Early detection of micrognathia during prenatal care is crucial to mitigate the associated risks and prevent unforeseen emergencies requiring invasive procedures, like tracheostomy. It enables proper planning for delivery in specialized tertiary care centers staffed with experienced teams in managing such cases. This proactive approach enhances clinician readiness, facilitates decision-making regarding management strategies in advance, and fosters improved family education and support. The primary goals of this paper are to provide a comprehensive review of diverse diagnostic techniques for micrognathia and to suggest a clear and pragmatic prenatal approach to addressing this condition. Furthermore, we present relevant ultrasonographic pictures of fetal micrognathia from our personal database.
Prenatal diagnosis of micrognathia
Micrognaţia – diagnostic prenatal
First published: 28 martie 2024
Editorial Group: MEDICHUB MEDIA
DOI: 10.26416/Gine.43.1.2024.9417
Abstract
Rezumat
Detecţia prenatală precoce a micrognaţiei este esenţială pentru a aprecia în mod obiectiv riscurile neonatale asociate şi necesitatea intervenţiei invazive de urgenţă, precum traheostomia. De asemenea, permite planificarea naşterii într-un centru terţiar specializat în gestionarea unor asemenea cazuri. Această abordare proactivă facilitează consilierea corectă a cuplului şi elaborarea unui plan decizional prompt. Obiectivele acestei lucrări sunt sintetizarea elementelor diagnostice pentru micrognaţie şi conturarea planului de urmărire prenatală în cazul feţilor cu această patologie. În plus, vom prezenta imagini ultrasonografice din cazuistica proprie, relevante pentru micrognaţia fetală.
Introduction
Micrognathia is a facial abnormality characterized by a reduced size of the mandible, leading to the fetus presenting with a small jaw and an overbite when viewed in profile. Being one of the most prevalent craniofacial deformities, micrognathia often coexists with retrognathia, glossoptosis and upper airway obstruction. These conditions can significantly impact the appearance of infants, complicate feeding, and pose substantial risks to infant survival(1,2).
While the exact cause of micrognathia remains unclear, it is well known that the mandible develops from the first pharyngeal arch. Therefore, any disruption to the development of the pharyngeal arch complex can lead to abnormalities in the mandible, maxilla and ear. One hypothesis suggests that ischemic necrosis, triggered by an enlarging hematoma originating from the stapedial artery system, which initially supplies blood to the first pharyngeal arch, may lead to the underdevelopment of the first arch, ultimately resulting in craniofacial microsomia(3).
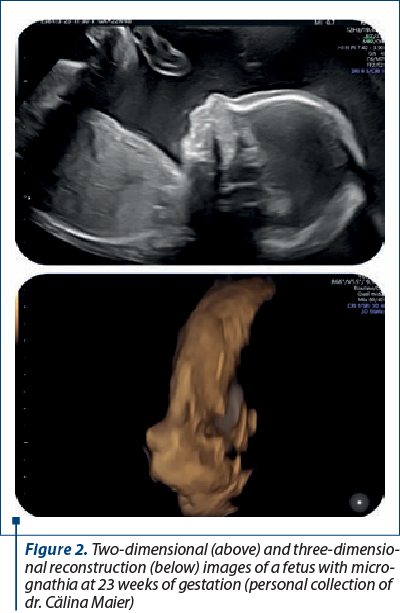
Advancements in fetal imaging have made it possible to detect fetal micrognathia relatively early in gestation, sometimes even as early as the first trimester (Figure 1). However, these cases are typically reevaluated later in the second trimester, particularly if there are no significant chromosomal or structural abnormalities present(2) (Figure 2).
