This case report describes a rare case of breast male cancer, a pathology with an incidence of less than 1% of all breast cancers. We hope to enrich the database around the world with our small part, because there are very few studies that report hormone-positive male breast cancer in a young patient regarding radiotherapy, but which is still, at the same time, a multidisciplinary matter. One of the difficulties of the case condition consisted in the fact that the patient was operated by sectorial excision, and we had uncertainty regarding the axillary nodal areas – the patient refused the sentinel lymph node technique and other investigations about it. For this reason, we are trying to highlight the importance of radiotherapy for achieving local control in this male breast cancer, when we didn’t know about the involvement of nodal extension of disease in this situation. The treatment plan was customized and included radiotherapy, being the one that ensures the locoregional control. The importance is given by the careful dosimetric analysis that involves all steps: precise simulation, performing a scan adapted to the patient with implications on the treatment, well defined contouring of treatment specific structures, and a good radiotherapy planning, also followed by the exact positioning each day, which can lead to better results.
Can we achieve successfully local control by IMRT radiotherapy in the treatment of male breast cancer? A case report
Putem obţine cu succes controlul local prin radioterapia IMRT în tratamentul cancerului mamar la un pacient de gen masculin? Prezentare de caz
First published: 18 decembrie 2023
Editorial Group: MEDICHUB MEDIA
DOI: 10.26416/OnHe.65.4.2023.8954
Abstract
Rezumat
Această prezentare descrie un caz rar de cancer mamar la un pacient de gen masculin, patologie care are o incidenţă mai mică de 1% din toate cazurile de cancer mamar. Sperăm să îmbogăţim baza de date din întreaga lume prin prezentarea acestui caz, deoarece sunt foarte puţine studii care raportează cancer mamar hormonal pozitiv la un bărbat tânăr, alături de aspectele privind radioterapia, fiind în acelaşi timp o chestiune multidisciplinară. Una dintre dificultăţile cazului a constat în faptul că pacientul a fost operat prin excizie sectorială, iar noi am avut incertitudini cu privire la zonele ganglionare axilare – pacientul a refuzat tehnica ganglionului-santinelă şi alte investigaţii similare. Din acest motiv, încercăm să subliniem importanţa radioterapiei pentru obţinerea controlului local în acest caz de cancer mamar la un bărbat, atunci când nu cunoaştem implicarea extensiei ganglionare a bolii în această situaţie. Planul de tratament computerizat realizat în radioterapie este personalizat, fiind cel care asigură controlul locoregional. Importanţa este dată de analiza dozimetrică atentă care implică toţi paşii: simulare precisă, realizarea unei scanări adaptate pacientului cu implicaţii asupra tratamentului, conturarea bine definită a structurilor specifice tratamentului şi o bună planificare radioterapeutică, urmată de poziţionarea cât mai exactă în fiecare zi, ceea ce poate conduce la rezultate mai bune în monitorizarea postterapeutică.
Introduction
Cancer is a major health problem and the second leading cause of death worldwide(1).
Breast cancer is the most common diagnosed cancer in women, and it is also the second leading cause of death among other types of cancer in female patients. Breast cancer detection and diagnosis have significantly improved in the last years due to the multiple screening programs implemented and the technological evolution of diagnostic techniques(2).
In the case of male breast cancer, the occurrence is very rare, constituting just one percent of the overall breast cancer cases. As to other uncommon medical conditions, conducting prospective clinical research in male breast cancer has shown to be difficult(3). Usually, male breast cancer (MBC) is identified by the presence of a painless retroareolar tumor(4).
Regarding recurrences outside the primary tumor bed, there were less than 4% after postoperative whole breast irradiation for early-stage breast cancer. As a result, the largest advantages of breast irradiation appear to arise from the dosage supplied to tissue next to the tumor site. Nonetheless, minimizing treatment morbidity while retaining radiation therapy’s potential to reduce local recurrences is a significant problem in radiation therapy treatment. To decrease toxicity without sacrificing the oncologic results, techniques such as partial-breast irradiation have been devised. Clinical oncologists can refer to precise dose/fractionation regimens and qualifying criteria based on national and international published guidelines. However, there remain several unanswered questions. Breast cancer is a multidisciplinary problem(5).
The majority of therapy options for MBC are derived from a variety of retrospective studies, clinical guidelines, or experiences in women(6). Still, there is a significant amount of variation in the clinicopathological features of MBC when compared to female breast cancer, including older age at diagnosis, more advanced stage, increased occurrence of estrogen receptor (ER) and progesterone receptor (PR) positivity, increased incidence of HER2 negative, and increased frequency of BRCA2 gene mutations(7-9). As a result, MBC patients should be evaluated and treated differently than female breast cancer patients.
Adjuvant radiation for tumors larger than 5 cm tended to enhance both relative survival and overall survival in most cases(10,11).
