Endometrioza extrapelvică - experienţa personală
Extrapelvic endometriosis - our experience
Abstract
Endometriosis is the second most common gynaecologic entity, affecting up to 15% of women of reproductive age. It is defined by the presence of functional endometrial tissue (glands and stroma) outside the uterine cavity, which is responsive to hormonal stimulation. Although it predominantly locates on peritoneal surfaces, extrapelvic endometriosis has been reported in almost all parts of the body giving rise to a wide variety of clinical symptoms. Only a few cases of spontaneous endometriosis are described, the majority being strongly related to obstetrical or gynecological procedures. The etiology that completely explains the cause and pathogenesis of extrapelvic endometriosis is unknown. The diagnosis represents a real challenge for the clinicians, being neither easy nor routine. Neoplastic transformation was reported. The optimal treatment is still under debate for each location.Keywords
extrapelvic endometriosisendometriosisscar endometriosisRezumat
Endometrioza este a doua cea mai frecventă afecţiune ginecologică, afectând până la 15% dintre femeile de vârstă reproductivă. Este definită că prezenţa de ţesut endometrial funcţional (glande şi stromă) în afara cavităţii uterine, ţesut responsiv la stimul hormonal. Deşi se găseşte preponderent pe suprafeţe peritoneale, localizări ale endometriozei extrapelvice au fost raportate la nivelul aproape oricărei părţi a organismului, cauzând o mare varietate de simptome. Au fost descrise puţine cazuri de endometrioză extrapelvică spontană, majoritatea fiind consecutive unor intervenţii obstetricale sau ginecologice. Etiologia care să explice pe deplin cauzele şi patogeneza endometriozei rămâne încă necunoscută. Diagnosticul reprezintă o adevărată provocare pentru clinicieni, nefiind uşor sau de rutină. S-a raportat transformarea neoplazică a leziunilor endometriozice. Calea optimă de tratament este încă subiect de dezbateri pentru fiecare dintre localizări.Cuvinte Cheie
endometrioză extrapelvicăendometriozăendometrioza cicatricelorIntroduction
Endometriosis is represented by the presence of functional endometrial tissue outside the uterine cavity(1). It involves pelvic or extrapelvic sites, giving rise to a wide variety of clinical symptoms(2). Only few cases of spontaneous episodes are described, most of them being related to obstetrical or gynaecological procedures. The pathogenesis of extrapelvic endometriosis is unknown(2,3). The diagnosis represents a real challenge for the clinicians. Malignant transformation was reported(4). The best treatment is still under debate for each site. We present seven cases of extrapelvic endometriosis diagnosed and treated in the last 3 years in the Obstetrics and Gynaecology Department of “Nicolae Malaxa” Clinical Hospital, Bucharest: three cases of abdominal wall endometriosis developed on caesarean section scars, two cases of episiotomy scar endometriosis, one case of primary umbilical endometriosis and one case of anterior vaginal wall endometriosis involving the urethra.
Case reports
Case 1
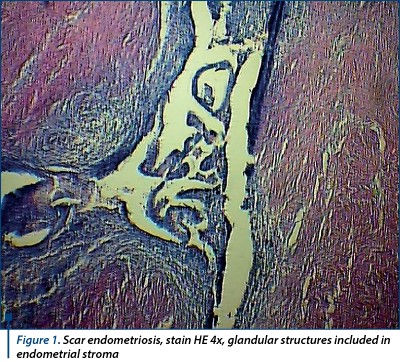
Three 28 to 39-year-old women experiencing cyclic monthly pain involving the abdominal caesarean scar and mild dysmenorrhoea 3 to 5 years after the procedure. Clinical exam was normal. Abdominal ultrasound and MRI of the the abdominal wall demonstrated in all cases subcutaneous cystic masses measuring 3.4 cm, 2.3 cm and 3.1 cm located in the abdominal wall fat, adjacent to the musculoaponeurotic layer. Surgery was performed with a wide local excision and reconstruction of the abdominal wall. Laparoscopic pelvic inspection revealed in two cases millimetric foci of peritoneal endometriosis in the Douglas pouch. Frozen section and pathologic paraffin wax examinations found endometrium glands and stroma (Figure 1). Hormonal therapy was provided for all patients after the surgery. At follow-up sessions, all patients were asymptomatic.