Ultrasound findings
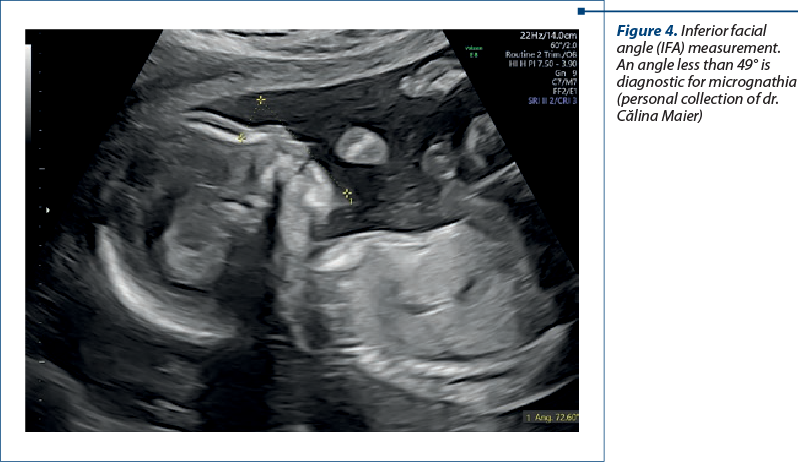
To enhance sensitivity and accuracy, several objective biometric indices have been introduced to refine the definition of micrognathia during prenatal assessment, including: the jaw index, the inferior facial angle (IFA), and the fronto-naso-mental angle (FNMA). The first one is determined by measuring the anteroposterior diameter of the fetal mandible at the axial plane and expressing it as a percentage of the biparietal diameter. This calculation yields an index that remains unaffected by gestational age. The IFA, measured in the midsagittal view of the fetal profile, is formed by the intersection of a line perpendicular to the vertical part of the forehead drawn at the level of nasal bone synostosis, and a line passing through the tip of the chin and the more protruding lip, typically the upper lip. Thus, an angle less than 49o gives the diagnosis of micrognathia (Figure 4).
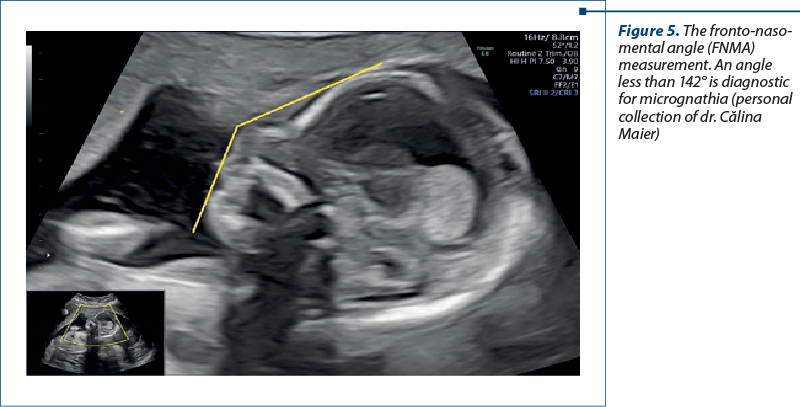
The FNMA is formed by the intersection of a line drawn from the tip of the nose to the frontal bone and another line extending from the nasal tip to the mentum(4-7) (Figure 5).
Caution should be exercised when diagnosing a fetus with “micrognathia”, particularly based on subjective evaluation. This term suggests an abnormality with significant pathology, yet micrognathia may become less noticeable with ongoing growth and development. There is no universally accepted gold standard for definitively diagnosing micrognathia postnatally. Employing a combination of objective sonographic markers along with follow-up ultrasound assessments can significantly diminish the risk of a false diagnosis.

Associated anomalies
Micrognathia is commonly linked to chromosomal abnormalities (trisomy 18/13/9/8, Turner syndrome, 22q11.2 deletion syndrome, deletions of chromosome 4/5, Pallister-Killian syndrome)(8), and other dysmorphic syndromes.
Primary mandibular syndromes encompass Pierre Robin sequence, characterized by micrognathia leading to glossoptosis and often accompanied by cleft palate, typically diagnosable in the third trimester. Other syndromes include Nager syndrome, Treacher-Collins syndrome and orofacial digital syndromes, which involve central nervous system and hand anomalies. Skeletal and neuromuscular disorders associated with micrognathia encompass a range of conditions, including various skeletal dysplasias such as achondrogenesis, campomelic dysplasia, diastrophic dysplasia, and others. Additionally, craniosynostosis syndromes, like Shprintzen-Goldberg syndrome, as well as Roberts pseudothalidomide syndrome are also known to include micrognathia(9,10).