The aim of this article is to analyze a clinical case in a man with early-stage breast cancer who presented for radiotherapy, the premise being the analysis of the treatment plan aimed at reducing risks and increasing local control with the help of targeted radiotherapy after incomplete surgery.
Patient information
A 46-year-old male patient with right sided breast cancer, without a relevant medical history, treated in our radiotherapy department (County Emergency Hospital Craiova, Romania) was included to receive radiation therapy after incomplete surgery.
Clinical findings
The patient presented for pain in the anterior thoracic wall, particularly in the right breast region, where a small asymmetry was noted, and the clinical examination revealed a round-oval tumor about 6/4 cm, immobile compared to the underlying planes, slightly painful on palpation, for which Doppler ultrasound was performed.
Timeline

Diagnostic assessment
The patient underwent incomplete surgery – pT2NxMx. The resection limits were clear, without invasion, and with negative margins.
The result of the HP exam for this patient was infiltrative ductal carcinoma (DCI), histological type NST, grade 3.
After the HP exam, an IHC analysis was performed, resulting: HER2 = 0 (negative); ER positive in almost 75% of tumoral cells with low and moderate intensity; PR = positive in over 80% of tumoral cells with moderate intensity; Ki67 = 10-12% of tumoral cells.
Therapeutic intervention
The following step in the overall therapy was represented by polychemotherapy (PCT) – six series of epirubicin 100 + cyclophosphamide 1000 mg, followed by the recommendation of irradiation.
The overall decision of the interdisciplinary team for irradiation was taken because we couldn’t know if there was a nodal microscopical involvement, even though the CT scan after the surgery revealed no evidence of macroscopic metastatic nodal and lack of distant involvement – M0 confirmed.
Acceptable low local recurrence rates remain the primary quality assurance target. The current guidelines recommend that local recurrence rates after wide excision and radiotherapy should be below 1% per year, and should not exceed 10% overall. Postoperative radiotherapy is strongly recommended following breast conserving surgery(12,13).
The patient was treated with a TrueBeam linear accelerator with 6 MV energy and standard 120 MLC – IMRT technique.
After conservative surgery or mastectomy, intensity-modulated radiation therapy (IMRT) may result in a more favorable dose distribution for breast cancer patients than 3D CRT or traditional tangential radiotherapy (RT)(14).
We did not intend to make a thorough analysis of HP and IHC, the current purpose being centered on the treatment plan, but we integrated these data because they provide us with important information regarding the analysis of the prognosis. The current literature states that, with all therapeutic options, the prognosis of breast cancer in men remains reserved(15). Our current purpose of treatment was only to increase the locoregional control of the disease while minimizing the risk of developing locoregional relapses.
Our patient received radiotherapy between 21.06.2023 and 31.07.2023, with a total dose of 50 Gy/25 fr/day in the target volume, well supported and well tolerated.
We performed the CT scan simulation by a GE Medical Systems CT scanner, thorax protocol for breast in “free breathing” and headfirst and supine position in order to be able to subsequently perform the contouring of organs at risk on CT scan slices acquired at 0.5 cm, followed by the realization of the treatment plan according to the international guidelines(16,17).
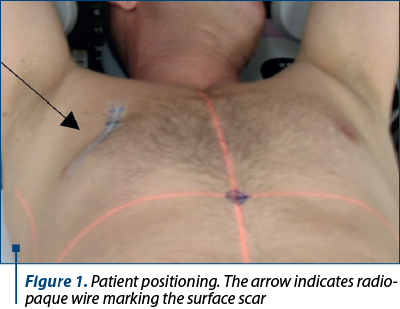
We used as containing systems breast board, upper arm supports 15° angulation left-right, and specific board for breast patients.
The head was laid in opposite directions of the irradiation volumes, also marking the surface scar with radiopaque wire, as shown in Figure 1.
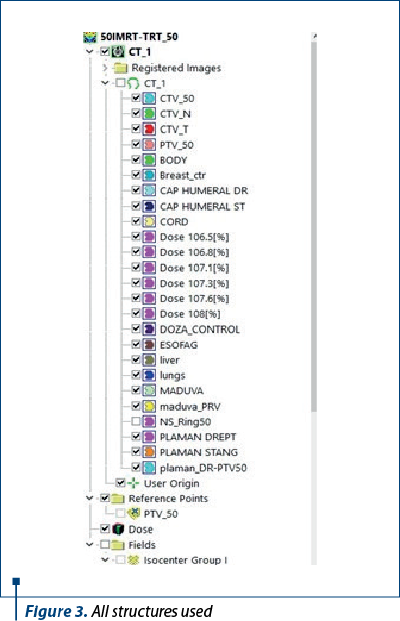
Contouring phase included axillary levels 1, 2, 3, and supraclavicular areas included in CTV_N (nodal clinical target volume), then CTV_T (the right chest wall); both CTVs were merged and formed together the CTV_50 structure and, finally, the PTV was formed by CTV_50 + 0.5 cm margin, cropped by body margin at 0.3 cm, resulting the final planning target volume, after we checked the international contouring guidelines(18).