Case 2
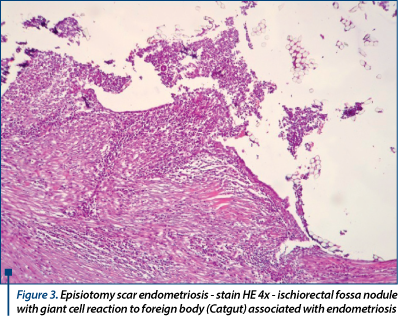
Two 42 year-old and 46 year-old ladies, at 10 and respectively 6 years after vaginal delivery, showed signs of perineum discomfort, pain and bluish swellings at the episiotomy scar. In both cases, CA-125 plasmatic levels were in normal ranges. The diagnosis was episiotomy scar endometriosis (Figure 2) and surgery was offered to both of them. The older patient chose the hormonal therapy, which failed to control the symptoms and, two years later, the intervention was performed. The surgical interventions were performed by a team of surgeons and gynaecologists, considering the possible involvement of the anal sphincter. Two and respectively 4 nodules, 1-4.5 cm in diameter, infiltrating the anal sphincter, the levatorani muscle, the ischiorectal fossa and the rectum wall were removed after wide dissection. Sphincteroplasty was required in one case. Pathologic examination found glands and endometrial stoma, hemosiderin deposits (Figure 3). The uterus and adnexa had normal appearance at postoperative abdominal ultrasound and MRI. Postoperative hormonal therapy with Depo-Provera in both cases, and followed by aromatase inhibitors and noretisterone acetatein in the older patient’s case (as enrollee in an international, multicenter clinical trial held within our department) strengthened the surgical treatment.
Case 3
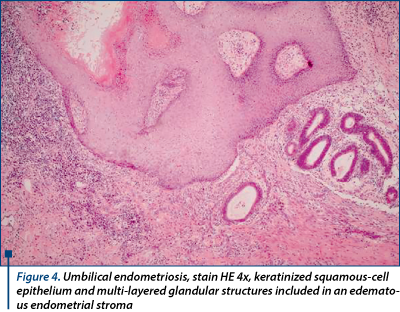
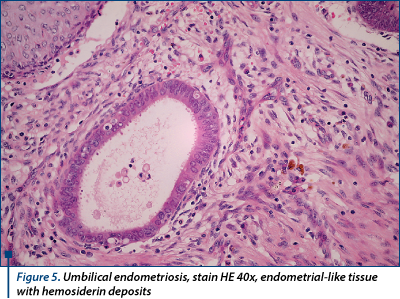
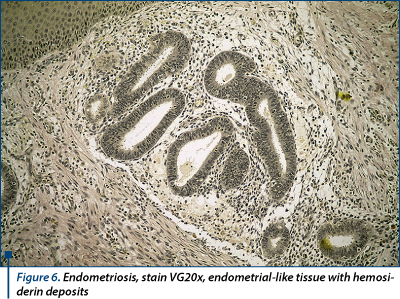
A 46-year-old lady, with an uncharacteristic personal history, presents excruciating abdominal pain and a large irreducible umbilical hernia (8/10 cm) with no signs of peritonitis or bowel obstruction. The initial diagnose was incarceration of the omentum in the umbilical hernial sac. On ultrasound, the hernial sac hosted a 4-cm hypoechoic mass. Surgery revealed an endometriotic nodule. Omphalectomy, partial omentum resection and a 3/4 cm endometriotic nodule excision with abdominal wall reconstruction were performed. Since no other macroscopic endometriotic peritoneal implants were found, the final diagnosis was simultaneous primary umbilical endometriosis and umbilical hernia, supported by pathologic examination (endometrium-like glands with and endometrium-like stroma with hemosiderin deposits - Figures 4, 5 and 6) and IHC positive tests for endometrial markers (‘Ck 7’, ‘AE1-AE3’, ‘CD10’). The postoperative evolution was uneventful. The patient is screened for endometriosis relapse every 3 months, the CA-125 plasmatic levels maintain within normal ranges and no signs of local recurrence are present.
