Ultrasound assessment of the fetal face represents the first way of interaction of the parents with their unborn baby, therefore this kind of evaluation is gaining followers worldwide, as it is useful in developing a strong maternal-fetal bonding. It is acknowledged that an important number of genetic disorders are associated with various degrees of facial anomalies. The ultrasound appearance of the fetal face is influenced by gestational age, as it varies significantly during gestation. In most of the countries, the anomaly scan is performed between 18 and 22 weeks of gestation. Fetal face structures can be assessed by using various reference scanning planes such as axial, coronal, sagittal and oblique views. Due to its importance, most ultrasound societies, including the Romanian Society of Ultrasound in Obstetrics and Gynecology (SRUOG), have published guidelines in order to standardize the fetal face assessment during the first- and second-trimester screening scan. We present a series of particular cases of fetal facial anomalies diagnosed at first- and second-trimester anomaly scans that certify the need of complying with the protocols for fetal face assessment and also the usefulness of additional techniques for the detection of more subtle findings.
Provocări în evaluarea feţei fetale – diagnostic şi management
Challenges in evaluating the fetal face – diagnosis and management
First published: 23 octombrie 2020
Editorial Group: MEDICHUB MEDIA
DOI: 10.26416/ObsGin.68.3.2020.4017
Abstract
Rezumat
Evaluarea ecografică a feţei fetale reprezintă prima metodă de interacţiune a părinţilor cu bebeluşul lor în perioada antenatală. De aceea, acest tip de evaluare câştigă tot mai mulţi adepţi, datorită faptului că reuşeşte să creeze o legătură puternică între mamă şi făt. Este bine cunoscut faptul că un număr important de anomalii genetice se asociază cu grade variate de malformaţii faciale fetale. Aspectul ecografic al feţei fetale variază pe parcursul gestaţiei. În majoritatea ţărilor, evaluarea ecografică a anatomiei fetale se realizează între 18 şi 22 de săptămâni de gestaţie. Anatomia feţei fetale poate fi evaluată ecografic folosind o serie de planuri secţionale, precum planurile axiale, coronale, sagitale şi oblice. Datorită importanţei sale, majoritatea societăţilor de ecografie, inclusiv Societatea Română de Ultrasonografie în Obstetrică şi Ginecologie (SRUOG), au publicat o serie de ghiduri de evaluare ecografică. Am întâlnit mai multe cazuri deosebite de malformaţii faciale fetale, la diverse vârste gestaţionale, care demonstrează atât nevoia respectării protocoalelor existente de examinare a feţei fetale, cât şi utilitatea tehnicilor adiţionale în stabilirea unor diagnostice mai subtile.
Introduction
The ultrasound assessment of the fetal face is the first way of interaction of the parents with their unborn baby, therefore recent achievements in three-dimensional (3D) ultrasound are playing a central role in the development of maternal-fetal connection. Besides the bonding experience, it is already acknowledged that an important number of chromosomal and non-chromosomal syndromes are associated with various degrees of facial anomalies. In addition, fetal face disorders, such as microphthalmia, retro- and micrognathia or cleft lip/palate, have a high social and cosmetic impact. For this reason, this anatomic region benefits the most from a 3D ultrasound approach(1).
The ultrasound appearance of the fetal face is influenced by the gestational age, as it varies appreciably during gestation. Accordingly, if until 23-24 weeks the fetal face has a thin and bony appearance, in the third trimester the facial features start to smooth and acquire progressively individual traits. As it is an extremely irregular region, the ultrasound evaluation of the fetal face requires a standardized approach, being one of the most delicate and difficult areas to explore(2).
In most of the countries, the anomaly scan is performed between 18 and 22 weeks of gestation. Therefore, fetal face is assessed during the second-trimester screening for fetal malformations, although in an inceptive way it is evaluated since the first trimester, as some of face anomalies benefit from an early diagnosis. Also, modern ultrasound equipment allows for a detailed and accurate evaluation of the first-trimester fetal face in most of the cases.
Fetal face structures can be assessed by using various reference scanning planes, such as axial, coronal sagittal and oblique views(1). Scanning in axial planes in lateral or preferably ventral approach, several important features can be evaluated: symmetrical orbits with the presence of ocular lenses, palate alveolar ridge, tongue/pharynx, and mandible/inferior alveolar ridge. Sagittal views are also important and provide information regarding the facial profile when scanning in median or mid-sagittal plane, and ears when using parasagittal views. Additional coronal and oblique views are also used to complete the evaluation of the fetal face: the coronal view of the face and palate and the oblique view of the upper lip.