The prescribed dose was 50 Gy in 25 fractions, as in most of FBC – 2 Gy per fraction.
First of all, there were checked the contouring and intersection axes for the alignment method, BB alignment, where three radio-opaque fiducial markers (BBs) were placed on the body intersecting with the treatment room lasers, indicating the actual intersection, the user origin defined as 0 value in x, y, z axes, as shown in Figure 2.

Then we observed the CTV and PTV delineations and checked all structures created, and we used optimization structures, entered as “ring 50” which means BODY-PTV_50 at 0.3 cm margin for helping to gather all small isodoses from all body structure and enter these small isodoses in PTV volume, and additional a lot of isodoses used in optimization for reducing the value of the hotspot. After that, we entered the dose prescription that we wanted to be delivered in PTV volume.
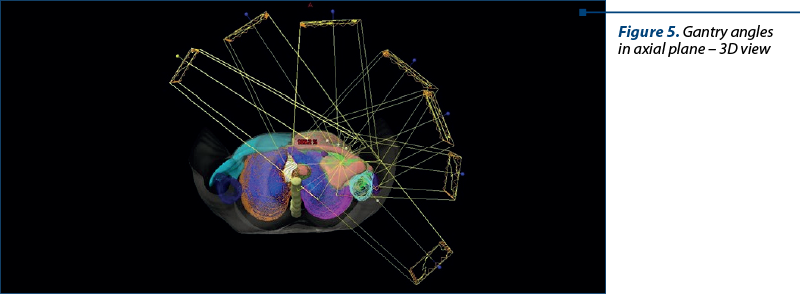
We considered to use IMRT radiation technique for this plan, using 7 beams with dynamic MLC’s leaf sequences in Eclipse TPS (Varian Medical Systems, Palo Alto, CA) version 17.0: PO optimizer 17, SMART LMC option, triple AAA algorithm (Analytical Anisotropic Algorithm).
The principle of operation of this algorithm is based on the pencil-beam kernel which characterizes the spatial distribution of radiation dosage when a highly focused beam is directed towards a water phantom, namely along the center axis of the beam. The process of correcting for inhomogeneity involves applying an equivalent route length adjustment to account for the primary dose contribution, as well as performing a one-dimensional convolution along fan lines to address the effects of dispersed radiation(14,15). The anisotropic analytical algorithm (AAA) employed by Eclipse TPS, developed by Varian Medical Systems, relies on the pencil beam convolution approach(16,17). The anisotropy analysis algorithm uses spatially distinct convolutional scattering kernels derived from Monte Carlo simulations and separate modeling of primary photons, scattered photons, and contaminating electrons. Inhomogeneities are addressed by radiological scaling of the dose accumulation function in the beam direction and electron density-based scaling of the 16 lateral photon scattering nuclei.
The final dose is obtained by superimposing the doses from photon and electron turns(18,19).
The anisotropic analytical technique presents itself as a viable choice for regular clinical application due to its comparatively efficient computational speed and accuracy when compared to the Monte Carlo approach(20).
First, we found the optimal angle for internal tangent, to be well placed not to enter in contralateral breast or heart, and we calculated the origin-to-isocenter shifts to round values for the PTV – X = 10 cm, Y = 15 cm, Z = 4.5 cm from USER ORIGIN.
Our used gantry angles were obtained after a few more tries, these being mostly dependent on the shape of PTV, body anatomy of the patient etc.
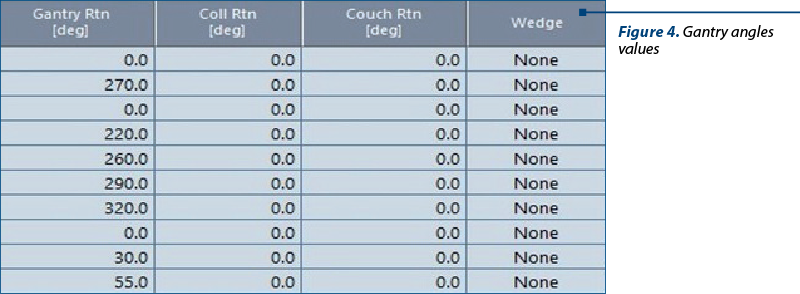
One of the firsts options was 55, 15, 340, 300, 270, 240, 200, but after a few optimizations, we swapped these values to be more optimized for specific anatomy of this male patient, for having better coverage of dose and less radiation in organs at risk (OARs).
Then we used 220, 260, 290, 320, 0, 30, 50, to have 30-40° between each beam, but for the internal tangent we observed that it is better to be smaller – 20° difference.