Case 4
A 38-year-old woman, complaining of dysmenorrhea, dyspareunia and recurrent urinary tract infections, symptoms developed after her instrumental fourth vaginal delivery. Physical examination demonstrated a 2-cm mass on the lower segment of the anterior vaginal wall. Cystoscopy showed external urethral wall compression. Perineal ultrasound suggested a cystic mass in the vaginal wall. Surgery found a vaginal endometriotic cyst. Pathologic evaluation of the surgically excised lesion revealed endometriosis. The postoperative evolution was simple.
Discussions
Endometriosis is a benign disease, usually affecting the pelvic peritoneum. Despite its rarity, extrapelvic endometriosis has been described in almost all parts of the body(3), giving rise to a wide variety of clinical symptoms(2). Its presence is strongly related to prior gynaecologic or obstetric surgery(1). The diagnosis of this disorder represents a challenge for the clinicians, because catamenial features of endometriosis are characteristic, but not always present among symptoms of extrapelvic endometriosis(3). We thoroughly searched for this clinical signature of endometriosis in our anamnesis and found it only in three cases.

Our report concern some case of primary extrapelvic endometriosis involving the umbilicus and six others developed on surgical scars. We highlight in this report the long duration from the previous obstetric intervention to clinical manifestations, as well as normal CA-125 plasmatic levels at the time of diagnosis in all cases. The pathogenesis is easy to explain for scar endometriosis - direct inoculation during surgical intervention with subsequent response to oestrogen stimulation(5). For primary umbilical endometriosis, one of the rarest encounters, the pathogenesis is still being under debate(6). In our case, its presence was uncovered accidentally due to incarceration of the omentum in the umbilical hernial sac. Ultrasound scan or the more expensive CT and MRI scanning were used to exclude intra-abdominal extension in all cases. The differential diagnosis was made with other disorders such as primary or metastatic malignancies, inflammatory processes or other benign lesions (lipoma, inclusion cyst, haemangioma). Histopathological examination confirmed in all cases the clinical diagnosis. Rarely needed, immunohistochemical assay supported the results of the previous examination. Although malignant transformation was rarely reported(4), wide local surgical excision is mandatory to prevent this from happening, as well as to prevent local recurrence, to enable accurate pathological diagnosis and to obtain good cosmetic outcomes(2). The therapeutic approach varies from simple observation, to surgical or hormonal treatment or a combination of these methods(3). Hormonal therapy often fails to control the disease, though its utility increases when used as preoperative management or to strengthen the surgical treatment(3).
Conclusions
Endometriosis can be considered a “parasitic-like” tissue for its ability to implant itself and to maintain its functionality in almost all parts of the human body(1). Extrapelvic involvement is rare without prior pelvic surgery, with a wide range of clinical symptoms(2). Catamenial features of endometriosis are characteristic, but not always present among symptoms of extrapelvic endometriosis(3). The diagnosis is neither easy, nor routine. Histopathology confirms the diagnosis. Surgery is the only one capable to enable accurate pathological diagnosis, to prevent local recurrence or malignant transformation and to obtain good cosmetic outcomes(2,4).
Acknowledgement: This paper is supported by the Sectoral Operational Programme Human Resources Development (SOP HRD), financed from the European Social Fund and by the Romanian Government under the contract number POSDRU/187/1.5/S/156040
Bibliografie
Damodaran S, Mary N, NawrozI, Mahmood T. Abdominal wall endometriosis. Middle East Fertility Soc J, 2010; 15:292–3.