Micrognathia can indeed have a functional cause. In conditions such as fetal akinesia deformation sequence, the fixed contracture of the temporomandibular joint hinders the typical development of the mandible. Furthermore, even in cases where micrognathia appears isolated, additional abnormalities may manifest later in gestation or postnatally(11).
Genetic testing
Diagnostic testing with chromosomal microarray analysis (CMA) should be considered when significant micrognathia is detected, especially if there are other features suggestive of a syndromic diagnosis. If a common aneuploidy syndrome is suspected, karyotype analysis or fluorescence in situ hybridization (FISH) with reflex CMA is a reasonable approach. While micrognathia can be inherited, a de novo variant is often associated with severe micrognathia.
In cases with additional anomalies, consanguinity or a family history of a specific condition, gene panel testing or exome sequencing may be beneficial, as CMA does not identify single-gene (Mendelian) disorders. If exome sequencing is pursued, appropriate pretest and posttest genetic counseling by a provider experienced in genomic sequencing complexities is recommended(12).
Following thorough counseling, cell-free DNA screening is a reasonable consideration for patients who decline diagnostic evaluation, especially when a common aneuploidy syndrome is suspected. In cases where micrognathia is isolated, it is recommended to assess both parents, as mild micrognathia can sometimes be a constitutionally inherited variant(12).
Pregnancy and delivery management
In addition to a comprehensive ultrasound examination, a thorough evaluation of fetal cardiac anatomy is crucial, and consideration should be given to performing a fetal echocardiogram. Fetal magnetic resonance imaging (MRI) may prove beneficial if the palate is not clearly visualized or if there are concerns regarding cerebral anomalies. It’s important to emphasize that careful assessment of fetal cardiac anatomy should always be prioritized. Consultation with an ear, nose and throat specialist may be beneficial if there is suspicion of airway obstruction. It is important to counsel the patient about potential neonatal challenges related to breathing and feeding(13).
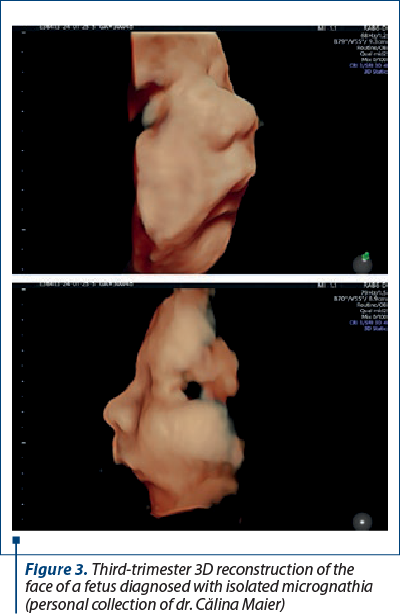
Pregnancy termination should be a topic of discussion with all patients upon detection of a fetal anomaly, although in cases of isolated, mild micrognathia, the prognosis can be favorable. It is advisable to conduct a third-trimester growth ultrasound examination, focusing on reevaluating the mandible, fetal growth, and amniotic fluid index (Figure 3). There is typically no need to alter the route of delivery; however, delivering in a tertiary care center is recommended, with pediatric and potentially ear, nose and throat specialists available to provide immediate intervention if necessary. Additionally, a lactation consultation should be arranged, and a breast pump can be prescribed if desired(13).
Prognosis
The prognosis varies depending on the ultimate syndromic diagnosis. Isolated micrognathia is frequently linked with Pierre Robin sequence, which includes glossoptosis, and there should be anticipation of airway obstruction at delivery. In certain instances, mandibular growth can accelerate and normalize into adulthood. Prognostic counseling should be tailored based on the suspected diagnosis derived from sonographic findings and diagnostic testing(14).
Conclusions
The assessment of the fetal face during the second trimester may be hindered by fetal position, but remains a crucial part of routine evaluation. Until recently, prenatal diagnosis of fetal micrognathia relied on subjective methods, primarily involving the evaluation of the fetal profile and the relationship between the maxilla and mandible. The detection of micrognathia should prompt further investigations, including karyotyping, sonographic assessment for additional abnormalities such as skeletal and cardiac anomalies, as well as evaluation of fetal ears. Obtaining a detailed maternal history, including familial syndromes and exposure to drugs, is also essential in the diagnostic process.
