Umbilical cord cysts are rare anomalies, being associated in the first trimester most often with chromosomal defects or structural anomalies, while in the second and third trimesters, they are associated with urachal abnormalities. Umbilical cord cysts remain a pathology that could endanger the fetus by a rapid growth that could cause umbilical cord compression followed by fetal distress, torsion or thrombosis, with unfavorable consequences. We present the case of a pregnant patient diagnosed in the second trimester with umbilical cord cyst localized at the placental site of the umbilical cord, with a low-risk noninvasive prenatal test performed in the first trimester, with no other structural anomalies, who delivered a healthy baby at term. The intraoperative findings included the presence of an abnormally adherent placenta, respectively placenta accreta, in a patient with no surgical or obstetrical risk factors. The pathology report revealed an umbilical cord hematoma. The aim of this article is to debate whether an umbilical cord hematoma could be a marker for placental abnormalities.
Umbilical cord hematoma associated with placenta accreta spectrum
Hematom de cordon ombilical asociat cu placentă din spectrul accreta
First published: 27 noiembrie 2023
Editorial Group: MEDICHUB MEDIA
DOI: 10.26416/Gine.42.4.2023.8990
Abstract
Rezumat
Chisturile de cordon ombilical reprezintă anomalii rare, fiind asociate în primul trimestru cu anomalii cromozomiale sau defecte structurale, în timp ce în al doilea şi al treilea trimestru sunt asociate cu anomalii uracale. Chisturile de cordon ombilical rămân o patologie care ar putea pune în pericol fătul, printr-o creştere rapidă ce ar putea determina compresia cordonului ombilical ulterior, urmată de suferinţă fetală, torsiune sau tromboză, cu consecinţe nefavorabile. Prezentăm cazul unei paciente gravide diagnosticate în al doilea trimestru cu chist de cordon ombilical localizat la nivelul inserţiei placentare a cordonului ombilical, cu un test prenatal neinvaziv cu risc scăzut efectuat în primul trimestru, fără alte anomalii structurale, care a născut la termen un copil sănătos. Constatările intraoperatorii au inclus prezenţa unei placente aderente, respectiv a placentei accreta, la o pacientă fără factori de risc chirurgicali sau obstetricali. Raportul de anatomie patologică relevă un hematom de cordon ombilical. Scopul acestui articol este de a dezbate dacă un hematom de cordon ombilical ar putea fi un marker pentru anomalii placentare.
Introduction
Prenatal ultrasonographic examination has proven its utility in evaluating and diagnosing placental as well as umbilical cord anomalies. Although rare, the main umbilical cord anomalies are represented by vascular abnormalities (umbilical artery hypoplasia, single umbilical artery, varix and aneurysms, supernumerary vessels)(1,2), cysts(3), cord insertion anomalies that interest the placental site (marginal, velamentous insertion) or the fetal site (omphalocele, gastroschisis, cloacal malformation, bladder exstrophy or amniotic bands)(4), thin cord, umbilical cord knot, abnormal coil or twist of the umbilical cord(5), or even solid anomalies (angiomyxoma, hematoma, teratoma)(6). Umbilical cord cysts have an incidence of 2-3%, and the most incriminated risk factor are chromosomal anomalies(7). Umbilical cord cysts (UCC) have been described as isolated ultrasonographic findings or associated with fetal aneuploidies, vertebral defects, omphalocele, imperforated anus, radial and renal dysplasia association, tracheoesophageal fistula or cord angiomyxoma. UCC could endanger the fetus as they could present an accelerated growth, altering the blood flow to the fetus and cause fetal distress; the most obscure outcome could be a torsion or thrombosis of the cyst that may lead to intrauterine death(7,8). To our current knowledge, there are no data in the literature associating umbilical cord hematomas with the presence of placenta accreta spectrum. We present the case of a pregnant patient with an umbilical cord hematoma firstly described at 25 gestational weeks and 3 days as an umbilical cord cyst that proved to be an umbilical cord hematoma, who underwent an elective caesarean section at term, with intraoperative findings of placenta accreta.
Case report
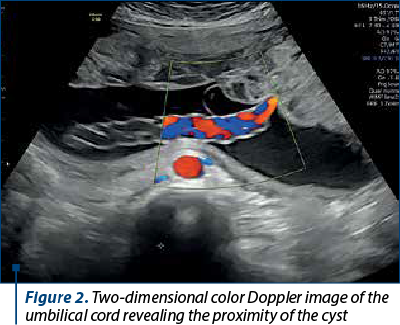
We present the case of a 36-year-old primigravida, with no obstetrical history and a naturally obtained pregnancy, who presented in our medical practice for pregnancy monitoring. The patient recorded no data regarding surgical history or invasive uterine procedures. The patient underwent a noninvasive prenatal test for the major chromosomal abnormalities, whose result was low risk for trisomies 13, 18 and 21. The pregnancy had a normal course until 25 gestational weeks and 3 days when a 3-cm anechogenic cystic image near the placental site of the umbilical cord, supposed to be an umbilical cord cyst, was identified during an ultrasonographic evaluation (Figures 1 and 2).

