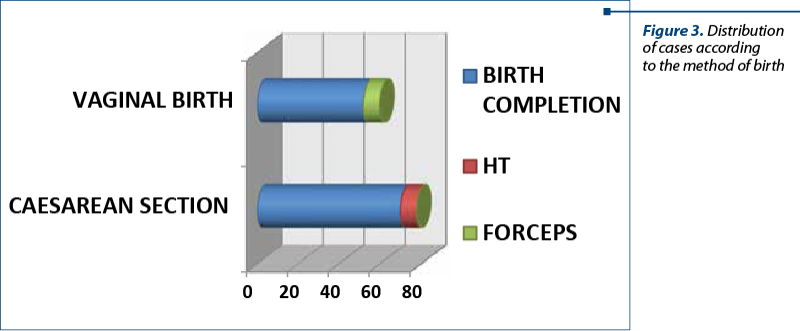
Of the 122 cases, 52 (48.4%) gave birth by natural means, of which in 8 cases the foetus was extracted by forceps (6.5%), and in 70 cases the foetus was extracted by caesarean section (57.6%) – Table 3 and Figure 3.
At vaginal birth, 7 cases of PIH developed voluminous vulvovaginal hematoma (Image 2). We mention that in the 8 cases of UPA following caesarean section, total extracapsular hysterectomy was performed with or without bilateral adnexectomy.

In the three cases of HELLP syndrome, we resorted to the help of on-call surgeons who applied the specific treatment. They mounted above and under the liver four soft fields soaked in NaCl 0.9%, the liver being compressed as in a sandwich, for haemostatic purposes, for 24 hours, the abdomen being closed. After 48 hours, the peritoneal cavity was reopened and the fields were suppressed. The area of upper- and under-hepatic haemostasis was assessed as very good.
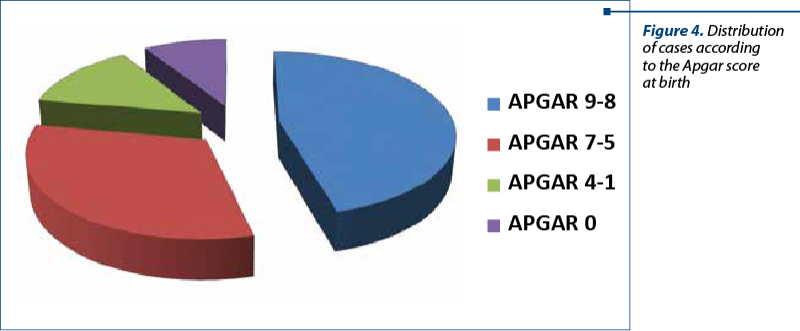
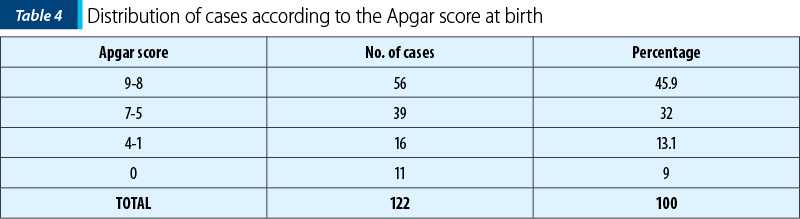
Regarding the Apgar score at birth, in 56 cases (45.9%) it was 8-9, in 39 cases (32%) it was 5-7, in 16 cases (13.1%) it was 1-4, and 11 newborns died intrauterine (9%) – Table 4 and Figure 4. The 11 cases of dead foetuses came from eight cases of UPA and from the three cases of HELLP syndrome.

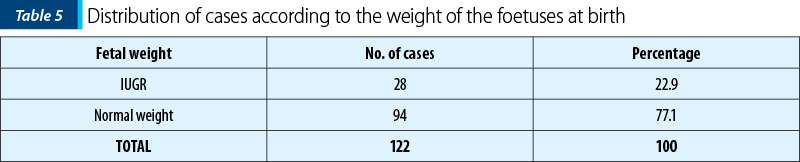
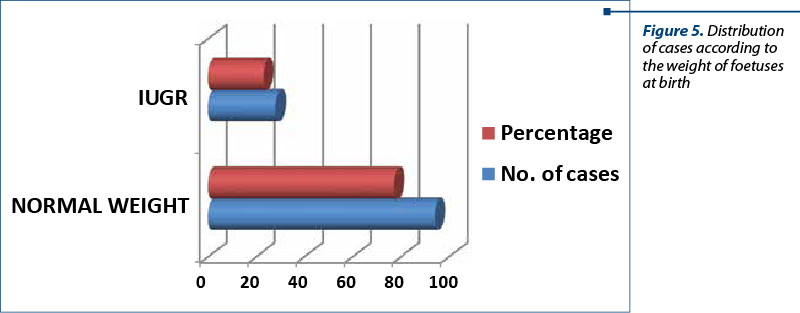
In 28 cases, the foetuses presented IUGR (22.9%), and the remaining 94 cases (77.1%) were normal weight (Table 5, Figure 5).