As it is also mentioned in literature, we chose the IMRT version with multiple angles, namely over 5, thus reaching the 7-angle version(19,20).
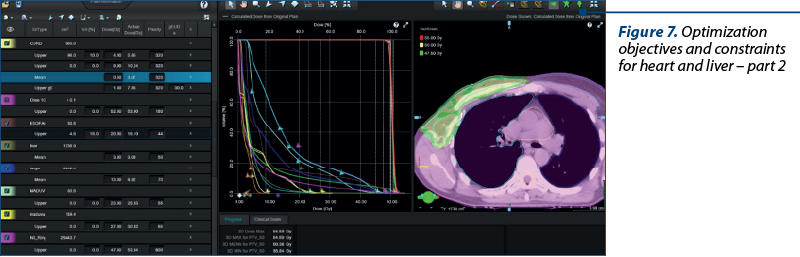
Then we started the optimization mode for plan optimization, and we entered the values as follows: OARs values and constraints for heart, lungs, the right lung and the left lung
The following dose constraints were observed in accordance with the Quantitative Analyses of Normal Tissue Effects in the Clinic (QUANTEC) criteria: for left-side irradiation, whole heart V5 ≤40-50%, V20<15%, V25<10%, and median heart dose ≤5 Gy; ipsilateral lung V20<30%, and median lung dose ≤8-9 Gy; ipsilateral humeral head V50<5%, Liver V40<30%, and Dmean <5 Gy(19).
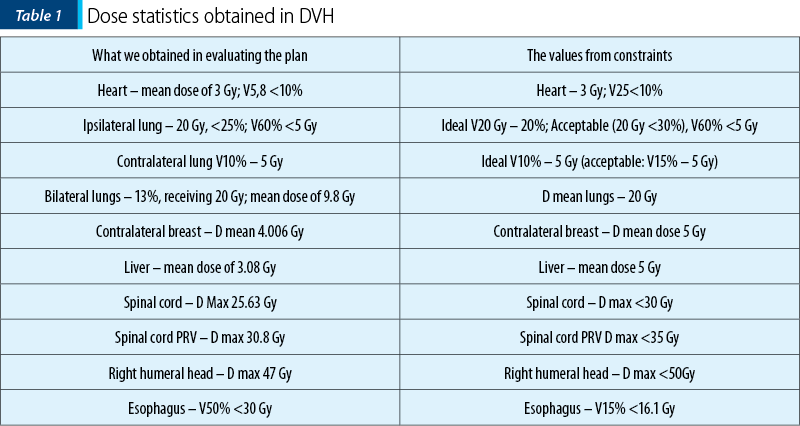
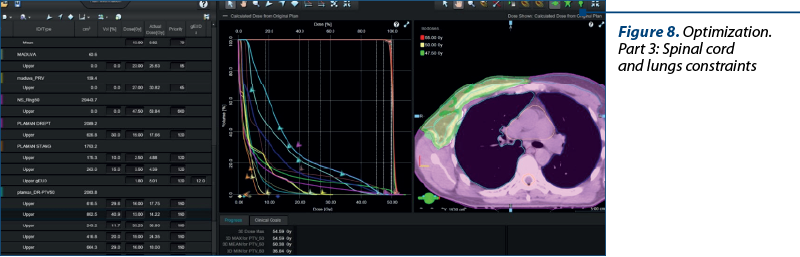
Organs at risk were the contralateral breast (left breast), heart, lungs, the lung left (the contralateral lung), the right lung (the ipsilateral lung), spinal cord, spinal cord PRV, liver and esophagus.
A conservative model (i.e., unduly safe) was applied in clinical evidence in some literature cases, which may have overestimated the danger, to predict that for partial irradiation, a V25 Gy<10% with 2 Gy per fraction will be associated with a less than 1% likelihood of cardiac mortality approximatively 15 years after RT(21).
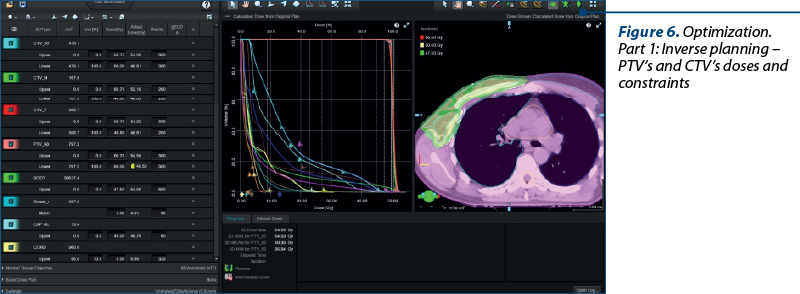
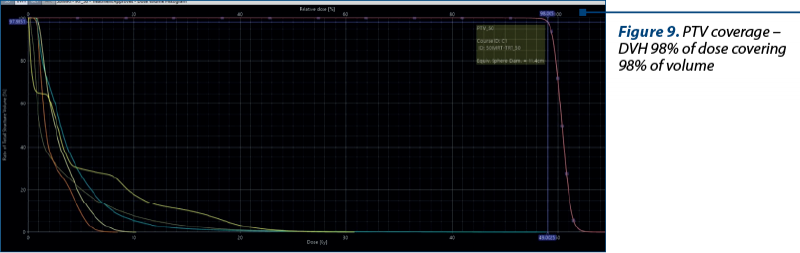
We achieved 98% of dose covering 98% of volume.