Due to its importance, guidelines have been published in order to standardize the fetal face assessment and are recommended by most of the ultrasound societies. The Romanian Society of Ultrasound in Obstetrics and Gynecology (SRUOG) guidelines recommend the assessment of the following structures as minimal requirements for the basic fetal anatomical survey: both orbits with the presence of ocular lenses, the assessment of the fetal profile with the presence of the nasal bone, the nostrils and the lips (especially the upper lip). Still, sometimes beyond the standard examination, extended views and tools are required in order to sustain a correct diagnosis regarding the fetal face: position of the tongue, three-dimensional assessment.
We present a series of cases with facial abnormalities diagnosed in our department at various gestational ages. Each case is accompanied by a short presentation of the diagnosis features, management options and counseling. The aim of the paper is to emphasize the importance of detailed face evaluation in the context of modern multidisciplinary fetal medicine.
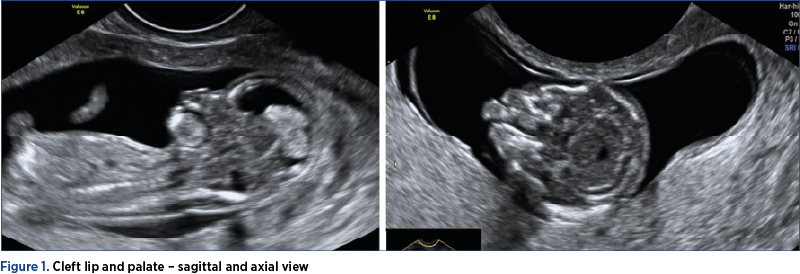
Case 1: Cleft lip and palate
A primiparous woman, 18 years old, was referred to our unit for the 11-13+6-week scan. The patient had no obstetrical history. The fetal face assessment revealed on axial and coronal views bilateral cleft lip and palate.
The risk for chromosomal and nonchromosomal anomalies is higher for cleft lip and palate rather than cleft palate, with a higher incidence in case of bilateral localizations. Still, the worse prognosis interests the median cleft, as in most of the cases it is associated with holoprosencephaly and other severe median defects. The risk in case of isolated cleft lip is minimal. The prognosis depends on the nature, whether the defect is isolated or is part of a chromosomal or nonchromosomal defect(1,3).
Usually, the diagnosis of a major defect at an early age is sufficient for the parents to decide the termination of pregnancy (TOP). In this case, the further exploration following TOP revealed other associated anomalies, but the trigger represented the face anomaly. Karyotyping after TOP revealed trisomy 18. The main message of the case is that a systematic approach in the evaluation of the face in the first trimester can help us in diagnosis beyond the immediate anatomical defect – in this case, a trisomy.
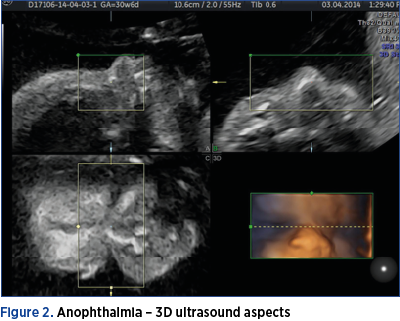
Case 2: Anophthalmia
A tertiparous patient, 42 years old, presented to our unit for uterine contractions at 30 weeks of gestation. Due to personal reasons, the patient had never had a previous scan before, the current presentation being the first one during the pregnancy. The ultrasound assessment revealed the absence of the orbits and ocular lenses. For proper counseling, we used 3D techniques – 3D surface rendering mode – to offer a better understanding of the diagnosis. Anophthalmia represents the hypoplasia of variable degrees of the bony orbit and the eye bulb. It can be unilateral or bilateral, in most cases being part of a severe chromosomal or nonchromosomal syndrome. The ultrasound diagnosis is made on the axial view at the level of the orbits. Bilateral anophthalmia is syndromic in most of the cases, with a very poor prognosis(1).
The counseling of this case had no particular challenges, because at this gestational age no changes in the management of the pregnancy was possible according to the legislation. However, the use of standard approach in the screening of the fetal face, even in the third trimester, can help us avoid missing important anomalies such as this one, while the use of additional techniques, such as 3D or 4D, can help us communicate better with the patient. This type of diagnosis implies an emotional challenge and a clear image was helpful in accepting the situation.

Case 3: Pierre Robin syndrome
A pregnant woman was referred to our department for a mid-trimester anomaly scan. The patient had a normal combined test performed at 11+3 weeks of gestation. The ultrasound assessment of the fetal profile revealed mild retrognathia, malposition of the tongue – with posterior localization within the pharynx, unable of reaching the lips throughout the evaluation. The mandibular bone, smaller in size, had an abnormal shape. The use of high-definition flow during swallowing suggested the presence of a posterior palate defect. Amniocentesis was performed and revealed a normal karyotype. After birth, Pierre Robin syndrome was confirmed by the pediatrician.