Discussion
PIH is a severe pathology in obstetrics, both through the maternal complications it causes (preeclampsia, eclampsia, uteroplacental apoplexy, HELLP syndrome, voluminous vulvovaginal hematoma), and through foetal complications (intrauterine growth restriction, foetal death in utero), major complications that endanger the life of the foetus and the mother.
The 122 complicated cases of PIH analyzed accounted for 3.7% of the total number of births.
By age groups, we found that patients aged 15-25 years old predominated (72 cases; 59%), which correspond to the data in the literature, this group including young primiparous whose decidua comes in direct contact for the first time with chorionic villi. Most of the cases came from urban areas (87 cases; 71.3%), which can be explained in terms of medical and social factors, stress, but also easier access to the consultation, investigations and ultrasound examination with Doppler velocimetry.
In maternity, as a hypotensive treatment there were administered Dopegyt®, Trinitrosan®, Tertensif®, Norvasc®, nifedipine, Enap®, as anticonvulsant – magnesium sulphate, and anticoagulant therapy(10-13). Intravenous diazepam was administered intravenously for the sedation of patients with eclampsia and for the prophylaxis of new tonic-clonic seizures.
Eclampsia along with uteroplacental apoplexy, uterine rupture and HELLP syndrome are major disorders in pregnancy(14-16). Eclampsia occurs against the background of severe untreated preeclampsia and is predominantly manifested by tonic-clonic seizure. In 50% of the cases, they appear antepartum, in 25% in labour, and the remaining 25% in postpartum(17). Eclamptic access occurs as a consequence of cerebral oedema, secondary to hypertension, and mimics epileptic access. The convulsive episode can be unique, especially when it occurs in advanced labor or after birth; sometimes the convulsions follow one another in 2-3 episodes or even more(1,18).
The cases with UPA were urgently hospitalized. They presented with severe acute haemorrhagic syndrome, in haemorrhagic shock, with dead foetus and placental detachment. The caesarean section was performed to save the mother’s life, extracting the recently dead foetus. The spontaneous delivery of the placenta through the hysterotomy incision highlighted the retroplacental hematoma, with a diameter of 5-10 cm, with red infarct areas of the placental maternal part. Intraoperatively, the uterus had multiple ecchymotic, purplish areas (Image 3). Under perfusion with oxiton (80-100 UI) and intramiometric administration (20-40 UI), the uterus was reactive, with appreciable bleeding. It was decided to continue the surgery after the caesarean operation, with total hysterectomy (Image 4). The fluid-coagulant changes already installed were managed by the administration of isogroup, isoRh transfusions.
The three cases of HELLP syndrome came from maternity hospitals in the Oltenia region, where they were hospitalized for blood pressure over 210/120 mmHg, frontal-occipital headache, vomiting, moderate pain in the upper abdominal floor, attributed to uterine contractions; although the patients were not in labor, there were symptoms on the basis of which the diagnosis of severe preeclampsia was established. After the administration of drug treatment with spasmolytic, hypotensive, magnesium sulphate, and left lateral decubitus, the general condition progressively altered, blood pressure dropped below 150 mmHg, the abdomen became very painful, predominantly in the upper floor and especially in the right upper quadrant. The patients were transferred to the maternity hospital of the County Emergency Clinical Hospital of Craiova. Median puboxiphoid laparotomy was performed, the recently deceased intrauterine foetuses were removed, the uteri were reactive, macroscopically normal, with tubules and ovaries of normal appearance. Approximately 400-850 ml of fluid, blood and clots were found in the peritoneal cavity. The spleen, stomach and intestine were intact, the right hepatic lobe was very bleeding, and the hepatic capsule was broken. For haemostasis, a compressive technique was performed by mounting four fields soaked in saline between the diagram and the liver and another four fields under the liver. Parietoraphy was performed in anatomical planes. Fluid-coagulation rebalancing with blood, plasma and antibiotic therapy was administered. After 48 hours postoperatively, surgery was performed to extract the fields and check the haemostasis. The compromised areas of the liver were covered with Gelaspon sponges. Parietorrhaphy was performed after the inspection of the uterus, appendages and abdominal viscera. The patients left the hospital after 14-20 days postoperatively, with the liver and genital area intact and the recommendation of a new pregnancy after at least three years.