PTV checking was 98% of dose covering 98% of volume, then for the CTV_50 – 98.7% of CTV covering 98.7% of volume, slightly improved coverage for CTV; also, we checked the CTV_N, having 99% of dose covering 99% of volume.
The Conformity Index value was 0.91, close to 1. According to the RTOG definition, the Conformity Index of radiation is the ratio of the volume covered by the reference isodose, which is 95%, according to ICRU(18), to the target volume, which is known as the planned target volume (PTV), and is expressed by the equation: CIrtog = Vri/TV(23-25).
Also, we normalized the dose to 98% of dose to cover 98% of PTV, fitting into an ideal variant of the treatment plan.
We obtained a value of 109.2 hotspot, which is smaller than 0.01%, meaning that it is a virtual point with location in PTV and it can be accepted if it is smaller than 2% of PTV volume.

The institutional plan acceptability criteria are 95% target volume received at least at 95% of the prescribed dose and less than 2% volume receives ≤107%. Both conditions were satisfied for our plan(18,24).
After that, the fluence map was edited and smoothed.
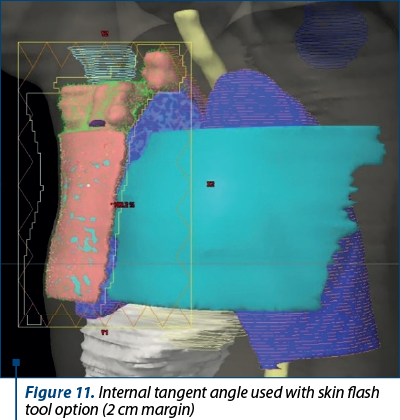
The Eclipse skin flash tool allows the planner to graphically extend the fluence outside the body surface using a paintbrush, and then fill it with transmission values. The skin flash tool visualizes the fluence of the specified field in the BEV.
After smoothing the fluence, it followed the skin flash tool by 2 cm margin from PTV for minimizing the respiratory movements of the patient.
In this instance, the results obtained met our eligibility criteria and met the proposed acceptability conditions for approval and verification of the treatment plan. Targets and dose checks for specific organs at risk were achieved.
After that we talked about the plan approval, the QA verification of the treatment plan was necessary and mandatory according to imposed international standards.
We also exported from TPS and imported and checked the RT dose to our IMRT/VMAT PSAQA – patient specific Quality Assurance – Maphan + Mapcheck 3 phantom.
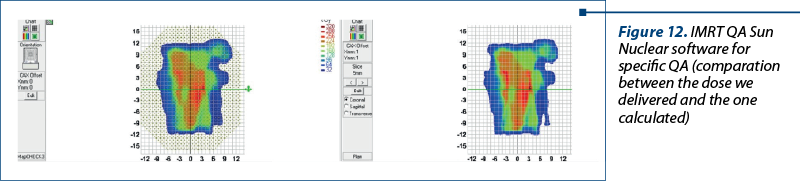
We measured in the MapCHECK 3 diode array at a water-equivalent depth of 5 cm (4.2 cm physical depth), having a high sensitivity and proven stability in a large active field size (26 cm x 32 cm), and the corresponding calculated dose planes were exported from the treatment planning system. Planar dose comparison pass rates were computed using several calculation parameters in the Sun Nuclear Corporation analytic software(26).
Gamma criteria 3% – performing the QA(26-28).
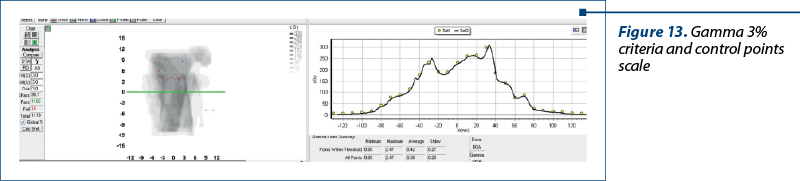
We introduced the RT dose file from plan, and we verified the actual dose by entering QA mode in our TrueBeam machine and measured the doses comparatively, resulting 98.7% pass rate.
A widely used approach for assessing the agreement between the measured and calculated doses is to compare the planar dose distribution quantitatively using the gamma index 6. The American Association of Physicists in Medicine (AAPM) generated Task Group (TG) 119, which outlined the acceptance criteria: a 3‐mm distance‐to‐agreement (DTA) for a per-field analysis and a 3% dose difference (%DD) with a global normalization method and an action level of a 90% gamma passing rate (%GP) applied with a dose threshold of 10% to remove the background noise(26-28).