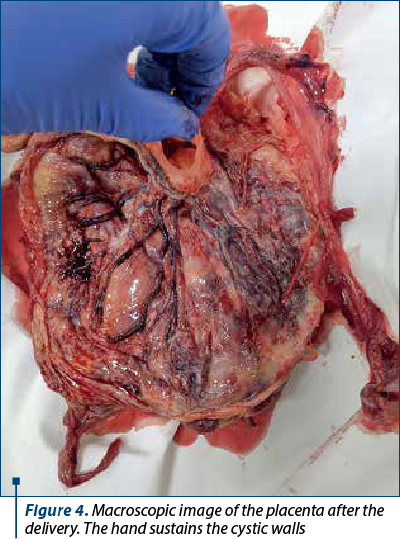
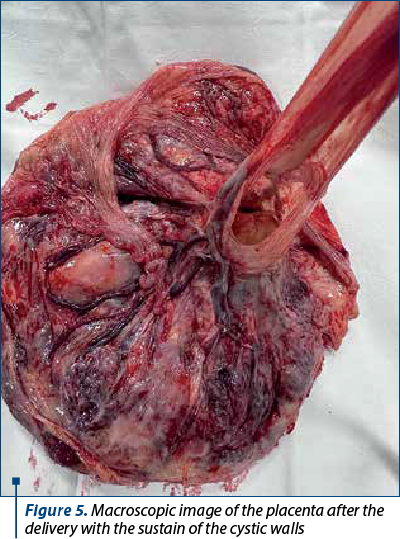
No other structural anomalies were described; the fetal weight, the Doppler velocimetry evaluation of the fetus, the amniotic fluid index, the biophysical profile, all ultrasonographic markers were within normal ranges. The cyst’s dimensions slightly grew until term (4.2 cm at 37 gestational weeks and 4 days) – Figure 3. Due to the possibility of fetal distress, the patient underwent an elective caesarean section at 39 gestational weeks and 3 days. A healthy baby boy, weighing 3000 g, with an Apgar score of 9 at 1 minute and 9 at 5 minutes, was delivered. The surgical findings were represented by the umbilical cord cyst, which was ruptured during the extraction of the placenta, as well as an abnormally invasive placenta, respectively placenta accreta (Figures 4, 5 and 6).
Reviewing more carefully the ultrasonographic images captured during pregnancy, we noticed the interruption of the clear retroplacental space (Figure 3).


The pathology report described a 3.5-cm umbilical cord hematoma and a white hardened area near the placental site of the umbilical cord.
Discussion
Firstly, to our current knowledge, in the literature there is no association between umbilical cord hematoma and placenta accreta spectrum.
Umbilical cord cysts described in the second and third trimesters of pregnancy are associated with other structural anomalies (urachal abnormalities), and they usually have their origin in embryonic remnants; they are represented by omphalomesenteric cysts and allantoic cysts, being located near the fetal site of the umbilical cord(9,10). The differential diagnosis in our case was based on the location of the cyst. Furthermore, spontaneous umbilical cord hematomas represent a rare pathology, being more frequently observed after invasive procedures, which was not performed in our case.
The main risk factors for placenta accreta spectrum are represented by anterior caesarean delivery, uterine procedures (dilatation and curettage, hysteroscopic procedures, endometrial ablation, myomectomy interesting the uterine cavity), infertility procedures (e.g., embryo transfer), multiparity, postpartum endometritis, manual extraction of the placenta, maternal age above 35 years old, and personal history of pelvic irradiation(11). In an article regarding twin pregnancy published by Lee et al. in 2021(12), twin pregnancies with velamentous cord insertion are more frequently associated with vasa praevia and placenta accreta spectrum, compared to pregnancies without velamentous cord insertion. Regarding the invasive placentation, given the fact that this was the first pregnancy and the patient did not undergo uterine interventions, and no artificial reproductive techniques were present as risk factors, maternal age was the single risk factor identified in our case. Regarding risk factors for the two pathologies, in our case there have not been any common risk factors.