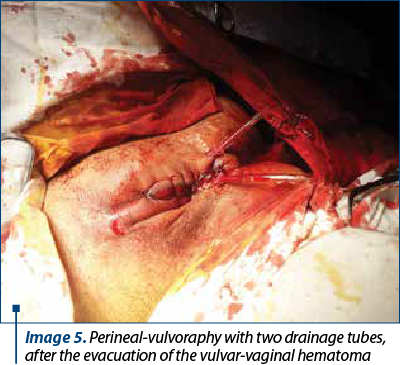
The voluminous vulvovaginal hematoma occurred in seven cases of natural births, of which in two parturients the foetuses were extracted in expulsion by forceps. Perineoraphy was performed after drainage tubes were left on each side of the vulva (Image 5). The postpartum evolution was good, the tubes being suppressed on the fourth day of evolution, in confinement after birth. The women who had given birth continued hypotensive treatment, antibiotic therapy, local anticoagulants and anti-inflammatory drugs.
The obstetric conduct at birth by caesarean section or vaginal way, with or without forceps, should be carefully chosen, so that not to obscure the maternal and foetal prognosis(19).
The vital maternal prognosis was good, and the functional one was relatively good. We refer in this situation to the cases of uteroplacental apoplexy where the total hysterectomy with or without bilateral adnexectomy was imposed, for saving the mothers’ lives.
The foetal prognosis was good in the foetuses with intrauterine growth restriction, and infaust in the 11 cases of antepartum stillbirths, referring to cases of uteroplacental apoplexy and HELLP syndrome.
Conclusions
Complicated PIH accounted for 3.7% of cases. Among the complications of PIH, the highest incidence was found in severe PE, 93 cases (76.2%). In the 8 cases of AUP (6.5%), the total hysterectomy was necessary for maternal vital purpose. IUGR is common in these pathologies (22.9%), as is foetal death in utero (9%).
Monitoring the maternal-foetal evolution in case of pregnancies with associated hypertensive pathology, from a clinical, biochemical and ultrasound point of view and through interdisciplinary consultations, is extremely important for the obstetrical practice.
The early identification of worsening preeclampsia involves the prevention of maternal complications (eclampsia, HELLP syndrome, uteroplacental apoplexy) and foetal complications (IUGR, foetal intrauterine death).
Monitoring the maternal-foetal evolution and the early identification of the worsening of preeclampsia determine the improvement of the vital and functional maternal-foetal prognosis in PIH.
Conflict of interests: The authors declare no conflict of interests.
Bibliografie
-
Georgescu-Brăila M, Berceanu S. Obstetrica, vol II, partea a II-a, Ed Aius, Craiova, 1997:5–62.
-
Bouariu A, Popescu M, Iancu G. Current opinions on PlGF and sFlt-1 as reliable markers for preeclampsia. Ginecologia.ro. 2019;7(26):24-7.
-
Pritchard JA, Cunningham FG, Prichard SA. The Parkland Memorial Hospital protocol for treatment of eclampsia: evaluation of 245 cases. Am J Obstet Gynecol. 1984;148(7):951-63.
-
Hypertension in pregnancy. Report of the American College of Obstetricians and Gynecologist’s Task Force on Hypertension in Pregnancy. Obstet Gynecol. 2013 Nov;122(5):1122 -31.
-
Mitran M, Velicu O, Bohîlţea R. Diagnosis and prevention of preeclampsia – literature review. Ginecologia.ro. 2017;5(17):10-2.
-
Macdonald-Wallis C, Lawlor DA, Fraser A. Blood pressure change in normotensive gestational hypertensive, preeclamptic, and essential hypertensive pregnancies. Hypertension. 2012;59(6):1241-8.
-
Khan KS, Wojdyla D, Say L. WHO analysis of causes of maternal death: a systematic review. Lancet. 2006;367(9516):1066-74.
-
Berg CJ, Callaghan WM, Swerson C. Pregnancy-related mortality in the United States, 1998 to 2006. Obstet Gynecol. 2010;116(6):1302-9.
-
Saucedo M, Deneux-Tharaux C, Bouvier-Colle MH. Ten years of confidential inquires into maternal deaths in France, 1998-2007. Obstet Gynecol. 2013;122(4):752-60.