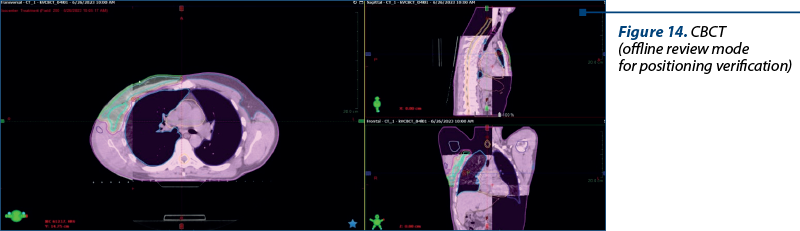
Then we started the treatment delivery and checking frequently – each day positioning of the patient till the end of radiotherapy treatment to be similar with the initial CT scan used for simulation with no major changes in reproducibility during treatment sessions.
We also used setups for imagining system – 0, 270 and 0 for CBCT before each to check the daily positioning by CBCT was as in TPS calculation with values of all delta couch values.
The patient endured radiation therapy well, with no acute side effects, only a faint erythema in the treatment area – grade 1 dermatitis.
Follow-up and outcomes
We also checked this patient three months later, when he performed a CT scan that highlighted the following: no signs of local recurrence of the disease and no nodal involvement, no metastatic findings at a distance, actually in treatment with tamoxifen.
HR positivity is the basis for successful tamoxifen therapy in male breast cancer. Data from studies comparing FBC and MBC suggest that MBC patients are largely HR-positive, and the rates of ER and PR cancers vary between 70% and 90%, respectively(30).
The patient accepted to cooperate with us from the start to help improve local evidence about breast male cancer, and he signed an information consent.
Also, through this case, we hope to manage better future breast male cancer cases in our department.
Discussion
There is a lack of randomized trials examining the efficacy of adjuvant radiation for male breast cancer and, interestingly, the majority of clinical trials about breast cancer have systematically excluded the male participants(31).
Given the limited availability of supporting data for this rare medical condition, the management of MBC closely mirrors that of female breast cancer. This includes the implementation of surgical resection, adjuvant radiation, chemotherapy and endocrine treatment, as outlined in the literature(3,6).
The current treatment options and information about the oncologic outcome mostly depend on limited retrospective studies or extrapolation from research conducted on breast cancer studies involving female subjects(6), this being the rationale for our decision to present this case. The purpose of the cases report is to determine the impact of various treatment factors, particularly postoperative radiotherapy, on short-term outcomes(6-8,31).
The data provided are derived from several studies that have demonstrated enhanced outcomes following the administration of adjuvant radiation treatment to the chest wall(10,30,31). In male breast cancer, in the early stages of the disease, radiotherapy plays a crucial role in maintaining local control, a multidisciplinary team being essential for the treatment.
We have obtained very good treatment plan results and, perhaps, not unexpectedly, we obtained, comparatively to female cases, a more easily coverage for PTV due to the anatomy of this patient.
In this case report, we try to highlight the importance of radiotherapy as a related treatment for breast cancer in male patients, whose prognosis is known to be unfavorable, ensuring a minimization of the chance of local recurrence(4-8). The creation of a personalized treatment plan is one of the most important parts of radiotherapy, which can assure a specific dose to target and help improve the local control of the disease.
Radiotherapy itself is a precise procedure including several steps and goes through a lot of well-established stages, which, if well done according to international guidelines and adapted to the patient, lead to a correct and complete treatment, after which we hope to expect a good response, thus achieving our intended objective, namely locoregional control in the case of this patient.
Post-mastectomy radiation therapy is usually recommended for men whose tumors are larger than 5 cm or affect four or more lymph nodes. It is also recommended for men with 1-3 affected lymph nodes, extensive lymphovascular invasion of the breast, or narrow surgical margins. However, the lack of specific data on men makes this determination difficult(29).
A five-year course of tamoxifen medication, combined with postmastectomy radiation therapy to the lymph nodes and chest wall area, enhances the survival(33,34).
In addition to surgery and polychemotherapy, radiation therapy plays a key role in ensuring local postoperative control, especially in the early stages, and not only in breast cancer. Each step is very important and requires a careful examination. Obviously, extended follow-up is necessary for male breast cancer patients who underwent conservative surgery and then inverse IMRT radiation therapy, given the tolerable acute toxicity and the clinical results.
Conclusions
For this rare condition, each case reported is a valued step toward a better knowledge, increased understanding and a broader database that may be utilized in future research, and we hope that this rare case of breast cancer in a young man who received IMRT radiotherapy will be a piece of the puzzle for a clearer picture of this pathology in the future.
Conflict of interest: none declared.