Pierre Robin syndrome – or, more correctly, Pierre Robin sequence – is a condition in which the infant has a lower than normal jaw, backward displacement of the tongue, and upper airway obstruction. In about 20-40% of cases, the condition is isolated(4,5), similar to our case. Although the exact cause of Pierre Robin syndrome is unknown, mutations at the level of the SOX9 gene are most frequently encountered in cases of isolated Pierre Robin sequence. However, in our case, the mutation was not found with the tests ran postnatally.
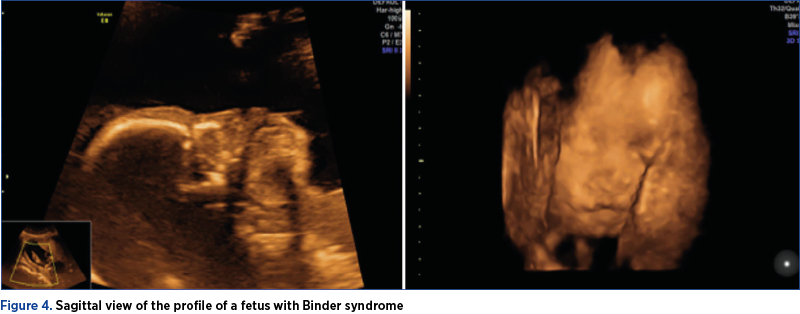
Case 4: Binder syndrome
A patient was referred to our unit for a mid-trimester anomaly scan. The ultrasound assessment of the fetal face revealed a mild facial hypoplasia, with a flat profile with a flat nasal bridge. We also detected an underdeveloped upper jaw with a protruding lower jaw. The patient had performed a quad test at 16 weeks, with all values within the normal ranges. For a better communication with the patient, we acquired 3D volumes of the fetal face. Along with these findings, we detected associated anomalies: a small membranous VSD and clubfoot. We offered the parents the possibility of karyotyping, which proved to be normal. After debating with the genetics department, we concluded that the diagnosis is most likely Binder syndrome.
Binder syndrome is a rare disease with unclear etiology and inheritance pattern. It is characterized by a developmental disorder that affects the anterior part of the maxilla and the nasal complex. Newborns with Binder syndrome have an abnormal/even absent nasofrontal angle, due to the hypoplasia of the nose, with a small tip. The nostrils are half-moon-shaped in most of the cases, the upper lip is convex, and the palate is high arched. Malocclusion and lower overbite are usually present. Although rare, prenatal detection is reported in most of the cases in the second trimester of pregnancy. However, being a rarely encountered pathology, it can be missed when using only the basic views of the standardized protocol of the fetal face. Due to the fact that Binder syndrome is not always an isolated finding and can occur in association with trisomy 21, Wolf-Hirschhorn syndrome, or it may result due to autosomal dominant transmission, karyotyping is mandatory(6).
In most of the times, these children need multiple surgical procedures and complex orthodontic treatment. After counseling, the couple decided to terminate the pregnancy.
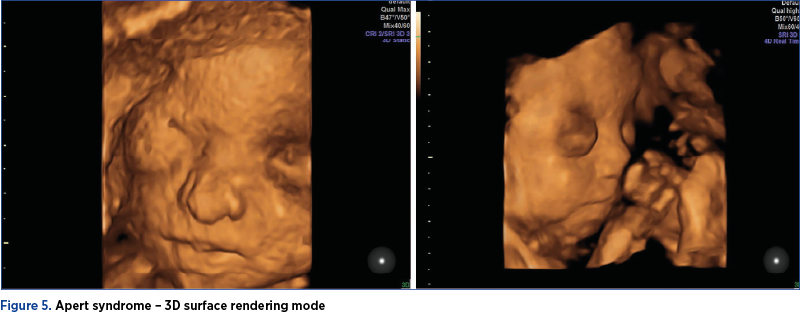
Case 5: Apert syndrome
A patient was referred to our unit for an anomaly scan and the presence of bilateral ventriculomegaly. The ultrasound assessment confirmed the ventriculomegaly, but also revealed a facial dysmorphism and clubfoot. The couple was offered genetic testing and the karyotype proved to be normal. The patient decided to ask for a second opinion in another center and continued pregnancy monitoring in the respective center until birth. Postpartum, the fetus was diagnosed with Apert syndrome, a genetic disorder characterized by skeletal malformations at the level of the skull, face, hands and feet. Apert syndrome is estimated to occur in about one in 65,000 births. A particular feature of Apert syndrome is the premature closure of the skull bones (craniosynostosis). Due to this early fusion, a normal development of the shape of the head and face is impeded. Apert syndrome is an autosomal dominant disorder caused by a rare mutation on a single gene – FGFR2 gene(7,8). In most of the cases, this disorder is diagnosed at birth or during infancy, but the prenatal diagnosis of Apert syndrome is possible in the hands of an experienced sonographer, unfortunately more frequently in the third trimester.