-
Brăila AD, Brăila M, Velea R. The severe form of preeclampsia. Particular situations, clinical and therapeutic implications. Filodiritto Ed. The 6th National Congress of SRUOG. 2018:62-6.
-
Arsene LV, Munteanu O, Voicu D. Assessment of the fetal-placental unit using clinical and ultrasound evaluation and inherited thrombophilia in pregnant patients. Ginecologia.ro. 2018;6(21):18-22.
-
Brăila AD, Neacşu A, Muşetescu AE. Biochemical markers in pregnancy associated with Sjogren syndrome and thrombophilia. Chim. 2018;69(8): 2300-3.
-
Ţurcan N, Bohîlţea R, Ioniţă D. Preeclampsia prevention strategies. Pharmacokinetics and pharmacodynamics of low-molecular-weight heparin (LMWH) in pregnancy. Ginecologia.ro. 2020;8(28):18-22.
-
Brăila AD, Marinov Krastev B, Mihai-Zamfir E. Uteroplacental apoplexy associated with invasive cervical neoplasm. RJME. 2017;58(4):1465-70.
-
Brăila AD, Gluhovschi A, Neacşu A. Placental abruption: etiopathogenic aspects, diagnostic and therapeutic implications. RJME. 2018;59(1):187-95.
-
Mihai-Zamfir E, Brăila AD, Brăila M. Convulsive syndrome in eclampsia and epilepsy in parturition under 30 years of age. RJMP. 2018;3(59):216-20.
-
Cunningam FG, Leveno KJ, Bloom SL, Spong Catherine Y, Dashe Jodi S, Hoffman Barbara L, Casey BM, Sheffield Jeanne S. Williams Obstetrics, 24rd Ed, 2017:637-52.
-
Crişan N, Nanu D, et al. Aspecte de conduită în formele severe de HTA indusă de sarcină. Obstetrica Ginecologia. 1994;3:103-6.
-
Brăila M, Neacşu A, Velea R, Brăila AD. Caesarean section and the forceps use - 5 year study in Craiova SCJU Maternity Section. Proceedings, The 13th Conference of the Romanian-German Society of Obstetrics and Gynecology. 2017:91-4.
Articole din ediţiile anterioare
OBSTETRICS | Ediţia 2 36 / 2022
Prognosticul neonatal al sarcinilor complicate cu anemie la adolescente
Diana Cristina Secară, Ana Veronica Uzunov, Octavian Munteanu, Alexandru Baroş, Monica Mihaela Cîrstoiu
Sarcina în rândul adolescentelor reprezintă o problemă de sănătate publică, având un impact deosebit asupra mamei, nou-născutului, societăţii...
31 mai 2022
GINECOLOGIE | Ediţia 12 (2) / 2016
Markeri moleculari utilizaţi pentru diagnostic, prognostic şi terapie în cancerul mamar - review
Cătălin Bogdan Coroleucă, Diana-Elena Comandașu, Ciprian Andrei Coroleucă, Prof. Dr. Elvira Brătilă, Ruxandra Stănculescu, Vasilica Baușic
Lucrarea îşi propune actualizarea informaţiilor privind implementarea în practica clinică a markerilor moleculari necesari stabilirii diagnosticulu...
15 aprilie 2016
GINECOLOGIE | Ediţia 3 21 / 2018
Corelaţii clinicopatologice în leiomiosarcoamele uterine – prezentare de cazuri şi review de literatură
Octavian Munteanu, Diana Ioana Voicu, Luciana Arsene, Ana Veronica Uzunov, Maria Sajin, Tiberiu Augustin Georgescu, Adrian Dumitru, Andreea Ruxandra Albu, Monica Mihaela Cîrstoiu
Sarcoamele uterine sunt un grup de tumori morfologic etergene extrem de agresive, cu o evoluţie clinică imprevizibilă şi cu prognostic slab. Con...
28 septembrie 2018
GINECOLOGIE | Ediţia 9 (3) / 2015
Importanţa testelor imunohistochimice în diagnosticul pozitiv al leziunilor epiteliale preneoplazice şi neoplazice endometriale
Maria Comănescu, Anca Potecă, Alexandru Comănescu, Teodor Potecă, Mihai Mitran
Neoplaziile maligne endometriale reprezintă una dintre cele mai frecvente leziuni ale tractului reproducător feminin, cazuri noi fiind descrise în ...
15 octombrie 2015