Financial support: none declared.
This work is permanently accessible online free of charge and published under the CC-BY licence.

Bibliografie
-
Siegel RL, Miller KD, Jemal A. Cancer statistics, 2020. CA Cancer J. Clin. 2020;70(1):7–30.
-
Libson S, Lippman M. A review of clinical aspects of breast cancer. Int Rev Psychiatry. 2014;26(1):4-15.
-
Zheng G, Leone JP. Male Breast Cancer: An Updated Review of Epidemiology, Clinicopathology, and Treatment. J Oncol. 2022;2022:1734049.
-
Forster T, Köhler C, El Shafie R, et al. Adjuvant Radiation Therapy for Male Breast Cancer-A Rare Indication? Cancers (Basel). 2020;12(12):3645.
-
Meattini I, de Oliveira Franco R, Salvestrini V, Hijal T. Partial Breast Irradiation. Breast. 2023;69:401-409.
-
Wu P, He D, Zhu S, Chang H, Wang Q, Shao Q, Li G. The role of postoperative radiation therapy in stage I-III male breast cancer: A population-based study from the surveillance, epidemiology, and End Results database. Breast. 2022;65:41-48.
-
Wang Y, Chen K, Yang Y, Tan L, Chen L, Zhu L, Su F, Liu X, Li S. Incidence and survival outcomes of early male breast cancer: a population-based comparison with early female breast cancer. Ann Transl Med. 2019;7(20):536.
-
Pritzlaff M, Summerour P, McFarland R, Li S, Reineke P, Dolinsky JS, Goldgar DE, Shimelis H, Couch FJ, Chao EC, LaDuca H. Male breast cancer in a multi-gene panel testing cohort: insights and unexpected results. Breast Cancer Res Treat. 2017;161(3):575-586.
-
Cardoso F, Bartlett JMS, Slaets L, et al. Characterization of male breast cancer: results of the EORTC 10085/TBCRC/BIG/NABCG International Male Breast Cancer Program. Ann Oncol. 2018;29(2):405-417.
-
Jardel P, Vignot S, Cutuli B, Creisson A, Vass S, Barranger E, Thariat J. Should Adjuvant Radiation Therapy Be Systematically Proposed for Male Breast Cancer? A Systematic Review. Anticancer Res. 2018;38(1):23-31.
-
Madden NA, Macdonald OK, Call JA, Schomas DA, Lee CM, Patel S. Radiotherapy and Male Breast Cancer: A Population-based Registry Analysis. Am J Clin Oncol. 2016;39(5):458-62.
-
Aebi S, Davidson T, Gruber G, Cardoso F; ESMO Guidelines Working Group. Primary breast cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2011 Sep;22 Suppl 6:vi12-24.
-
Clarke M, Collins R, Darby S, Davies C, Elphinstone P, Evans V, Godwin J, Gray R, Hicks C, James S, MacKinnon E, McGale P, McHugh T, Peto R, Taylor C, Wang Y; Early Breast Cancer Trialists’ Collaborative Group (EBCTCG). Effects of radiotherapy and of differences in the extent of surgery for early breast cancer on local recurrence and 15-year survival: an overview of the randomised trials. Lancet. 2005;366(9503):2087-106.
-
Zhang F, Wang Y, Xu W, Jiang H, Liu Q, Gao J, Yao B, Hou J, He H. Dosimetric Evaluation of Different Intensity-Modulated Radiotherapy Techniques for Breast Cancer After Conservative Surgery. Technol Cancer Res Treat. 2015;14(5):515-23.
-
Gnerlich JL, Deshpande AD, Jeffe DB, Seelam S, Kimbuende E, Margenthaler JA. Poorer survival outcomes for male breast cancer compared with female breast cancer may be attributable to in-stage migration. Ann Surg Oncol. 2011;18(7):1837-1844.
-
Offersen BV, Boersma LJ, Kirkove C, Hol S, Aznar MC, Biete Sola A, Kirova YM, Pignol JP, Remouchamps V, Verhoeven K, Weltens C, Arenas M, Gabrys D, Kopek N, Krause M, Lundstedt D, Marinko T, Montero A, Yarnold J, Poortmans P. ESTRO consensus guideline on target volume delineation for elective radiation therapy of early stage breast cancer. Radiother Oncol. 2015;114(1):3-10.
-
Ursini LA, Nuzzo M, Rosa C, et al. Whole breast radiotherapy in cN0 early breast cancer patients with pathological sentinel lymph nodes (pN1mic, pN1a) without axillary dissection: preliminary results of the observational LISEN trial. Strahlenther Onkol. 2022;198(7):612-621.
-
Hodapp N. Der ICRU-Report 83: Verordnung, Dokumentation und Kommunikation der fluenzmodulierten Photonenstrahlentherapie (IMRT) [The ICRU Report 83: prescribing, recording and reporting photon-beam intensity-modulated radiation therapy (IMRT)]. Strahlenther Onkol. 2012;188(1):97-9 [German].