Corresponding author:
Călina Maier
E-mail: calinamaier@yahoo.com
Conflict of interest: none declared.
financial support: none declared.
This work is permanently accessible online free of charge and published under the CC-BY licence.

Bibliografie
- Paladini D. Fetal micrognathia: almost always an ominous finding. Ultrasound Obstet Gynecol. 2010;35(4):377-84.
- Zhen L, Yang YD, Xu LL, Cao Q, Li DZ. Fetal micrognathia in the first trimester: an ominous finding even after a normal array. Eur J Obstet Gynecol Reprod Biol. 2021;263:176–80.
- Sankaran S, Kyle P. In: Twining’s Textbook of Fetal Abnormalities (Third Edition), 2014. Chapter 13. Abnormalities of the face and neck. Pages 289-335.
- Antonakopoulos N, Bhide A. Focus on prenatal detection of micrognathia. J Fet Med. 2019;06(03):107-12.
- Chitty LS, Campbell S, Altman DG. Measurement of the fetal mandible – feasibility and construction of a centile chart. Prenat Diagn. 1993:13(8):749–56.
- Paladini D, Morra T, Teodoro A, Lamberti A, Tremolaterra F, Martinelli P. Objective diagnosis of micrognathia in the fetus: the jaw index. Obstet Gynecol.1999;93(3):382–6.
- Li H, Zhu Z. Ultrasonographic study of fetal mandibular markers during the first trimester in a Chinese population. J Obstet Gynaecol Res. 2022;48(2):333–9.
- Luedders D, Bohlmann M, Germer U, Axt-Fliedner R, Gembruch U, Weichert J. Fetal micrognathia: objective assessment and associated anomalies on prenatal sonogram. Prenat Diagn. 2011;31(2):146–51.
- Nicolaides KH, Salvesen DR, Snijders RJ, Gosden CM. Fetal facial defects: associated malformations and chromosomal abnormalities. Fetal Diagn Ther. 1993;8(1):1–9.
- Bromley B, Benacerraf BR. Fetal micrognathia: associated anomalies and outcome. J Ultrasound Med. 1994;13(7):529–33.
- https://fetalmedicine.org/education/fetal-abnormalities/face/micrognathia
- International Society for Prenatal Diagnosis, Society for Maternal Fetal Medicine, Perinatal Quality Foundation. Joint Position Statement from the International Society for Prenatal Diagnosis (ISPD), the Society for Maternal Fetal Medicine (SMFM), and the Perinatal Quality Foundation (PQF) on the use of genome-wide sequencing for fetal diagnosis. Prenat Diagn. 2018;38(1):6-9.
- Suenaga M, Hidaka N, Kido S, Otera Y, Fukushima K, Kato K. Successful ex utero intrapartum treatment procedure for prenatally diagnosed severe micrognathia: a case report. J Obstet Gynaecol Res. 2014;40(8):2005–9.
- Kaufman MG, Cassady CI, Hyman CH, et al. Prenatal identification of Pierre Robin sequence: a review of the literature and look towards the future. Fetal Diagn Ther. 2016;39(2):81–9.
Articole din ediţiile anterioare
A rare case of omphalocele and trisomy 18
Omphalocele, also called exomphalos, is a congenital malformation due to a defect in the closure of the anterior abdominal wall. The characteristic...
Horseshoe kidney – fetal ultrasound diagnosis
The spectrum of congenital anomalies of the kidney and urinary tract (CAKUT) is broad, ranging from mild cases involving unilateral hydronephrosis ...
Umbilical cord hematoma associated with placenta accreta spectrum
Prenatal ultrasonographic examination has proven its utility in evaluating and diagnosing placental as well as umbilical cord anomalies. Although r...
The prenatal diagnosis of chromosomal anomalies by quantitative fluorescence polymerase chain reaction in Romania – a five-year report from a new institute
The prenatal diagnosis of chromosomal anomalies is of high importance in cases of pregnancies with increased risk, such as the mother’s age over 35...