The question we raise now is the following: “Is it possible that umbilical cord hematoma could be a marker for placental abnormalities?” We believe the answer is not yet known, so the take-home message should be the fact that pregnant patients with umbilical cord hematomas require a thorough monitoring and an accurate evaluation of the retroplacental clear space, even in patients with no obstetrical history or no uterine procedures performed, in order to improve the obstetrical outcome.
Conclusions
This was an atypical case of placenta accreta in a primipara with no risk factors for placenta accreta spectrum diagnosed during surgery, a pregnancy with no particularities besides an umbilical cord cyst diagnosed at 25 gestational weeks and 3 days, ulteriorly pathologically diagnosed as an umbilical cord hematoma. The umbilical cord hematoma did not cause umbilical cord compression and was not associated with chromosomal abnormalities. In conclusion, each and every pregnancy complicated with umbilical cord hematoma should be offered a thorough evaluation of the retroplacental clear space, as it could be a possible marker for placenta accreta spectrum; this prenatal finding could improve the obstetrical outcomes.
Conflict of interest: none declared.
financial support: none declared.
This work is permanently accessible online free of charge and published under the CC-BY licence.

Bibliografie
-
Pérez-Cosio C, Sheiner E, Abramowicz JS. Four-vessel umbilical cord: not always a dire prognosis. J Ultrasound Med. 2008;27(9):1389-91.
-
Aoki S, Hata T, Ariyuki Y, Makihara K, Hata K, Kitao M. Antenatal diagnosis of aberrant umbilical vessels. Gynecol Obstet Invest. 1997;43(4):232-5.
-
Ghezzi F, Raio L, Di Naro E, Franchi M, Cromi A, Dürig P. Single and multiple umbilical cord cysts in early gestation: two different entities. Ultrasound Obstet Gynecol. 2003;21(3):215-9.
-
Sepulveda W, Rojas I, Robert JA, Schnapp C, Alcalde JL. Prenatal detection of velamentous insertion of the umbilical cord: a prospective color Doppler ultrasound study. Ultrasound Obstet Gynecol. 2003;21(6):564-9.
-
De Laat MW, Franx A, Nikkels PG, Visser GH. Prenatal ultrasonographic prediction of the umbilical coiling index at birth and adverse pregnancy outcome. Ultrasound Obstet Gynecol. 2006t;28(5):704-9.
-
Daniel-Spiegel E, Weiner E, Gimburg G, Shalev E. The association of umbilical cord hemangioma with fetal vascular birthmarks. Prenat Diagn. 2005;25(4):300-3.
-
McCalla CO, Lajinian S, DeSouza D, Rottem S. Natural history of antenatal omphalomesenteric duct cyst. J Ultrasound Med. 1995;14(8):639-40.
-
Bohîlţea RE, Dima V, Ducu I, Iordache AM, Mihai BM, Munteanu O, Grigoriu C, Veduţă A, Pelinescu-Onciul D, Vlădăreanu R. Clinically Relevant Prenatal Ultrasound Diagnosis of Umbilical Cord Pathology. Diagnostics (Basel). 2022;12(2):236.
-
Wildhaber BE, Antonelli E, Pfister RE. The giant umbilical cord. Arch Dis Child Fetal Neonatal Ed. 2005;90(6):F535-6.
-
Heifetz SA, Rueda-Pedraza ME. Omphalomesenteric duct cysts of the umbilical cord. Pediatr Pathol. 1983;1(3):325-35.
-
Heller DS, Wyand R, Cramer S. Recurrence of basal plate myofibers, with further consideration of pathogenesis. Fetal Pediatr Pathol. 2019;38(1):30-43.
-
Lee HM, Lee S, Park MK, Han YJ, Kim MY, Boo HY, Chung JH. Clinical significance of velamentous cord insertion prenatally diagnosed in twin pregnancy. J Clin Med. 20213;10(4):572.
Articole din ediţiile anterioare
Body stalk anomaly – case report and review
Body stalk anomaly is a rare congenital defect with an incidence rate ranging from 1 in 14,000 to 1 in 31,000 pregnancies, according to large epide...
Ultrasound-based differential diagnosis of fetal abdominal wall defects in early pregnancy
Fetal abdominal wall defects (AWDs) encompass a wide range of congenital anomalies that involve the incomplete closure or disruption of the abdomin...
Prenatal diagnosis of micrognathia
Early detection of micrognathia during prenatal care is crucial to mitigate the associated risks and prevent unforeseen emergencies requiring inv...
Performance of imaging exams in screening and diagnosis of breast cancer
Breast cancer holds great importance as a public health issue, threatening the physical and mental well-being of women worldwide. According to the ...