-
Yang Z, Zhang L, Chen X, et al. Multibeam inverse intensity-modulated radiotherapy (IMRT) for whole breast irradiation: a single center experience in China. Oncotarget. 2015;6(33):35063-35072.
-
Jin GH, Chen LX, Deng XW, Liu XW, Huang Y, Huang XB. A comparative dosimetric study for treating left-sided breast cancer for small breast size using five different radiotherapy techniques: conventional tangential field, filed-in-filed, tangential-IMRT, multi-beam IMRT and VMAT. Radiat Oncol. 2013;8:89.
-
Gagliardi G, Constine LS, Moiseenko V, Correa C, Pierce LJ, Allen AM, Marks LB. Radiation dose-volume effects in the heart. Int J Radiat Oncol Biol Phys. 2010;76(3 Suppl):S77-85.
-
Chen WZ, Xiao Y, Li J. Impact of dose calculation algorithm on radiation therapy. World J Radiol. 2014;6(11):874-880.
-
Petrova D, Smickovska S, Lazarevska E. Conformity Index and Homogeneity Index of the Postoperative Whole Breast Radiotherapy. Open Access Maced J Med Sci. 2017;5(6):736-739.
-
Feuvret L, Noël G, Mazeron JJ, Bey P. Conformity index: a review. Int J Radiat Oncol Biol Phys. 2006;64(2):333-42.
-
Richmond ND, Turner RN, Dawes PJ, Lambert GD, Lawrence GP. Evaluation of the dosimetric consequences of adding a single asymmetric or MLC shaped field to a tangential breast radiotherapy technique. Radiother Oncol. 2003;67(2):165-70.
-
Miften M, Olch A, Mihailidis D, Moran J, Pawlicki T, Molineu A, Li H, Wijesooriya K, Shi J, Xia P, Papanikolaou N, Low DA. Tolerance limits and methodologies for IMRT measurement-based verification QA: Recommendations of AAPM Task Group No. 218. Med Phys. 2018;45(4):e53-e83.
-
Bailey DW, Spaans JD, Kumaraswamy LK, Podgorsak MB. The MapCHECK Measurement Uncertainty function and its effect on planar dose pass rates. J Appl Clin Med Phys. 2016;17(2):165-173.
-
Woon W, Ravindran PB, Ekayanake P, Vikraman S, Lim YY, Khalid J. A study on the effect of detector resolution on gamma index passing rate for VMAT and IMRT QA. J Appl Clin Med Phys. 2018;19(2):230-248.
-
Ruddy KJ, Winer EP. Male breast cancer: Risk factors, biology, diagnosis, treatment, and survivorship. Ann Oncol. 2013;24:1434–1443.
-
Eggemann H, Brucker C, Schrauder M, et al. Survival benefit of tamoxifen in male breast cancer: prospective cohort analysis. Br J Cancer. 2020;123(1):33-37.
-
Giordano SH, Cohen DS, Buzdar AU, Perkins G, Hortobagyi GN. Breast carcinoma in men: A population-based study. Cancer. 2004;101:7–51.
-
Yu E, Suzuki H, Younus J, Elfiki T, Stitt L, Yau G, Vujovic O, Perera F, Lock M, Tai P. The impact of post-mastectomy radiation therapy on male breast cancer patients - a case series. Int J Radiat Oncol Biol Phys. 2012;82(2):696-700.
-
Ionescu S, Nicolescu AC, Marincaş M, Madge OL, Simion L. An Update on the General Features of Breast Cancer in Male Patients – A Literature Review. Diagnostics. 2022;12(7):1554.
-
Lin AP, Huang TW, Tam KW. Treatment of male breast cancer: meta-analysis of real-world evidence. Br J Surg. 2021;108(9):1034-1042.
Articole din ediţiile anterioare
Cele mai importante toxicităţi ale chimioterapicelor folosite în tratamentul tumorilor solide
Principalele toxicităţi induse de chimioterapia tumorilor solide sunt: toxicitatea hematologică (anemia, leucopenia, trombopenia) şi cea nonhematol...
Cardiac toxicity of checkpoint inhibitors (CPI) used in cancer immunotherapy
Acest scurt review analizează câteva studii publicate în ultimii trei ani în întregime pe internet. Am urmărit să extragem principalele caracte...
Dependența încrucișată - prezentare de caz
Medicii oncologi sau de îngrijire paliativă întâlnesc nu o dată în cursul carierei lor pacienţi care au dezvoltat o adicţie sau o dependenţă psihic...
A case report of fulminant hepatitis due to docetaxel in breast cancer
Prezentăm cazul unei femei de 57 de ani diagnosticată cu cancer mamar metastatic, fără comorbidităţi, care a avut hepatotoxicitate severă (gradul 4...