Arkoulis N, Chew BK. An unusual case of asymptomatic spontaneous umbilical endometriosis treated with skin-sparing excision. J Surg Case Rep, 2015:1–3.
Machairiotis N, Stylianaki A, Dryllis G, Zarogoulidis P, Kouroutou P, Tsiamis N, Katsikogiannis N, Sarika E, Courcoutsakis N, Tsiouda T, Gschwendtner A, Zarogoulidis K, Sakkas L, Baliaka A, Machairiotis C. Extrapelvic endometriosis: a rare entity or anunder diagnosed condition? Diagnc Pathol, 2013; 8:194.
Fargas Fàbregas F, Cusidó Guimferrer M, Tresserra Casas F, Baulies Caballero S, Fábregas Xauradó R. Malignant transformation of abdominal wall endometriosis with lymph node metastasis. Case report and review of literature. Gynecolc Oncol Rep, 2014; 8:10–3.
Uzunçakmak C, Gülda A, Özçam H, Dinç K. Scar Endometriosis: A Case Report of This Uncommon Entityand Review of the Literature. Case Reports in Obstetrics and Gynecology, 2013, Article ID 386783, http://dx.doi.org/10.1155/2013/386783.
Stojanovic M, Radojkovic M, Jeremic L, Zlatic A, Stanojevic G, Janjic D, Mihajlovic S, Dimov I, Kostov M, Zdravkovic M, Stojanovic M. Umbilical Endometriosis Associated with Large Umbilical Hernia. Case Report. Chirurgia, 2014; 109:267-70.

Sarcina la adolescente - o problemă la nivel global
Daniela Stan, Mihai Mitran
S-a spus că numărul adolescentelor însărcinate atinge proporţii epidemice. Însă nu ne putem da cu adevărat seama de amploarea acestui fenomen dacă nu luăm în considerare impactul pe care îl are sarcina asupra adolescentei. În cel mai bun caz, viaţa ei va fi supusă unor schimbări majore, care îi vor marca pe e...
Refluxul vezico-ureteral congenital
Simona Vlădăreanu, Monica-Mihaela Cîrstoiu, Costin Berceanu, Claudia Mehedințu, Virgil-Ionuţ Mihoci
Refluxul vezico-ureteral (RVU), existenţa unui flux de urină retrograd orientat dinspre vezica urinară spre tractul urinar superior, este diagnosticat frecvent în contextul unei infecţii de tract urinar (ITU). Menţinerea...
Metodologia de achiziţie a plânsului nou-născutului
Elvira Brătilă, Diana-Elena Comandașu, Ştefan-Stelian Diaconescu, Mircea Sorin Rusu, Gheorghiţa Sardescu
Plânsul reprezintă iniţierea comunicării vocale umane, fiind cel mai important mijloc de transmitere a nevoilor şi dorinţelor sugarilor. Acest articol furnizează informaţiile necesare pentru proiectar...
Anatomia continenţei urinare la femei
Elvira Brătilă, Simona Vlădăreanu, Costin Berceanu, Monica-Mihaela Cîrstoiu, Claudia Mehedințu, Diana-Elena Comandașu
Mecanismele continenţiei urinare sunt încă controversate şi neînţelese pe deplin. În acest articol prezentăm principalul concept care descrie fiziopatologia continenţei urinare. Conform datelor recente din literatura de ...
Investigaţiile urodinamice şi valoarea acestora în luarea deciziilor terapeutice la femeile cu simptome urinare
Andrei Manu-Marin
Introducere. Investigaţiile urodinamice obiectivează presiune din detrusor în timpul umplerii controlate a vezicii urinare, cât şi în timpul micţiunii şi raportează această presiune la debitul urinar ...