The lesson we learned from this case is to deal carefully with all suspected facial dysmorphism cases, and not to rely only on normal standard genetics results, such as the karyotype.
Discussion
Fetal face ultrasound assessment – and especially the use of the 3D techniques – has represented for years, both for the parents and physician, the most interactive part of the ultrasound pregnancy evaluation. In spite of this role, there has been demonstrated the clinical utility of such an approach in the evaluation of fetal facial anomalies.
Due to the development of more and more sophisticated devices, accurate sonographic diagnosis of fetal facial malformations is possible even from early gestation. Still, a conscientious scanning technique is required, as the fetal face is frequently difficult to assess owed to unfavorable fetal position.
Most national guidelines recommend for the standard basic examination of fetal anatomy only a few views of the fetal face. Therefore, subtle anomalies can be missed, creating distress to the couple. The prenatal detection rates of fetal facial malformations sharply increased since the recommendation for fetal face assessment in three sonographic examination planes: axial, sagittal and coronal. According to Rotten et al.(2), when these planes are systematically assessed, the major abnormalities detection rate increases to 88%. Consequently, we strongly recommend the use of the additional scanning planes, in order to maximize the detection rate of fetal malformations and for a better genetic counseling and investigation protocol.
Conclusions
Fetal face assessment should be an integral part of fetal ultrasound evaluation during pregnancy, when screening or targeted assessment is recommended. The detection of facial malformations can lead to the diagnosis of various genetic disorders or to pregnancy termination in case of severe defects.
Bibliografie
-
1. Paladini D, Volpe P. Ultrasound of congenital fetal anomalies. Differential diagnosis and prognostic indicators, second edition. CRC press, 2014, 97-98, 108-110, 117-127.
-
2. Rotten D, Levaillant JM. Two- and three-dimensional sonographic assessment of the fetal face. 1. A systematic analysis of the normal face. Ultrasound Obstet Gynecol. 2004 Mar;23(3): 224-231.
-
3. Nyberg DA, Sickler GK, Hegge FN, Kramer DJ, Kropp RJ. Fetal cleft lip with and without cleft palate: US classification and correlation with outcome. Radiology. 1995 Jun;195(3):677-84.
-
4. Comănescu A, Comănescu M, Hirnau M, Barbu EM, Cernea N, Sîrbu OC. Ultrasound assessment of the oral cavity – our experience. Ginecologia.ro. 2017 Dec;4 (1):18-24.
-
5. Purnell CA, Gosain AK. Pierre Robin sequence. In: Rodriguez ED, Losee JE, Neligan PC, eds. Plastic Surgery: Volume Three: Craniofacial, Head and Neck Surgery and Pediatric Plastic Surgery. 4th ed. Philadelphia, PA: Elsevier; 2018.
-
6. Levaillant JM, Moeglin D, Zouiten K, Bucourt M, Burglen L, Soupre V, Baumann C, Jaquemont ML, Touraine R, Picard A, Vuillard E, Belarbi N, Oury JF, Verloes A, Vazquez MP, Labrune P, Delezoide AL, Gérard-Blanluet M. Binder phenotype: clinical and etiological heterogeneity of the so-called Binder maxillonasal dysplasia in prenatally diagnosed cases, and review of the literature. Prenat Diagn. 2019 Feb;29(2):140-150.
-
7. Siminel MA, Neamţu CO, Diţescu D, Forţofoiu MC, Comănescu AC, Novac MB, Neamţu SD, Gluhovschi A. Apert syndrome – clinical case. Rom J Morphol Embryol. 2017;58(1):277-280.
-
8. Vieira C, Teixeira N, Cadilhe A, et al. Apert syndrome: prenatal diagnosis challenge. BMJ Case Reports CP. 2019 Dec;12(12):e231982.
Articole din ediţiile anterioare
Consilierea în agenezia ductului venos secundară venei cave inferioare întrerupte
The ultrasound (US) examination of the fetal venous system has exposed a wide spectrum of malformations.
Omfalocel, scrot bifid, hipospadias şi micropenis: rezultate clinice în cazuri cu cariotip normal
Acest studiu îşi propune să descrie caracteristicile, monitorizarea şi managementul unei malformaţii complexe: omfalocel, hipospadias, scrot bifid ...
Sarcina cicatricială după operaţia cezariană – o continuă dilemă terapeutică. Serie de cazuri şi review al literaturii
Sarcina cicatricială după operaţie cezariană (CSP) este o tulburare iatrogenă care pune viaţa în pericol, cu o incidenţă tot mai mare, din cauza cr...
Prognosticul în cazul pentalogiei lui Cantrell
Pentalogia lui Cantrell este un sindrom congenital rar, considerat letal, care asociază în forma sa completă următoarele cinci defecte: defect la n...